Example of NIRF Lymphatic Imaging in Mice
When ICG or cABD-IRDye800 is injected ID at the base of the tail of a normal mouse, the lymphatic vasculature between the injection site at the base of the tail and the inguinal lymph node (LN) should be immediately visualized. Shortly after injection (a few seconds to minutes), the lymphatic vessel between the inguinal LN and the axillary LN should be visualized as seen in Figure 2. Since the lymphatics in mice vary from animal to animal as they do in humans, variation in architecture between animals may be seen as shown in Figure 3. When ICG or NIRF-cABD is injected ID on the dorsal aspect of the hind paw of a normal mouse, two lymphatic vessels can be visualized draining to the popliteal LN as shown in Figure 4. In some cases, it is difficult to distinguish both vessels because of their close proximity with each other.
Precautions for NIRF Lymphatic Imaging Impacted
At times, visualization of the lymphatics is delayed, most commonly due to the injection being administered subcutaneously (SC) instead of ID. When SC injections are given, lymphatic transport may not be immediately visualized as seen in Figure 5(a) because of the additional time required for the dye to reach and be taken up by the lymphatic capillaries in the skin. This is why it is important to inject ID instead of SC. On occasion, abnormal lymphatic vessels are observed, as seen in Figure 5(b), in the area of a wound such as a bite or cut from the hair/fur clippers. The animal’s body temperature should be maintained within normal range, as changing body temperature can result in inconsistent lymphatic function. Limitations of the technique include obscuration of fluorescent lymphatic vessels by skin pigmentation, the inability to image the deep thoracic lymphatic ducts due to light scattering in the tissue, and the unknown effect of anesthesia on lymphatic function.
Generally, it takes the ID depot of ICG or cABD-IRDye800 up to 2 days to clear the liver and bladder, and up to 3 days to clear the injection site. When residual fluorescent signal has cleared, the imaging protocol can be repeated, allowing longitudinal lymphatic imaging to evaluate changes in architecture or lymph function after some intervention.
Analysis of Lymphatic Function
The acquired images can be loaded into ImageJ or MATLAB for data analysis. Constant-area, circular ROIs are selected or “drawn” along the entire length of the fluorescent lymphatic vessel as done for human10 and animal5 lymphatic imaging as shown in Figures 6(a) and Figure 6(d). The ROIs are selected such that their diameter is approximately the diameter of the image of the fluorescent vessel. The mean fluorescence intensity within each ROI is plotted as a function of imaging time to assess the propulsive velocity and the frequency of “packets” of dye-laden lymph propelled along the lymphatic vessels as shown in Figures 6(b) and Figure 6(e). To assess the lymphatic propagation velocity and frequency of lymphatic propulsion, two ROI’s, with clearly defined maxima or minima fluorescent intensity variations representing the propagation of packets of lymph, are selected and their fluorescent intensity profiles are plotted as shown in Figures 6(c) and 6(f). The propagation velocity is computed by taking the ratio of the distance between the two ROI’s and the transit time for a packet of lymph to propagate between them. By assessing the number of fluorescent pulses or “packets” arriving at a single ROI per time, the contractile frequency is computed. While this technique provides the only method to assess propulsion frequency and velocity of a propelled lymphatic “packet,” others have indirectly evaluated lymphatic transport by measuring the depot clearance of an imaging agent and thus calculating removal rate constants11. In cancer metastases10 and early infection, we find loss of lymphatic propulsion in animals. Others report changes in contractility in response to arthritis12. In humans, we report increased propulsion following lymphedema treatments including pneumatic compression drainage13 and manual lymphatic drainage (massage)14.
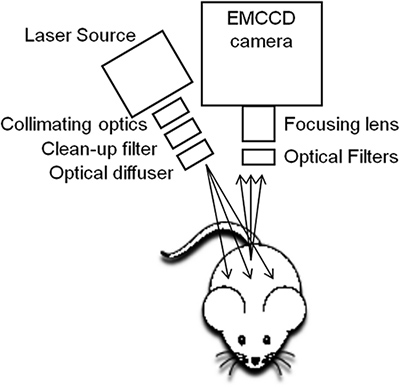
Figure 1. The NIRF imaging system is custom-built for small animal lymphatic imaging. The device consists of a 785-nm laser diode outfitted with an aspheric lens, diffuser, and filters to create a uniform excitation field that illuminates the animal and an EMCCD camera, focusing lens, and optical filters to capture images of fluorescent lymph10.
