The protocol and images presented in this study were prepared with an Olympus URF-V flexible endoscope14 and NBI11,15. Video images were saved in MPEG-2 format and pictures in JPG, TIF, PNG, or DICOM format with maximum 1,280 x 1,024 pixels, transferable to standard USB flash portable memories. NBI enhances the visual contrast of hemoglobin-containing tissues. Normal light and NBI imaging are key features to illustrate the normal anatomy of the colorectal mucosa and the differences between normal and abnormal vascularization during ulceration and tumor development (Figures 3A and 6A). Images with methylene blue as contrast medium during chromoendoscopy show its benefits for close-up images, revealing the aerial normal honeycomb appearance of the colonic crypts (see close up in Figure 3B).
To date, we have conducted over 500 murine endoscopies following this protocol, with about 10% representing repeated examination. Generally, the procedure requires 10-15 minutes to complete, split evenly between administration of anesthesia, endoscopy, and recovery from anesthesia. The examination covers from the anus to the splenic flexure of the distal colon. We have also successfully conducted postmortem endoscopic examinations of the proximal colon, cecum and ileum in some cases, following postmortem dissection of the tissues immediately prior to harvesting tissues for histology (Figure 6B). In one case, we also observed and confirmed suspected gastric dilation in a mouse affected with severe duodenal stricture and impaction due to intestinal adhesions. The abnormal image was observed transmurally from the most cranial aspect of a mildly inflamed distal colon; postmortem examination showed the distended stomach was juxtaposed to the colon.
We have developed a valid and reliable decimal-weighted scoring system to improve the standardized application of murine endoscopy across published research studies. Three scoring systems have been previously employed and served as the foundation for the development of our decimal-weighted system4-6. Although these systems allow for the categorization of various criteria and levels of lesion severity, they lack proper criteria definitions, some of which are difficult to evaluate from endoscopic images. In some cases, ambiguous parameters included in the scoring systems have questionable relevance to endoscopic examination in mice. A summary of eleven published parameters4-6 and their endoscopic advantages, limitations, and physiological relevance are presented in Table 1.
Because the proposed murine colonic endoscopy scoring system will be used for research purposes, its usefulness for performing statistical inference was essential. To assure that the scoring system had high construct validity, we first developed a conceptual framework to identify relevant parameters, grouped these parameters to fewer criteria (n=3), and assessed their colinearity and correlation with actual presence of inflammation and healing (Figure 7). Next, we added perianal findings using discrete integers to represent ordinal levels of severity, and integrated the concept of tumor induction and development using decimal identifiers. In addition, we added ‘strictures’ as another parameter not previously considered/reported in murine intestinal endoscopy. The resulting output scores produce high validity and are suitable for parametric statistical analysis. Lastly, we added mapping and numerical plotting capabilities for detailed disease monitoring.
To assess the convergent validity of our assessment system, the scores obtained from three published parameters for 36 mouse colonoscopies were compared against the scores obtained by the same person blindly using three previous scoring systems4-6. Every comparison showed good positive correlation, indicating high convergent validity for our integrated scoring system (Pearson p<0.0001; Figure 8). The analysis supports the inclusion of perianal findings as part of the clinical criteria to assess colorectal health, as it was commonly present in cases of severe colitis and improved data dispersion (P=0.0351 between score 0 and 1, P=0.0086 between score 2 and 3, Figure 8B). When the integrated scoring system (after adding perianal findings) was compared to the other available systems, it was evident that 2 of the 3 other systems have a major inferential limitation due to clustering of cases to one of the four possible integer categories, a major indication of method misclassification bias (Figure 8C)16. With decimal identifiers, our novel scoring system has the lowest probability of clustering data points in integer categories.
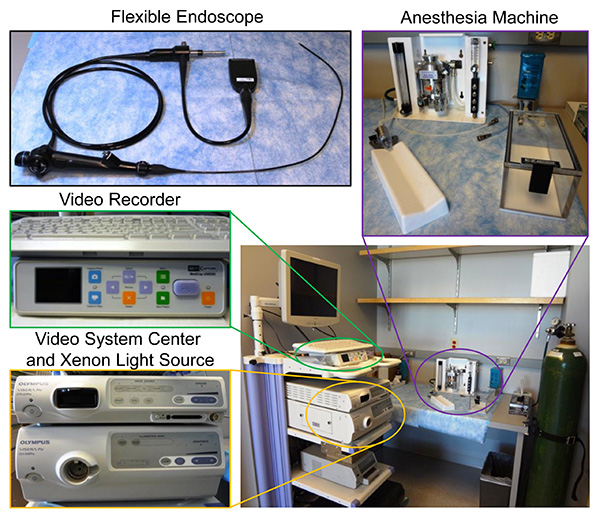
Figure 1. Instruments. Flexible endoscope, video control system, light source, video recorder, and inhalation anesthesia machine used in this study. Click here to view larger image.
