A Murine Model of Primed Mycobacterial Uveitis to Study Post-Infectious Uveitis
Abstract
Source: John, S., et al. Primed Mycobacterial Uveitis (PMU) as a Model for Post-Infectious Uveitis. J. Vis. Exp. (2021).
This video demonstrates a method to generate a mouse model of primed mycobacterial uveitis (PMU) for studying post-infectious uveitis. Upon induction of PMU by intravitreal injection of heat-killed Mycobacterium tuberculosis in a mouse previously immunized with the same immunogen, the progression of chronic inflammation in the eye is analyzed using imaging and histopathological examination
Protocol
All procedures involving animal models have been reviewed by the local institutional animal care committee and the JoVE veterinary review board.
1. Antigen preparation for subcutaneous injection
- Perform all procedures in this section inside a chemical fume hood to prevent inhalation or skin contact with the Mycobacterium tuberculosis (Mtb) H37Ra powder. Handle according to your institutional policies for Complete Freund's Adjuvant (typically BSL-1). This includes using chemical-resistant gloves, safety glasses, and protective work clothing (lab coat).
- Use a good sterile technique to prevent contamination of reagents that will be introduced into experimental animals.
- Make the Mtb suspension in phosphate-buffered saline (PBS) by mixing 5 mg of lyophilized, heat-killed Mtb H37Ra powder with 2.5 mL of cold PBS in a 5 mL microcentrifuge tube. Vortex once for 30 seconds and then place on ice.
- To generate a fine suspension of the H37Ra in PBS, sonicate the suspension on ice for 5 min.
- Unclamp the body of the converter unit and clean the probe with a 70% (v/v) alcohol swab.
- Switch on the sonicator, adjust the power setting to 4 by turning the power control knob, and immerse the probe's tip into the PBS-containing mycobacterial powder. Ensure that the probe tip is immersed to at least half the depth of the sample and that the probe tip is not touching the wall of the microcentrifuge tube.
- Sonicate the mixture on ice for 30 seconds, pause for 30 seconds, and repeat for a total of 5 min to fully disperse the powder into an even suspension without heating the liquid.
- Add 2.5 mL of Freund's Incomplete Adjuvant to the mixture and repeat the sonication process on ice until the emulsion forms a toothpaste-like consistency.
- Set the power to 0 using the control knob and turn off the unit to end the sonication. Remove the tip from the suspension and wipe the probe with an alcohol swab.
- Store the antigen emulsion at 4 °C. Making batches of the emulsion will help ensure consistency across experiments. The emulsion can be stored at 4 °C for up to 3 months.
2. Subcutaneous injection
- Perform subcutaneous injection a week prior to the intravitreal (IVT) injection (designated as day -7).
- Load a 1 mL syringe (no needle attached) with the mycobacterial emulsion. Due to the viscosity and opacity of the emulsion, difficult-to-see air bubbles can fill the syringe.
- To prevent air bubbles in the syringe, after loading 0.2-0.3 mL of emulsion, invert the syringe (tip facing up) and gently tap the syringe repeatedly on the edge of a counter to bring the bubbles to the surface.
- Expel the air from the syringe and continue filling the syringe. Invert and intermittently tap until filled.
- Place a 25 G needle on the syringe and advance the emulsion to fill the needle. Store the syringe on ice until used.
- To perform the subcutaneous injection safely, either anesthetize the mouse or utilize humane restraint methods that allow easy access to the animal's hindquarters.
- To anesthetize for subcutaneous injection, place the animal in an isoflurane induction chamber (3%-4% for induction and 1%-3% for maintenance). Once anesthetized, ensure that the mouse has a slow respiratory rate and exhibits no signs of respiratory distress.
- Place the subcutaneous injections on either the dorsal surface of the hips or on the ventral surface of the legs proximal to the region of the inguinal lymph nodes.
- Carefully insert the needle to prevent injecting into the muscle. Inject 0.05 mL of the Mtb emulsion into the subcutaneous space. Do not remove the needle immediately in order to allow the thick emulsion to be fully injected.
- Repeat the injection on both left and right sides for a total of 0.1 mL per animal.
