Five week old LDLR-/- mice were fed a standard diet or a high fat diet for ten weeks. Mice were sacrificed and perfused with formalin as described above. Cross sections of the aortic sinus were prepared and stained with hematoxylin and eosin to determine lesion area and volume (Figure 4). When mice are fed a standard chow diet, atherosclerotic development is very limited and may not be detectable at 15 weeks of age. High fat diet significantly accelerates atherogenesis in this model and induces the formation of large advanced lesions containing necrotic acellular cores and fibrous caps.
Atherosclerotic lesions can be further characterized by staining for the presence of specific cell types and factors that define stages of lesion development. Monocyte infiltration into the intima represents one of the earliest events of atherogenesis. Intimal monocytes differentiate into macrophages which engulf cellular debris and lipids. Lipid engorged macrophages, known as foam cells, create a "fatty streak" in the artery wall.
Macrophage/foam cells can be detected at all stages of lesion development by staining with antibodies against specific macrophage markers including F4/8017, CD6818, Mac-3 (CD107)19, and MOMA-220 (Figure 5). Vascular smooth muscle cells (VSMCs) are confined to the medial layer of a healthy artery. VSMCs are induced to migrate and proliferate in the intima during the development of an advanced lesion. VSMCs can be identified by staining with an antibody against alpha actin21 (Figure 5).
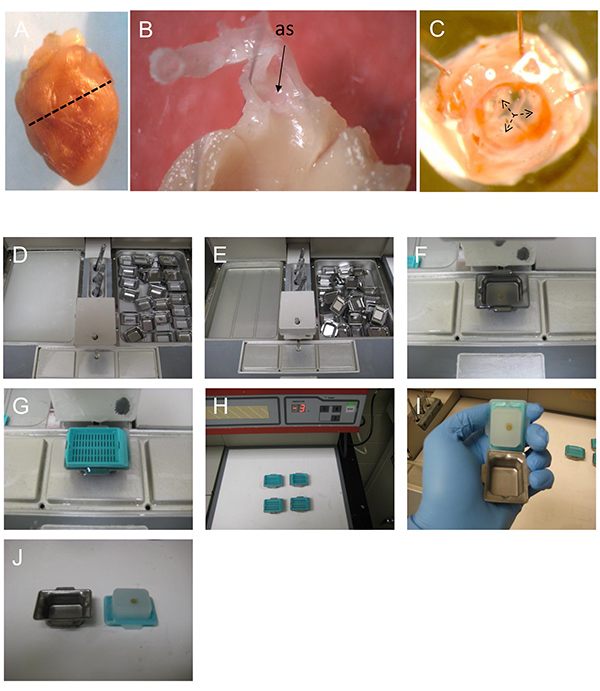
Figure 1. Preparing the heart and the aortic sinus for embedding and sectioning. A) The mouse heart is transversely cut along a straight line joining the lower tips of the right and left atria. The apical (top) part of the heart is processed to examine and quantify atherosclerosis in the aortic sinus. B) A cut away view showing the orientation of the ascending aorta and the aortic sinus (as) of a dissected heart. C) A view of the aortic sinus from inside the heart. The three aortic valve leaflets are identified (black arrows). D-E) paraffin wax is melted overnight and (F) poured into the mold containing the tissue. G) The mold is covered with a labeled plastic cassette and (H) cooled on ice to set. I-J) The solid paraffin block is separated from the mold and is ready for sectioning.
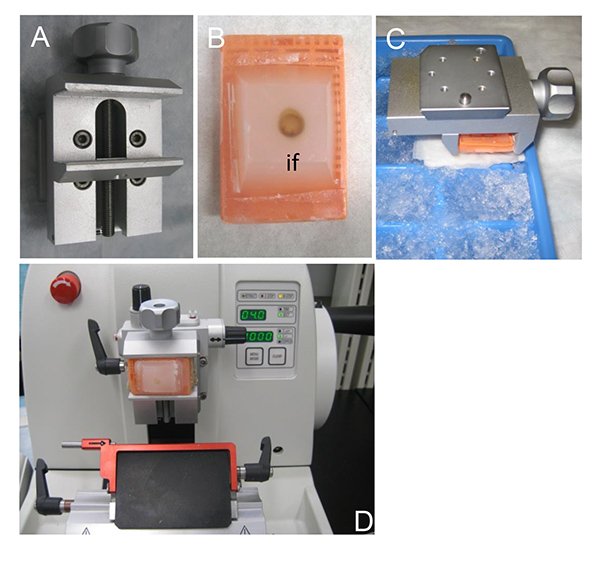
Figure 2. Tissue sectioning using a microtome. A) The specimen holder that allows cutting angle adjustments during sectioning. B) A paraffin block containing the dissected heart. The sectioning proceeds from the inner face (if) of the dissected heart which has to be completely exposed in the paraffin block. C) Cooling the specimen on ice just prior to sectioning. Cooling causes the paraffin block to contract and improves the quality of the resulting sections. D) The microtome set up. Sections 4-5 µm of thickness are ideal for staining and analysis.