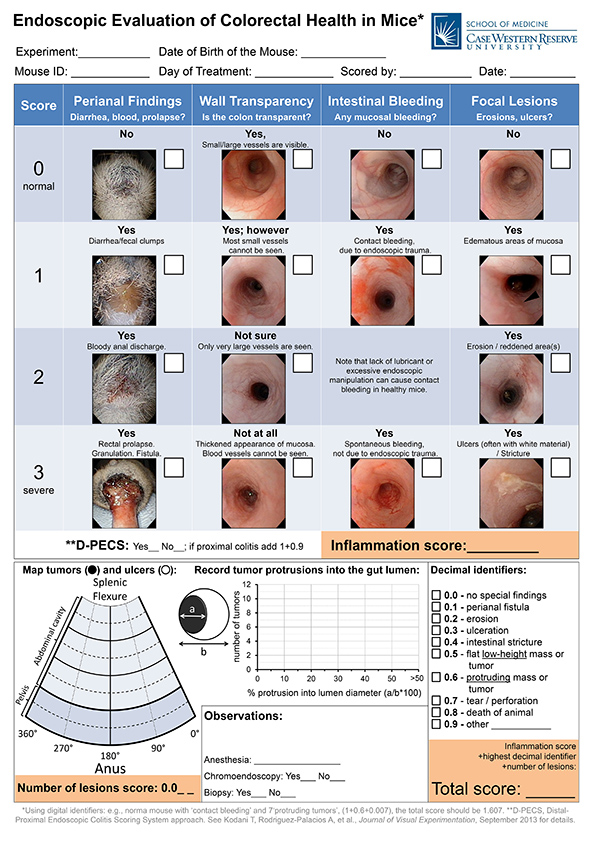
Figure 2. Decimal scoring system form for assessment of colitis and colorectal tumors in mice. The system has a core inflammatory component of four non-co-linear parameters, graphics for tumor information, and decimal units to notable lesions or complications. See detailed criteria and examples in section below (Endoscopic Assessment of Murine Colorectal Inflammation and Tumors Using a Decimal-weighted Scoring System). Click here to view larger image.
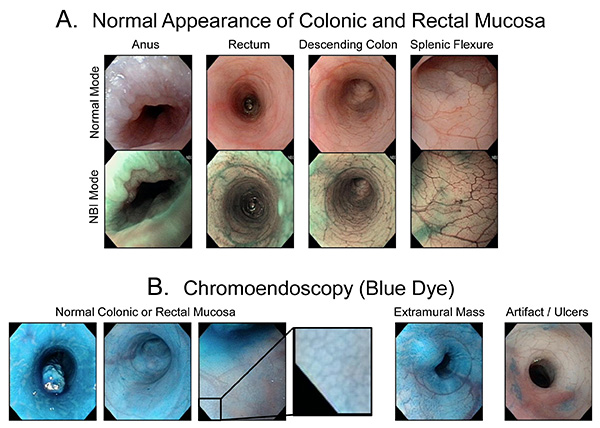
Figure 3. Paired images of normal mucosa in normal endoscopic light mode, NBI mode, and with chromoendoscopy. Arborization of blood vessels is normally less common in the rectum. Click here to view larger image.
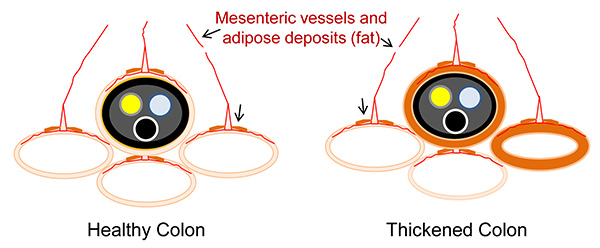
Figure 4. Cross-sectional representation of intestinal loops to illustrate the principle of endoscopic transparency of the intestinal wall in mice. Endoscopic visualization of mural intestinal vessels and mesenteric fat, and that of mesenteric vessels and fat from adjacent healthy viscera, is possible through the wall of a healthy colon. Inflammation and thickening of the intestinal wall in the peritoneal sections of the distal colon prevents the visualization of intramural and transmural structures from other viscera, even if other intestinal segments are healthy. Click here to view larger image.