- If anesthetized, place the mouse on a warm heating pad until complete recovery. Do not leave the mouse unattended until it has regained sufficient consciousness to maintain sternal recumbency.
- Return the mouse to its cage upon complete recovery and label the cage card with the date of subcutaneous injection.
- Provide analgesia with oral acetaminophen (200 mg/kg/day), but not non-steroidal anti-inflammatory drugs (NSAIDs) as anti-inflammatory agents can impact the induction of uveitis.
3. Antigen stock preparation for intravitreal injection
- Perform all procedures in this section under appropriate sterile conditions to prevent contamination of the intravitreal Mtb suspension.
- Make the intravitreal suspensions.
- For induction of mild to moderate panuveitis, make the intravitreal suspension at a 5 mg/mL concentration by adding 5 mg of the mycobacteria extract to 1 mL of 1x PBS.
- For induction of moderate to severe panuveitis, make the intravitreal suspension at a 10 mg/mL concentration by adding 10 mg of the mycobacteria extract to 1 mL of 1x PBS.
- Vortex once for 30 seconds and then place on ice.
- To generate a fine suspension of the H37Ra in PBS, sonicate the suspension on ice for 10 min as described in step 1.4. Aliquot this stock solution in 100 µL volumes and store at -20 °C.
- Prior to use, thaw at room temperature and vortex on high for 1 min. Keep the aliquots on ice while transporting them to the animal facility.
4. Intravitreal injection procedure on day 0
- Animal preparation
- Wear fitted examination gloves, and place the mouse on a weighing balance to obtain its weight in grams.
- Give an intraperitoneal injection of 0.02 mL/g bodyweight of a solution containing 100 mg/mL Ketamine and 20 mg/mL Xylazine mixed with sterile water to anesthetize the animal. An alternative approach includes induction using ~1.5% isoflurane (inhaled).
- Wait approximately 2 min for the mouse to fall asleep, and then place the mouse in a warming box and cover the lid. Perform pain reflex tests like ear, toe, and tail pinch to assess the depth of anesthesia for the procedure.
- Once asleep, anesthetize the cornea with 1 drop of 0.5% (v/v) tetracaine. Avoid getting tetracaine near the nose or mouth of the mouse. After 10 s, dab off the excess liquid.
NOTE: It has been observed that iris dilation and anterior chamber (AC) visualization are improved when topical anesthesia is administered, possibly due to improved corneal reflex suppression with the combined systemic and topical anesthesia. However, this step could be omitted if desired. - Dilate the pupil with 1 drop of 2.5% (v/v) phenylephrine. Use caution to avoid any excess droplets that might enter the nose or mouth. After 2-3 min, dab off the excess liquid.
- To decrease the risk of endophthalmitis, add 1 drop of 5% betadine to the eye surface and surrounding hair. Leave on the eye for 2-3 min.
NOTE: Perform all procedures in this section under appropriate sterile conditions to prevent endophthalmitis. - Remove betadine and cover the eye with hypromellose (0.3%) or carbomer eye gel 0.2% w/w) to prevent dryness under anesthesia. This will also help prevent cataract formation.
- Setting up the microinjection system
- Perform the intravitreal injection using a micropump connected to a microsyringe pump controller and an injection syringe (Figure 1A-C). Alternatively, inject with a 33 G needle attached to a Hamilton syringe as described in subsection 4.4.
- Connect a 34 G needle to the injection holder to assemble the injector. Loosen the silver screw cap at the front end of the injection holder and slide the needle into the body of the holder about halfway. Tighten the silver screw cap finger tight.
- Connect the tubing to the injection holder as mentioned in steps 4.2.4-4.2.5.
- To insert the tubing on the injection holder, loosen the plastic screw on the back end of the holder, slide the tubing through the gasket inside, and tighten the screw.
- Maintain a slight gap with the end of the tubing to prevent tubing damage during the injection. Refer to Figure 1C.
- Thaw a 100 µL aliquot of the mycobacterium stock suspension.
- Add 3 µL of a 1% fluorescein sodium (AK-Fluor) solution and vortex well.
- Load a 10 µL syringe with the antigen and fluorescein mix without including any air bubbles.