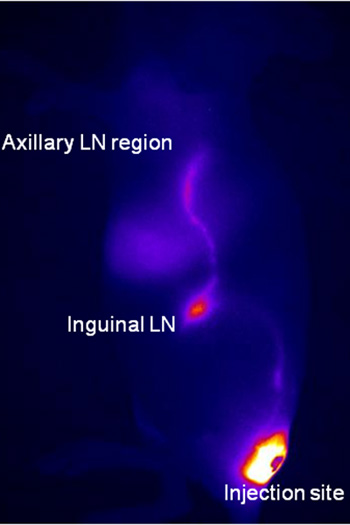
Figure 2. When 10 μl of ICG or cABD-IRDye800 is injected ID at the base of the tail of a normal mouse using a 31-gauge needle, the lymphatic vasculature between the injection site at the base of the tail and the inguinal lymph LN should be immediately visualized. Dynamic fluorescence images are acquired immediately after injection and for up to 20 min following injection. Shortly after injection (a few seconds to minutes), lymphatic vessels between the injection site and the inguinal LN and subsequently to the axillary LN region are visualized on the lateral view. The image shown in Figure 2 was taken 5 min. after injection with 10 μl of ICG ID at the base of the tail. The bright spot between the inguinal and axillary regions is the liver.
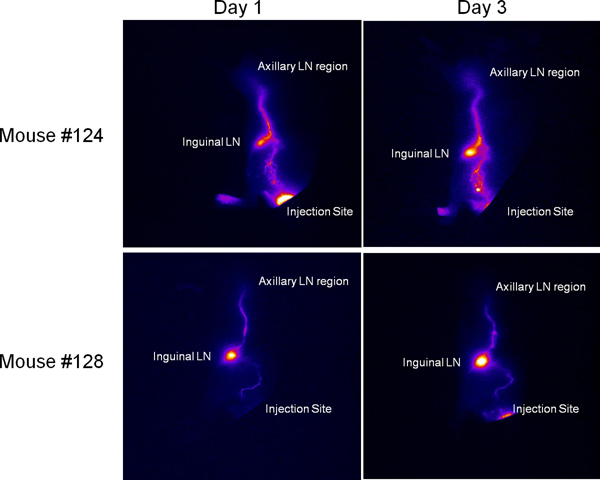
Figure 3. Since the lymphatics in mice vary from animal to animal as they do in humans, variation in architecture between animals may be seen and is stable over time. Mouse #124 was injected with ICG at the base of the tail and imaged immediately on day 1. The top panel contains the image obtained at day 1 as well as an image obtained 2 days later (on day 3) using the same mouse and injection/imaging protocol. The bottom panel contains images obtained from another mouse (#127) injected with ICG and immediately imaged day 1 and subsequently imaged on day 3. While the lymphatic architecture (the pattern of lymphatic vessels) varies between mouse #124 and #127, the images obtained using NIRF are consistent for each mouse on days 1 and 3.
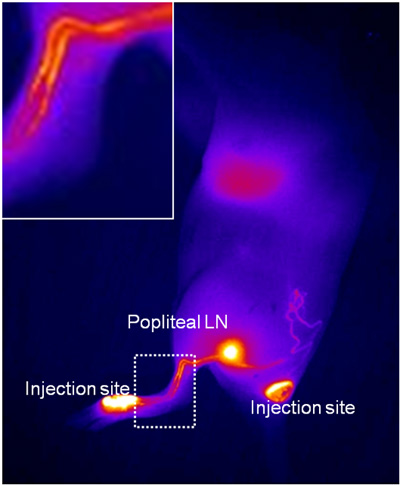
Figure 4. When 5-10 μl of ICG or NIRF-cABD is injected ID on the dorsal aspect of the hind paw of a normal mouse, two lymphatic vessels should be visualized draining to the popliteal LN. Dynamic fluorescence images are acquired immediately after injection and for up to 20 min following injection. In some cases it is difficult to distinguish both vessels because of their proximity as illustrated in the enlarged image represented by the dashed box. For the representative mouse shown here, 10 μl of ICG was injected in the dorsal aspect of the left, hind paw (first injection site) and in the left side of the tail base (second injection site). This image was captured approximately 2 – 3 min after the first injection and approximately 30 sec – 1 min following the second injection.