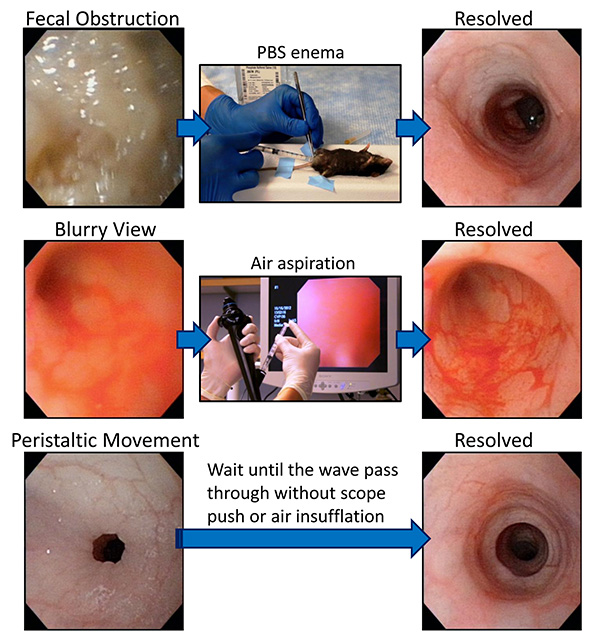
Figure 5. Troubleshooting. Resolving low visibility caused by intestinal content, blurry images and peristaltic movements. Click here to view larger image.
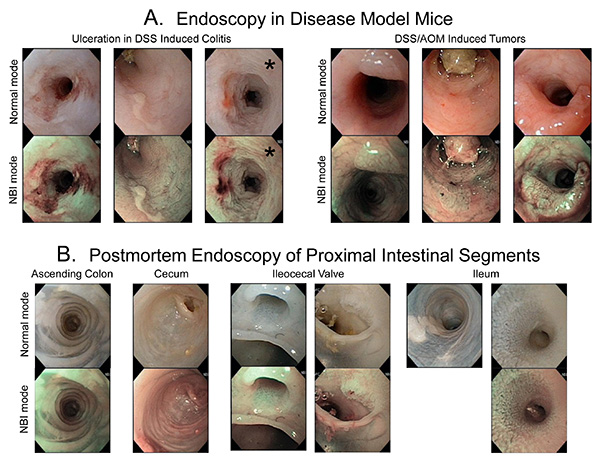
Figure 6. Paired images (regular light vs. narrow-band imaging, NBI) of diseased colorectal mucosa and other proximal intestinal segments. NBI helps to identify ulcerative and tumorous lesions. Some ulcers appear brownish with NBI; others, covered with fibrinous material appear thick and white. AOM/DSS tumors are better characterized with NBI, especially during early stages when they are not protruding into the lumen. Asterisks (*) highlight endoscopic artifact (mucosal corrugation) in colon filled with PBS, not observed in all other images where colon is distended with air. Click here to view larger image.
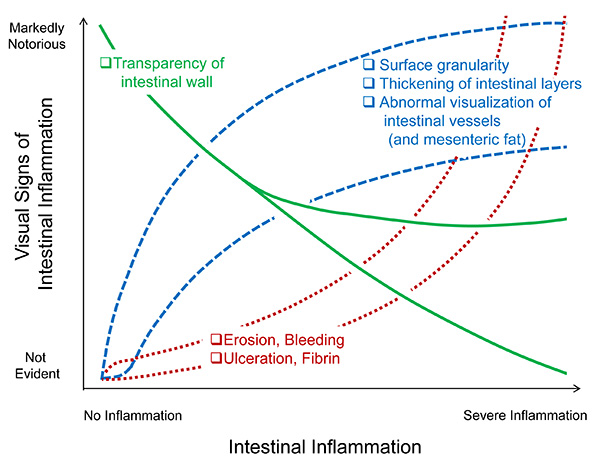
Figure 7. Theoretical correlation and co-linearity between the severity of intestinal inflammation and the ability to visually discern and grade various published criteria of colonic inflammation (see Table 1). Click here to view larger image.
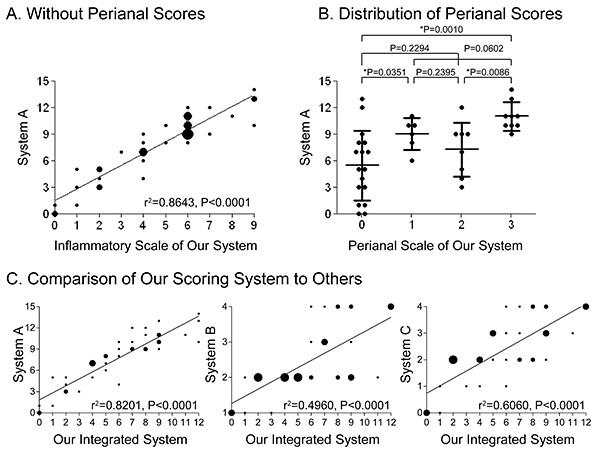
Figure 8. Comparison of performance between our scoring system and previously published scoring systems. Data from paired blind analyses of 36 mouse video endoscopies. A) Comparison of System A (5 parameters) to the inflammatory parameters, except the perianal lesions (3 parameters). B) Importance of including perianal findings in the scoring system; perianal examination consistently provided additional statistically significant information in cases of moderate/severe colitis in mice. C) Performance of the scoring system after including the perianal findings in comparison to previously reported systems (36 mouse video endoscopies were scored with each method). Note that systems B and C have a major limitation due to clustering of cases in one of their four categories leading to misclassification bias (Systems B and C cluster cases in nonequivalent categories). By adding decimal identifiers, we also lowered the chance of clustering in integer categories, while allowing tracking of now meaningful numerical scores. Click here to view larger image.