- Remove the loading needle from the syringe, and slide the tubing through the silver screw cap gasket until the tip reaches the zero mark in the syringe body.
- Once the tip of the tubing is correctly aligned to the desired position, tighten the screw cap finger tight.
- Flush the solution in the syringe through the injection tubing to fully load the system. Then repeat steps 4.2.8-4.2.11 to reload the syringe for injection.
- To install the loaded syringe on the micropump, press the clamp release button at the end of the micro-pump to open the syringe clamps.
- Position the cap of the plunger into the plunger cap holder at the rear end of the micropump.
- Then slide the syringe collar onto the collar stop and the syringe body into the syringe clamp.
- Release the clamp button and tighten the plunger retaining screw. Refer to Figure 1D.
- Slide the injection holder and the needle through the o-clamp on the stereotactic injection apparatus. This is a custom platform; alternatively, the syringe can be held and positioned manually.
- Set the infusion volume and the rate of infusion volume on the micro syringe pump controller to inject 500 nL per cycle at a rate of 40 nL/s, respectively.
NOTE: Faster injection rates can be used, however, more reflux may be experienced before needle repositioning can be achieved. - Test the system to ensure correct functioning prior to performing an intravitreal injection.
NOTE: When the injection system is functioning correctly, activation of an injection cycle using the foot pedal or the control pad will produce visible movement of the plunger cap holder and a small droplet of greenish liquid will be seen at the tip of the needle. In the case that no liquid is produced, activate additional cycles or flush and reload the syringe. - Prior to injecting the eye, gently wipe the needle with a 95% ethanol pad.
- Intravitreal injection procedure
- The mouse is placed on a stereotaxic apparatus to perform the injection procedure.
- Keep the stage/platform on which the mouse rests warm by attaching 2-3 paper towels on its surface.
- Place the mouse in a prone position on the platform. Use the right and left ear bars to gently fix the animal's head. Refer to Figure 1E.
- Position the mouse and orient it under the scope so that the superior nasal aspect of the right eye is visible.
- Use a 30 G needle to displace the eyelashes and expose the sclera. Visualize the limbus and the radial blood vessel.
- Use a sterile 30 G needle to make a guide hole in the sclera 1-2 mm posterior to the limbus.
- Insert the 34 G needle attached to the injection holder into the eye through the guide hole at an angle that will avoid the lens, but place the needle tip into the vitreous cavity.
- Using the micro syringe pump controller, carefully inject 1 µL of the Mtb extract into the vitreous cavity. In case of consistent reflux, increase the injection volume to 1.5 µL to ensure adequate dose delivery.
NOTE: For sham controls, inject 1 µL of PBS into the eye of the animal. - Verify intravitreal placement by visualization of a greenish reflex in the eye. Refer to Figure 1F.
- After 10 s, withdraw the needle from the eye. Note any reflux.
- Remove the mouse from the platform, place 0.3% hypromellose or 0.2% w/w carbomer eye ointment on both eyes for corneal protection, and move to the recovery warming box.
- Do not leave the mouse unattended until it has regained sufficient consciousness to maintain sternal recumbency. Do not return to the company of other animals until fully recovered.
- When the mouse is fully awake, return to the cage and add acetaminophen (200-300 mg/kg/day) medicated water bottle. Label the cage card with the date of the IVT injection.
- Intravitreal injections are generally well tolerated. Clinical signs that may indicate pain and the need for removal from the study include periocular alopecia (indicative of self-trauma), corneal ulceration, weight loss, and hunched posture.
