1. Animal Care and Use
Following review and approval from the Institutional Animal Care and Use Committee, male mice at least 12 weeks old are used. A mouse is anesthetized with pentobarbital sodium (60 mg/kg) via intraperitoneal (i.p.) injection. Throughout surgical procedures and experimental protocols, anesthesia is maintained by supplements (10-20% of initial injection, i.p.) as needed (every 30-60 minutes; indicated by withdrawal response to toe or tail pinch). After completion of the experimental procedure the mouse is overdosed with pentobarbital (i.p.) and euthanized by cervical dislocation.
2. Micropipettes and Microiontophoresis
- Microiontophoresis micropipettes (internal tip diameter, ˜1 μm) are prepared from borosilicate glass capillary tubes using a horizontal pipette puller. Ours have a ˜5 mm taper for stiffness; longer tapers are more flexible.
- Micropipettes are backfilled with 1M ACh (Figure1A-C) dissolved in 18.2 MΩ water. For backfilling, a microcapillary tube is connected to 0.2 μm filter coupled to a syringe containing the agonist of interest (Figure 1). These can be readily fabricated (below) or purchased from commercial vendors. The microcapillary tube is inserted into the back end of the micropipette and ACh solution is delivered into the lumen while withdrawing the microcapillary tube as the micropipette fills. Holding the micropipette with its tip pointing down, air bubbles are removed by gently flicking the micropipette.
- The micropipette is secured in a holder mounted in a micromanipulator (Figure 2). The holder has a silver wire connecting the ACh solution within the micropipette to an external pin, which in turn is connected to the positive terminal of a microiontophoresis programmer. A second silver wire secured at the edge of the tissue preparation is connected to the negative terminal to complete the circuit as the tip of the micropipette is advanced into the physiological saline solution over the preparation.
- A retaining current is applied to prevent vasodilation (or fluorescent response) when the micropipette tip is positioned adjacent to the arteriolar wall. Retaining current will vary with the size of the micropipette tip (internal diameter = 1 μm) and agonist concentration but is highly reproducible for defined parameters (we use ˜200 nA for 1M ACh, 1 μm tip). The retaining current ceases coincident with delivery of ejection current via the electronic trigger (Supplementary Figure 1) synchronized with the onset of image acquisition.
3. Micromanipulation
- A custom platform for an X-Y microscope stage was fabricated out of ferromagnetic stainless steel. Platform dimensions (1/8″ X 12″ X 13″) enable sufficient space to position micromanipulators around the experimental preparation as desired (Figure 2A). Micromanipulators secured to magnetic bases (Figure 2B) enable positioning as dictated by the preparation. These are placed directly on the fabricated platform around the preparation for positioning micropipettes at sites of interest (Figure 2C).
4. Representative Results
- With the micropipette tip positioned adjacent to an arteriole, there is fluorescence response to ACh (retaining current than adjusted to prevent ACh leakage). Below a threshold stimulus there was no effect. However, as stimulus intensity increased, endothelial cell calcium fluorescence increased over progressively greater distances along the arteriole, as did the intensity of fluorescence at the site of stimulation (Figure 3).
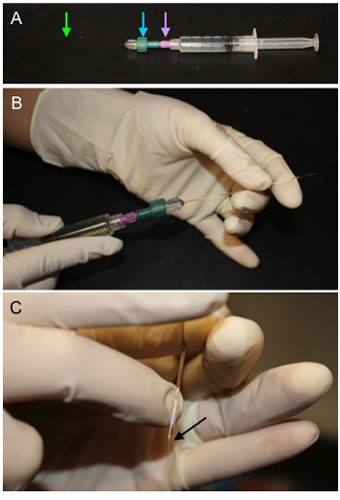
Figure 1. Method for Backfilling Microiontophoresis Pipettes. A) A microcapillary tube (green arrow) is secured in a compression fitting (blue arrow)
attached to a 0.2 μm filter (purple arrow) which is then attached to a syringe filled with 1M ACh. B) The microcapillary tube is fed into the
microiontophoresis pipette through the back end and solution is displaced to fill the lumen of the micropipette. C) Once the pipette is filled, hold the tip
down and gently flick above the taper to remove bubbles (black arrow).
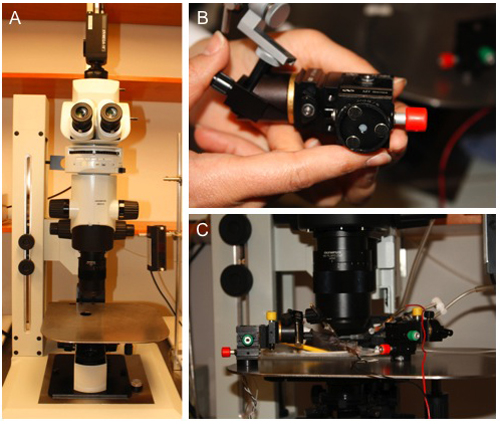
Figure 2. Custom Platform for Micromanipulator Placement. A) A ferromagnetic stainless steel platform was placed on a custom MVX10 microscope base
containing an X-Y translational stage. B) Circular magnetic bases affixed to the bottom of compact 3-axis micromanipulators. C)
Micromanipulators positioned around the experimental preparation (See associated protocol: JoVE ID#2874) to study specific sites of interest. Their
compact size and versatility enable multiple micropipettes to be used simultaneously.
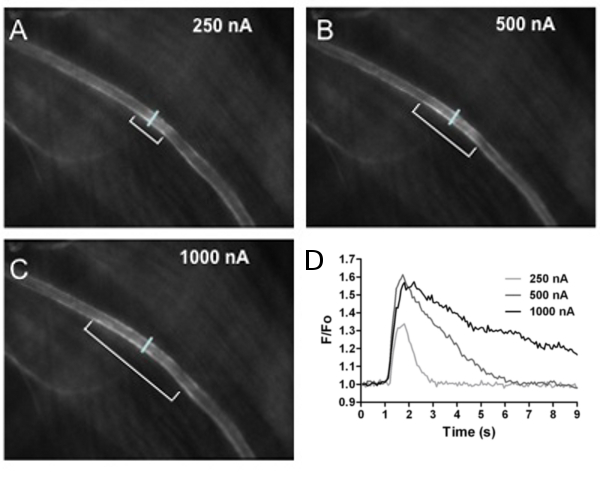
Figure 3. Calcium Fluorescence in Arterioles. Calcium fluorescence of endothelial cells lining the arteriolar wall increased with stimulus intensity.
The first 3 panels shown images of fluorescence responses to A) 250 nA, B) 500 nA and C) 1000 nA ejection current (all 500 ms pulse duration). The distance over which
endothelial cell calcium fluorescence increased is indicated by brackets in A-C (˜130, 270 and 400 μm, respectively). The reference line across the arteriole in each
panel indicates where fluorescence responses (F/Fo) to ACh were recorded at the site of stimulation. D) Recordings of F/Fo vs. time for increasing ACh stimuli. As
ejection current increased, F/Fo increased in amplitude and duration. Note that 100 nA stimulus was below threshold and had no effect.

Supplementary Figure 1. Circuit diagram for electronic trigger. This circuit is interfaced with a parallel port from a personal computer. When activated it provides a constant TTL pulse of 5V. The 7805 chip is a 5V voltage regulator connected to a 9-12V DC power supply (a battery of appropriate voltage is fine). Output from the 7805 provides power to the Quad Bilateral Switch and to the output of the circuit. Input across the 1K resistor is from the computer.