Table 1. Clinical parameters published as endoscopic criteria to assess intestinal inflammation in mice. Click here to view larger image.
Endoscopic Assessment of Murine Colorectal Inflammation and Tumors Using a Decimal-weighted Scoring System: Parameter Definitions and Protocol
Our integrated endoscopic scoring system for colorectal health has three major components: 1) assessment of the extent and severity of colorectal inflammation, with four parameters and 12 possible numerical grades; 2) recording of the location, size and number of tumorous lesions; and 3) decimal units with assigned types of primary or predominant lesions and endoscopic complications to highlight findings of special significance for the researcher, herein referred to as “decimal identifiers”. The location and size of tumors are recorded on a virtual colonic map, and the number of tumors in each percentage of protrusion (obstruction) into the lumen is recorded on a graph. These two charts provide tumor information that can be integrated in three-dimensions. The decimal units for lesion categories range from 0.0-0.9. If the number of lesions for a particular category is relevant, second and third decimal places can be used to indicate the number of lesions. For example, if three lesions are observed, adding 0.003 would allow the researcher to know that there were three lesions; if there are 12 lesions, then 0.012 would be used. This tracking system is of special benefit if repeated endoscopic examinations are anticipated. Detailed definitions of the inflammation criteria and severity grades are given below.
A. Assessing colorectal infammation with four clinical parameters – definition of endoscopic criteria
1. Perianal findings: Assess this aspect before commencing scoping to avoid confusion with post-endoscopy bleeding. Health of the perianal region is a proxy for health status of the colon, skin, and the animal's attitude in general, and is included as part of the endoscopic examination because some lesions cannot and should not be examined closely with the naked eye. Exercise biosafety measures as appropriate. Note that healthy grooming habits by the mice may remove blood/discharges, but will not remove skin lesions from the perianal region. Scoring:
- Normal. No blood, diarrhea, fissures, fistulas or discharge observed.
- Clumps of fecal matter or diarrhea observed.
- Clots/clumps of bloody discharge, loose feces (diarrhea), pus, or minor ulcerations observed.
- Granulation tissue or lesions observed that involve most of the surrounding skin and indicate that the animal has marked irritation or inflammation in the perianal region; rectal prolapse.
2. Transparency of the colon: Defined as the ability to visualize the blood vessels or extramural organs through the colonic wall as the colon-endoscope is gently moved. Note that the rectum is naturally less transparent due to the muscular layers and because it is in the pelvic cavity where less contrast exists. This is one of the physiologically most comprehensive parameters as it reflects the overall inflammatory condition or health of the murine colon. Note that it is possible to have a non-inflamed colon with mucosal erosions/ulcers in early stages of infection or toxic effects on the epithelium. Beware that physiological isotonic solution should be used for flushing during endoscopy, as hypotonic solutions, such as water, cause changes with whitening and contraction of the mucosa in mice if use for prolonged periods (See asterisks in Figure 6).
- Normal. Large and small blood vessels of the colon and the surrounding viscera are clearly visible. Move the endoscope slightly (back and forth, clock/counterclockwise). White mesenteric fat or dark content of other viscera can also be observed.
- Small vessels are partially invisible but large vessels are visible.
- Small vessels are invisible and large vessels are not clear. The mucosa does not appear thickened.
- Apparent thickening of the intestinal wall and/or mucosal edema/generalized. Blood vessels are not visible. Few distended/varicose vessels may be visible in some cases.
3. Mucosal bleeding: Differentiate contact bleeding from spontaneous bleeding. Routine standard endoscopic procedures in healthy mice should not induce bleeding. If there is inflammation, the increased mucosal vascularity and tissue fragility can lead to mucosal erosion and bleeding. There is no need to intentionally scrape the colon to assess this parameter.
- Normal, no bleeding.
- Common contact bleeding. This traumatic bleeding is defined as contact bleeding; it should be judged only after withdrawing the endoscope.
- Not applicable. Intentionally not assigned to force the examiner to decide the nature of bleeding.
- Spontaneous bleeding, defined as a non-traumatic and naturally-occurring hemorrhage that is observed as the endoscope enters the colon. Sometimes, air insufflation induces spontaneous bleeding during severe colitis.