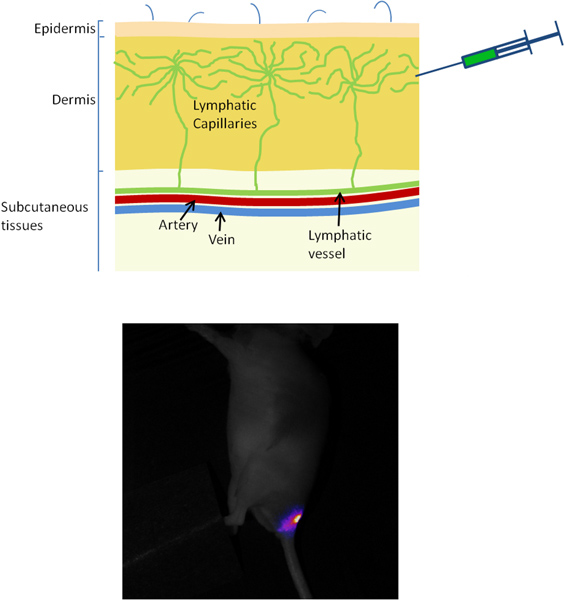
Figure 5. (a) Occasionally visualization of the lymphatics is delayed or impaired, most commonly due to the injection being administered SC instead of ID. When 10 μl of ICG or cABD-IRDye800 is injected SC at the base of the tail of a normal mouse using a 31-gauge needle, lymphatic transport will not be immediately visualized because of the additional time required for the dye to reach and be taken up by the lymphatic capillaries in the skin. Also, due to the relatively deep SC injection, there may be no lymphatic uptake and therefore no visualization of the vessels and lymph nodes. In Figure 5(a), a mouse was injected with 10 μl of ICG at the base of the tail SC and images were acquired 5 min after injection. The dye at the injection site can be visualized and no lymphatic vessels or lymph nodes can be visualized. This is the reason ID injections are important. (b) Visualization from animal’s ventral side of aberrant lymphatic vessels resulting from a wound encountered one day earlier during fur removal with clippers (tissue injury site noted on animal’s right side). The image was captured approximately 5 min after 10 μl of ICG was administered ID at the base of the tail on each the left and right side. On the non-injured (animal’s left) side, the inguinal LN can be visualized as well as the relatively straight efferent lymph vessel draining up toward the axillary LNs. On the mouse’s right side, however, normal lymph vasculature was interrupted due to wounding and appears aberrant due to tissue repair (scabbing).
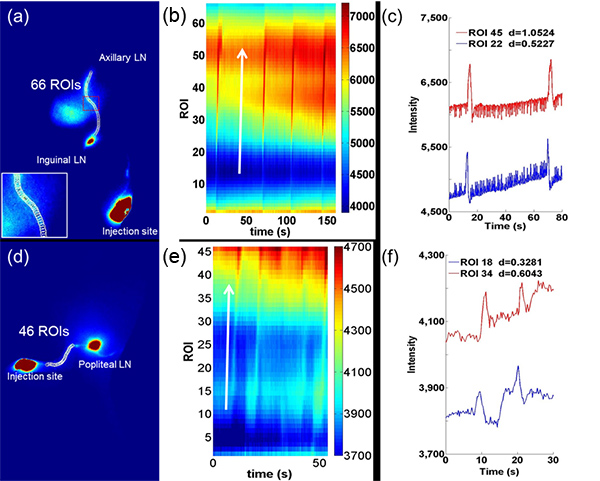
Figure 6. Quantitative analysis of lymphatic contractile function consists of selecting ROIs along the lymphatic vessels draining from (a) the inguinal LN to the axillary LN and (d) the injection site on the dorsal aspect of the paw to the popliteal LN. A magnified image (inset in (a)) of the red dashed rectangle illustrates the selection of ROIs along the fluorescent vessel. A compilation of average fluorescence intensity as a function of time for all ROIs from (a) and (d) is represented by the pseudo-color plot shown in (b) and (e), respectively. The perturbations in fluorescence intensity across pixels represent a lymphatic “pulse” propagating through the ROIs and are parallel to the arrows. The average fluorescence intensity for single ROIs 22 and 45 from (b) are shown in (c) and the average fluorescence intensity for single ROIs 18 and 34 from (e) are shown in (f). Fluorescence intensity profiles as a function of time (as shown in (c) and (f)) facilitate the identification of packets of propagating lymph and the extraction of the transit time and distance between two ROIs. The two ROIs are selected based in part on their location along the lymphatic vessel and the clarity with which the maxima and minima representing lymph propagation are shown. Velocity is computed as the ratio of the distance between two ROIs and the transit time that is taken between peak fluorescence intensity. Click here to view larger figure
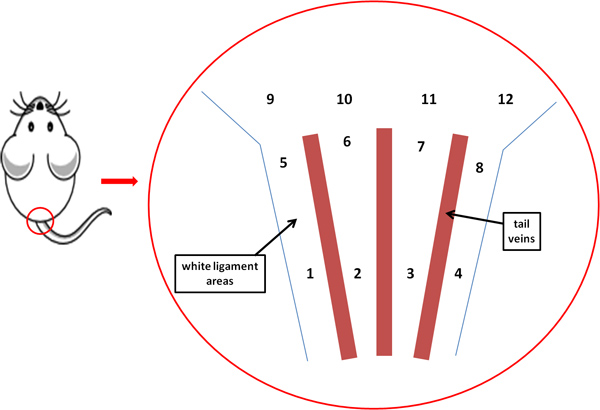
Figure 7. To visualize the lymphatics draining from the inguinal region to the axillary region, inject the left or right side of the base of the tail. In general, to visualize the left side, inject in location 5, 6, 9, or 10; and to visualize the right side, inject in location 7, 8, 11, or 12. Locations 1 through 4 may be too inferior on the tail for optimum uptake to visualize lymphatic drainage from the inguinal region to the axillary region.