Representative Results
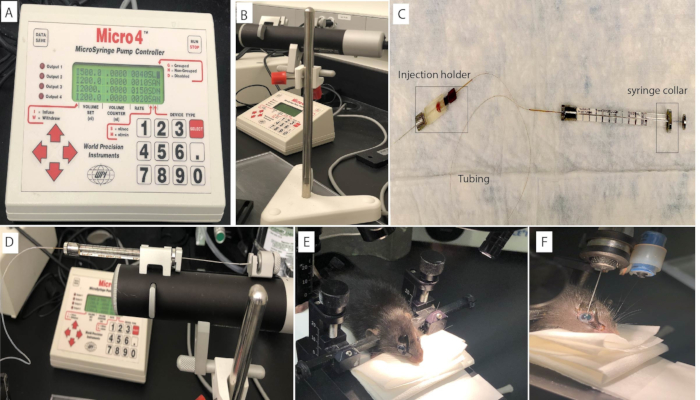
Figure 1: Mouse intravitreal injection setup. The intravitreal injection is performed on the mouse eye using (A) a micro syringe pump controller connected to the (B) Micropump and (C) an injection syringe. The syringe is loaded and mounted on the (D) Micropump. The mouse head is positioned using (E) ear bars to ensure stability and consistency during the intravitreal injection procedure. (F) Fluorescein in the injection solution produces a greenish reflection from within the eye after a successful procedure.
Disclosures
The authors have nothing to disclose.
Materials
| AK-FLUOR | Akorn Pharmaceuticals, IL, USA | 10% Fluorescein sodium 100 mg/mL in 5 mL vial | |
| AnaSed | Akorn Animal Health, IL, USA | NDC 59399-110-20 | Xylazine 20 mg/mL |
| Betadine 5% Sterile Ophthalmic Prep Solution | Alcon, TX, USA | 8007-1 | |
| B-D Precision Glide Needles -25 G | Becton, Dickinson and Company, NJ, USA | 305122 | |
| B-D Precision Glide needle -30-G | Becton, Dickinson and Company, NJ, USA | 305106 | |
| Bond MAX, Bond Rx | Leica Biosystems, IL,USA | Automated IHC staining system | |
| Chloramphenicol ointment | Martindale Pharma, Romford, UK | 1% w/w Chloramphenicol | |
| EG1150H | Leica Biosystems, IL,USA | Tissue Embedding | |
| Envisu R2300 | Bioptigen/Leica | OCT Machine | |
| Freund's Incomplete Adjuvant | BD Difco, NJ, USA | 263910 | |
| GenTeal lubricant eye ointment | Alcon, TX, USA | — | |
| GenTeal lubricant eye gel | Alcon, TX, USA | — | |
| H37Ra lyophilized Mycobacteria extract | BD Difco, NJ, USA | 231141 | |
| Hamilton RN Needle (33/12/2)S | Hamilton, Reno, NV | 7803-05(33/12/2) | 33 G |
| Hamilton syringe | Hamilton, Reno, NV | CAL7633-01 | 5 µL |
| Insulin needle | Exel International, USA | 26029 | 1 mL |
| Isoflurane | |||
| Ketaset | Zoetis, USA | 377341 | Ketamine HCL 100 mg/mL |
| Microinjection Syringe Pump and Micro4Controller | World Precision Instruments, FL, USA | UMP3 | |
| Micron IV | Phoenix Research Laboratories, Pleasanton, CA | Alternative Imaging/OCT Machine | |
| Nanofil 10 µL syringe | World Precision Instruments, FL, USA | NANOFIL | |
| Nanofil Intraocular Injection Kit | World Precision Instruments, FL, USA | IO-KIT | |
| Olympus SZX10 | Olympus | Dissection scope | |
| PBS | Gibco | 14190 | |
| Phenylephrine Hydrochloride Ophthalmic Solution USP 2.5% Sterile 15 mL | Akorn Pharmaceuticals, IL, USA | 17478020115 | |
| RM2255 | Leica Biosystems, IL,USA | Tissue Sectioning | |
| TB Syringe | Becton, Dickinson and Company, NJ, USA | 309602 | 1 mL |
| Tetracaine 0.5% | Alcon, TX, USA | 1041544 | |
| Tissue Tek VIP series | Sakura Finetek USA, Inc.,CA. | Histology Tissue Processing | |
| Tropicamide 1% | Chauvin Pharmaceuticals, Romford, UK | Minims | |
| Tylenol | Johnson & Johnson Consumer Inc, PA, USA | NDC 50580-614-01 | Acetaminophen |
| Viscotears | Novartis Pharmaceuticals, Camberley, UK | Carbomer eye gel 0.2% w/w |