4. Focal lesions: To accommodate the patchy, unpredictable nature of colorectal diseases, this integrated scoring system allows grading for the presence of focal lesions (mostly ulcerative in nature) by the severity of the inflammation. Since the colon is a short, straight tubular segment in mice, it was deemed unnecessary to describe the location of the lesions. Instead, the number of lesions are recorded and added to the total score using the system of decimal identifiers. However, if emphasis on the location of the lesions is needed, we have an option called ‘Distal-Proximal Endoscopic Colitis Scoring System’ (D-PECS) described below in section F. Further streamlined applications can be derived from our decimal scoring system. Because tumors rarely exist without inducing some form of inflammation in the colorectal region in mice, we have included tumors in the decimal identifiers section to uniquely allow the study of tumors in the context of intestinal health (see below).
- Normal, no focal lesions.
- Well-defined areas of small flat elevation covered by normal mucosa observed. This is to address local edematous areas or potential areas of cell infiltration/proliferation, as found in mild colitis.
- Reddened or erosive areas observed.
- Ulceration or strictures. Ulcers are identified by redness and deformity (irregular edges with evidence of abnormal vascularization) due to edematous or fibrotic wound repair. NBI endoscopy is useful to differentiate detection or observation of ulcerations. Strictures are recognized as areas abnormally narrow, circular or irregular and static in shape, that do not contract or expand as expected. Often strictures involve areas of abnormal mucosal crypts, or villi in the ileum. In the case of flexible endoscopes (external diameter = 3.3 mm) the careful inability to advance the scope into more proximal areas of the colon has been consistently associated with abnormal strictures verified post-mortem.
B. Tumor charts for recording location, size and number
1. Virtual colonic map: This map is a virtual perspective image of the distal colon and rectum that is made by cutting the top of the lumen (0°) and rolling it out. The top and bottom of the chart are assigned proximal of the colon (flexure), and anus, respectively. The center line (180°) indicates the bottom of the lumen (ventral aspect of animal), and right and left halves of the semicircles indicate the right and left wall of the lumen. The map can be used to describe the location and horizontal size of tumors, as well as ulcerations.
2. Tumor numbers for each degree of tumor occupation: Although the colonic map provides only two-dimensional information, the extent to which tumors grow into the gut lumen is an important feature of tumors, since protrusion can cause intestinal stenosis or obstruction. To capture this information, we added a recording graph for percent protrusion into the lumen that documents the number of tumors in each percentage range, allowing a three-dimensional perspective for assessing the extent of colonic tumors.
C. Decimal identifiers to make numerical scores meaningful and fast-track relevant cases
Our scoring system uses a novel decimal identifier system to record the presence of relevant lesions or complications. These identifiers are for descriptive purposes and are intended to facilitate interpretation of a numerical score and fast-track cases of endoscopic interest. However, they also serve to numerically weight predominant types of lesions, and allow the generation of data sets amenable to parametric statistics. When using the developed scoring form, mark the lesions as appropriate, and choose one decimal identifier to be added to the inflammatory score.
- No special findings.
- Perianal fistula, or excessive perianal inflammation, rectal prolapse.
- Primarily erosive lesions with minor wall involvement.
- Mostly ulcerative lesions, some covered with fibrin, bleeding, or large with irregular shapes due to coalescing of small ulcers (the number of ulcers can be recorded as 0.301 for one tumor, 0.302 for two tumors, 0.311 for eleven tumors, etc.).
- Intestinal stricture (optional because stricture is a severe inflammatory complication in colitis, add 2 points to the total inflammatory score).
- Well-defined plaque (thick/nontransparent tissue within intestinal wall; e.g. a flat low-height tumor). The number of plaques can be recorded as described for lesions (i.e., 0.401, 0.402,…0.411, etc.). They may appear as a flat non expandable surface that may seem to protrude up to about 5-10% which modifies the circumferential appearance of the intestinal lumen.
- Protruding mass or tumorous lesion. The number of masses can be recorded as described for lesions (i.e., 0.601, 0.602,…0.611, etc.). They are clearly bulging, but may appear flat but protruding >15% of the distended circumference of the intestinal lumen.
- Induced tear/perforation during endoscopy.
- Death of animal during endoscopy.
- Other: _____________ (e.g. severe proximal endoscopic colitis, see Distal-Proximal Endoscopic Colitis Scoring System below).
D. Examples and applications
The murine endoscopy scoring system presented in this paper is specifically designed to integrate the collection and analysis of data on colonic inflammation and colorectal tumors. With respect to tumors, the data can be analyzed using multiple statistical approaches, including area under the curve, median, mode, or principal component analysis. At the individual level, the scoring system can help researchers monitor colonic health in a single mouse over time. After summing the inflammatory subscores and appending the proper decimal identifier for type and number of lesions where appropriate, the total score will allow researchers to numerically quantify the extent of colonic inflammation, the most predominant type of lesion, and the number of lesions. For example, a score of 12.609 indicates that this mouse has severe colorectal inflammation and nine protruding tumorous masses; a healthy mouse with a normal perianal region and colorectal mucosa that was perforated during endoscopy would have a total score of 0.7. The decimal identifier system will allow researchers to catalogue and easily search large data repositories of scored mice. For example, a researcher could set search criteria to identify all scores that end in “0.6” and retrieve all cases that have protruding tumors. More examples are illustrated in the supplementary Figures S1-S3.
