Transient MCAO (60 min) was induced by inserting a silicone-coated filament in the external carotid artery. The filament was then pushed through the terminal end of the internal carotid artery up to the origin of the MCA, under LD monitoring. Common carotid artery and pterygopalatin artery were transiently occluded during the surgical insertion of the filament. A schematic representation of the surgical procedure is shown in Figure 1A.
The cranial coordinates for positioning the two LD probes were chosen according to the underlying arterial territory. Preliminary experiments with gelatin-ink perfusion (Figure 1B) showed that the ischemic core is expected in the central MCA territory (bregma -1 mm, 5 mm from midline; Probe 1), while the collateral flow is expected in the borderzone territory between the cortical branches of middle and anterior cerebral arteries (bregma +2 mm, 2 mm from midline; Probe 2).
Cerebral hemodynamics was studied using multi-site Laser Doppler probes during the entire period of the surgical procedure, i.e. before, during and after MCAO (Figure 2). The cerebral perfusion deficit during MCAO was smaller and showed a higher degree of variability in Probe 2 compared to Probe 1, suggesting inter-individual differences in the functional performance of intracranial collaterals under ischemic conditions. The multi-site Laser Doppler monitoring also allows to study the cerebral hemodynamic changes during the occlusion of proximal extra-cranial cerebral arteries (common carotid artery, internal carotid artery, pterygopalatin artery).
Stroke outcome was assessed 24 hr after reperfusion by infarct volume, calculated on 19 consecutive sections stained with Cresyl violet (Figure 3), and Garcia functional neuroscore11. Immunohistochemistry for specific markers associated with ischemic brain injury was performed, in order to obtain a topographical distribution of neuronal loss (microtubule associated protein 2, MAP2) and ischemic penumbra (heat shock protein-70, Hsp70) in relation to the multi-site hemodynamic monitoring of intracranial circulation (Figure 4).
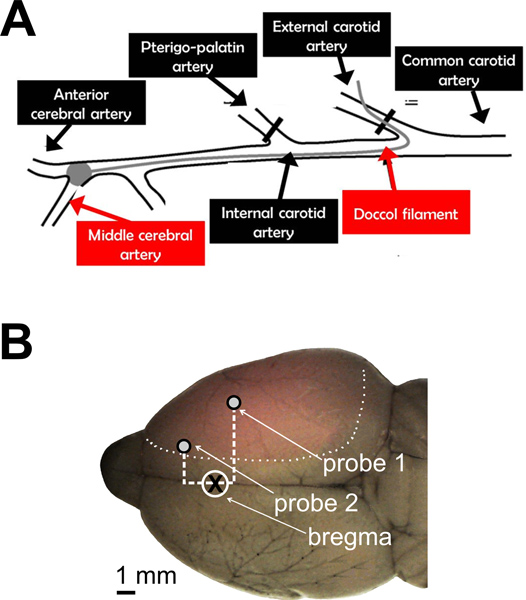
Figure 1. Cerebral perfusion monitoring during intraluminal MCAO in the rat. A. Schematic representation of the surgical procedure for transient MCAO. A silicone-coated filament was used to occlude the origin of the MCA, after being introduced in the external carotid artery and pushed through the internal carotid artery. Proximal cervical arteries were either ligated (external carotid artery) or transiently occluded (pterygopalatin artery and common carotid artery) during the procedure. B. A representative brain is shown after gelatin-ink staining. Transcardiac perfusion of gelatin-ink solution were performed 60 min after the onset of ischemia, without reperfusion. The normally perfused brain was stained by gelatin-ink and appeared as grey-colored with black stained vessels, while the ischemic (not-perfused) area remained unstained (pink-colored). Cranial coordinates for positioning the two LD probes are shown. Probe 1 = -1 mm from bregma, 5 mm from midline; Probe 2 = +2 mm from bregma, 2 mm from midline.
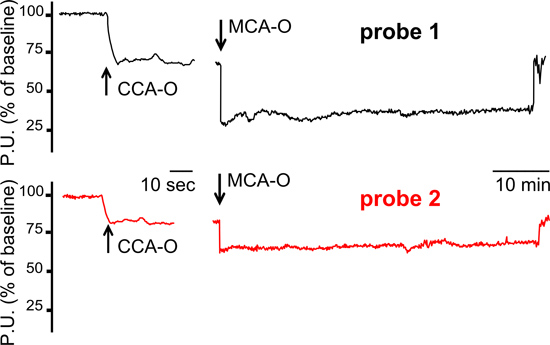
Figure 2. Cerebral hemodynamic recordings using multi-site Laser Doppler probes. A typical hemodynamic pattern which suggests functionally active intracranial collaterals under ischemic conditions is shown. In this animal, LD tracings showed a smaller perfusion deficit in Probe 2 channel, compared to Probe 1 channel, during both CCA occlusion and MCA occlusion. MCA-O=middle cerebral artery occlusion. CCA-O=common carotid artery occlusion. P.U.= perfusion units.
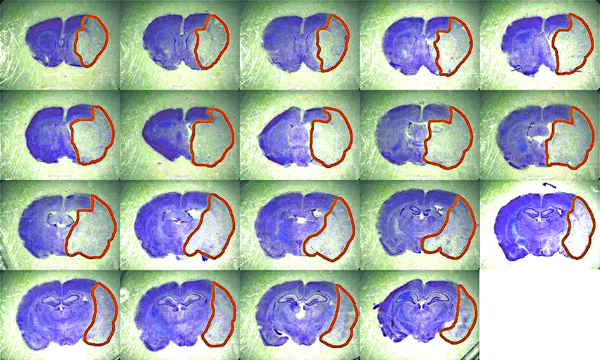
Figure 3. Representative brain sections for the calculation of infarct volume. Histological coronal sections (50 μm; n = 19 with 250 μm interval; bregma +2.5 mm to −3.0 mm) are fixed in 4% paraformaldehyde and stained with Cresyl violet 0.1%. Infarct volume is calculated using ImageJ image processing software, corrected for inter-hemispheric asymmetries due to cerebral edema, and expressed in mm3. Click here to view larger figure
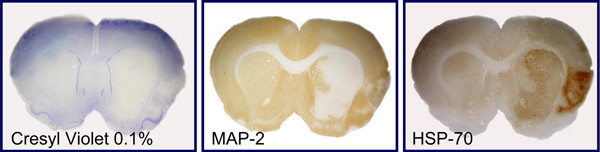
Figure 4. Immunostaining of molecular markers of neuronal loss and penumbra. Representative consecutive brain sections are shown, which were stained with Cresyl violet 0.1% (A) or immunostained with markers of neuronal loss (microtubule associated protein 2, MAP2; B) and ischemic penumbra (heat shock protein-70, Hsp70; C).