E. Distal-proximal endoscopic colitis scoring system (D-PECS)
This is an optional modification of our decimal identifier scoring system to differentiate cases with severe/extensive proximal colitis. Because the endoscopic signs of colitis and colorectal tumors in mice appear to develop consistently in the distal segments of the colon we recommend:
- To score the colon following the criteria described, paying special attention to the distal two-thirds of the colon and ignore the proximal segment if it is apparently healthy. This avoids confusion and increases discriminatory power of endoscopy to differentiate animals with various degrees of extensive colitis.
- If inflammatory or tumor changes are observed in the proximal third, we recommend to add one point to the total score (1.0) and assign the decimal identifier as ‘0.9 – Other,’ which could be labeled as severe proximal endoscopic colitis. Plot the findings in the map grid and bar chart.
- Monitor animals that have endoscopic abnormalities in the proximal third of the colon. Pay special attention postmortem, as disease may be unusually severe or may extend beyond the splenic flexure towards the proximal colon.
- If this recommendation was followed, record this approach in the ‘observations section’ of the evaluation form, and follow this trend across experiments. Please cite in your final publication that the assessment was conducted following our ‘distal-proximal endoscopic colitis scoring system’ or D-PECS, which ranges from 0-13.9. Note that this modification has no statistical effect on our scoring system if used in animals without extensive/severe proximal colitis.
Supplemental Figures.
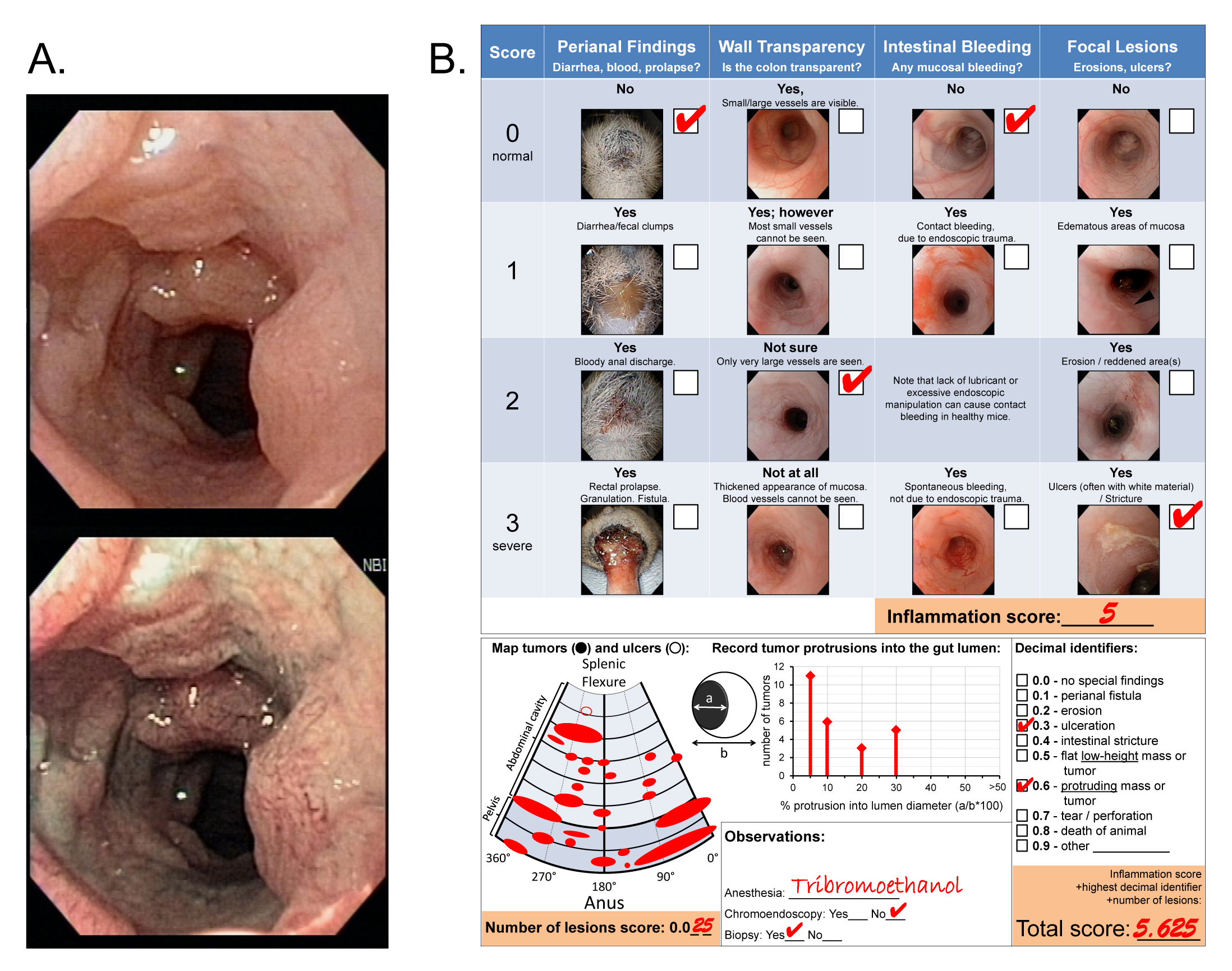
Figure s1. Example of endoscopic assessment of a mouse with colorectal tumors. Animals were treated with AOM and DSS prior endoscopy. A) Representative image in normal and NBI mode, respectively. B) Scoring form filled with endoscopic findings. Note that although there are two relevant findings, the researcher chose to assign the decimal identifier 0.6 based on clinical severity and research goals. A variety of parametric statistical analysis can be conducted with the data recorded in the ‘Map of Tumors/ulcers’ and the ‘Record of tumor protrusions’ charts. Click here to view larger image.
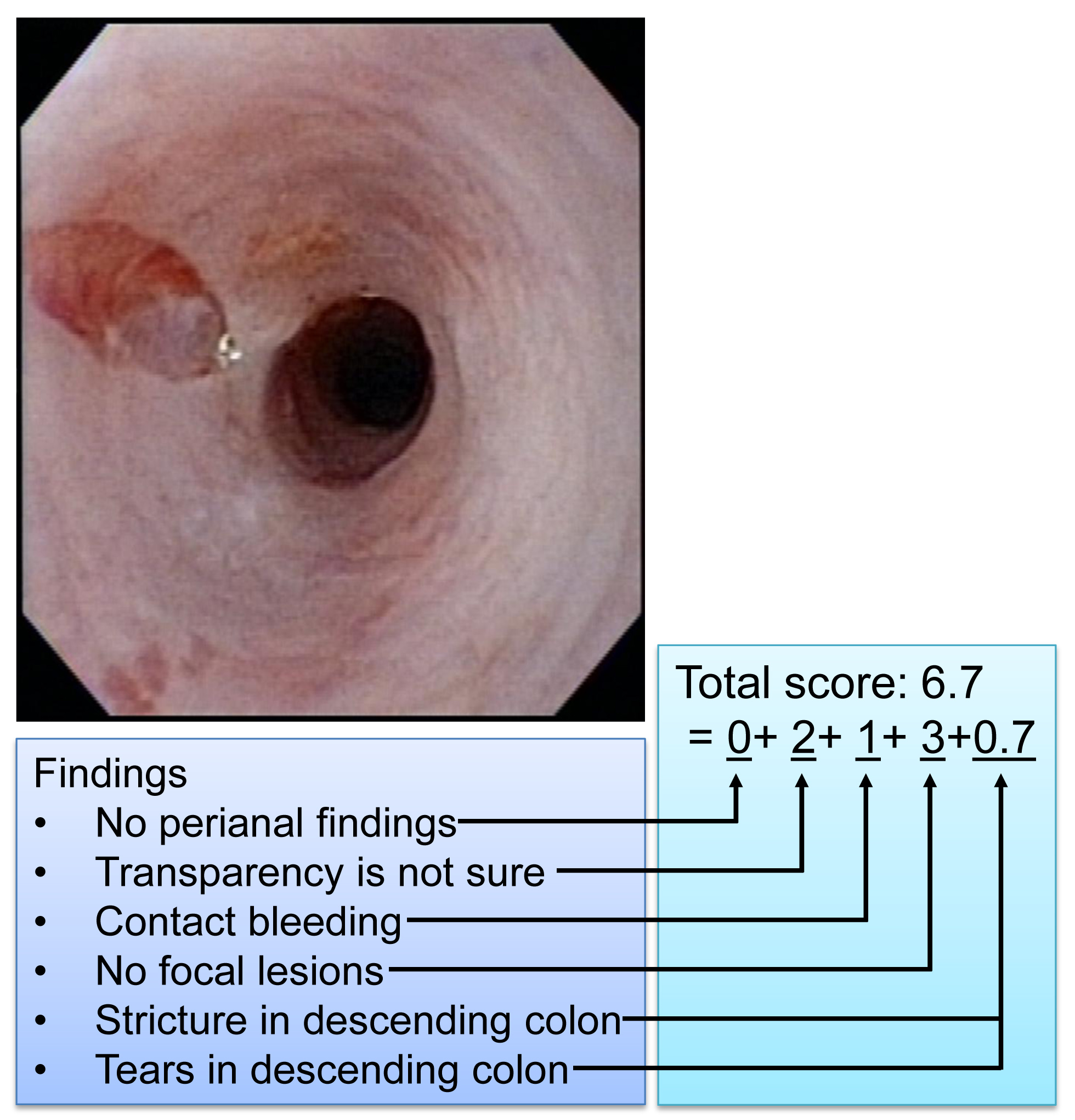
Figure s2. Example of a mouse with a colonic stricture and an endoscopic complication. Note the narrowing of the intestinal lumen and that a nonperforating, mucosal tear was induced during endoscopy just distal to the stricture site. Narrowing and debilitation of the inflamed colon may result in mucosal tears. The animal was under general anesthesia. Note that the scoring system has allowed us to monitor and reduce procedural complications. Click here to view larger image.
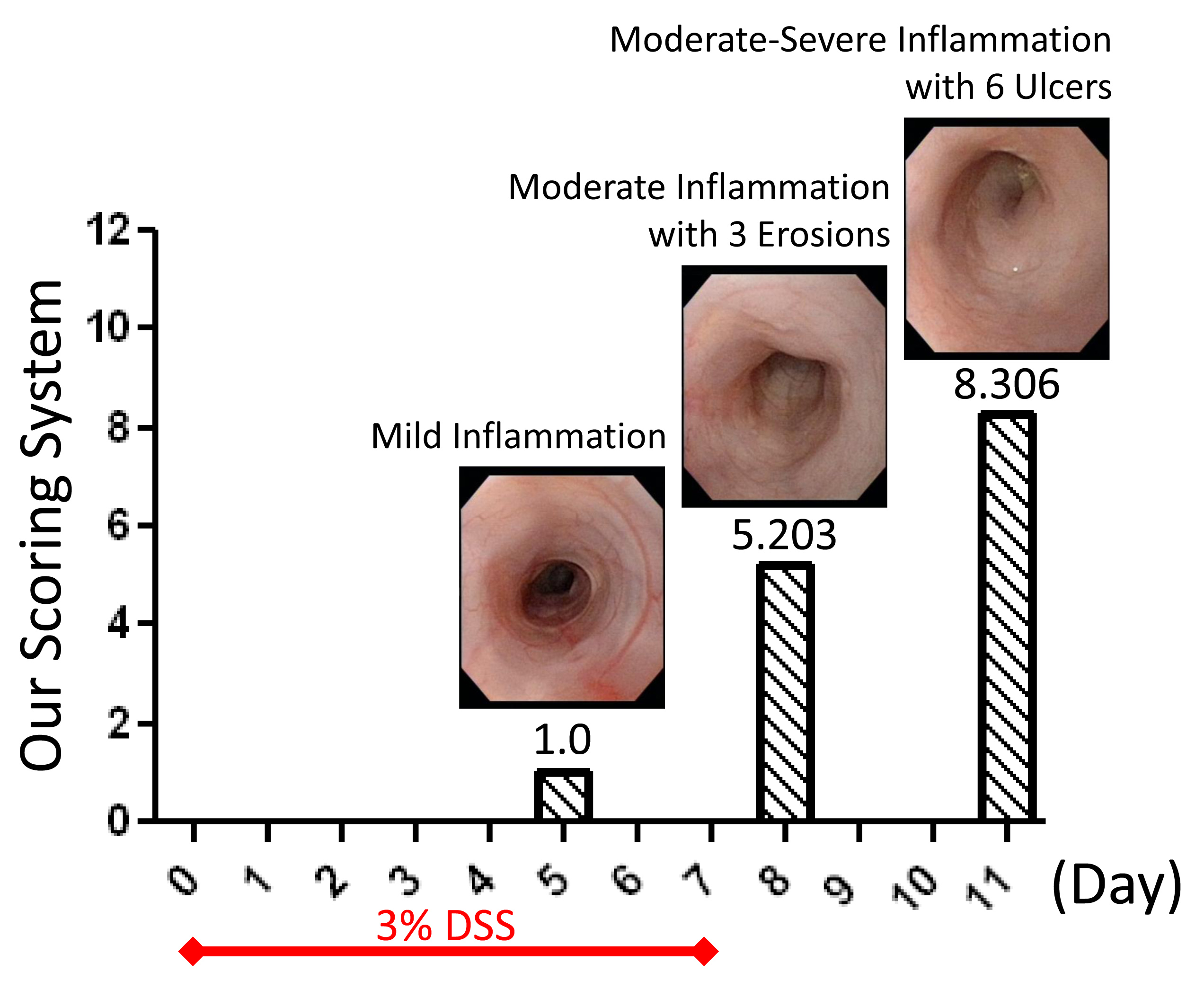
Figure s3. Example of time course of inflammation and endoscopic scoring in a DSS-treated mouse. Note that the numbers can be self-explanatory and indicate that colonic inflammation progressed (from 1-5 and 8), and that erosions developed by day 8 (decimal 0.2) and ulcers by day 11 (decimal 0.3). Click here to view larger image.