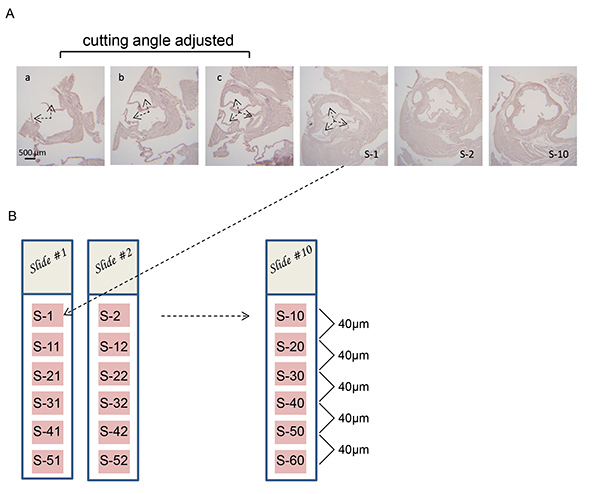
Figure 3. Adjusting the microtome cutting angle to obtain perpendicular cross sections of the aortic sinus. A) Series of cross sections of aortic sinus from an LDLR-/- mouse. Two partial valve leaflets are visible in section "a" (arrows). The cutting angle is adjusted "a-b" and "b-c" until all three valve leaflets are equally visible in each section ("c") (arrows). Under normal circumstances the cutting angle will be adjusted by viewing unstained sections under a light microscope. The sections shown have been stained to increase clarity. B) 10 glass slides are labeled from Slide #1 to Slide #10 and 4 µm thick sections (S-1 to S-10) are collected successively onto the top portion of each slide. Then, the next series of 10 subsequent sections are collected following the same pattern: S-11 to S-20; S-21 to S-30; S-31 to S-40 until the atherosclerotic lesions are no longer observed. Hematoxylin and eosin staining is carried out to visualize the atherosclerotic lesions on each section of the slide being analyzed.
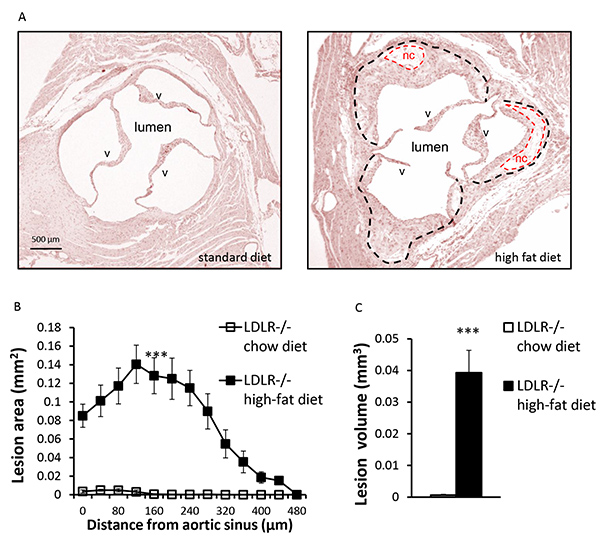
Figure 4. Quantification of atherosclerotic lesions. A) Representative hematoxylin and eosin stained cross sections of aortic sinus from a 15-week-old LDLR-/- mouse fed a standard or high-fat diet, as indicated. Atherosclerotic lesions (outlined with black dashes) and acellular necrotic core (nc) (outlined with red dashes) as well as the aortic valves (v), are indicated. B) Quantification of atherosclerotic lesion area through the aortic sinus and ascending aorta. Each point represents the mean lesion area (± SEM) determined at a specific distance from the aortic sinus. Atherosclerotic lesion area is measured using ImageJ software. C) The volume of the atherosclerotic lesions is estimated by calculating the area under the curve for each condition. n=5 mice per group, *** p<0.001.
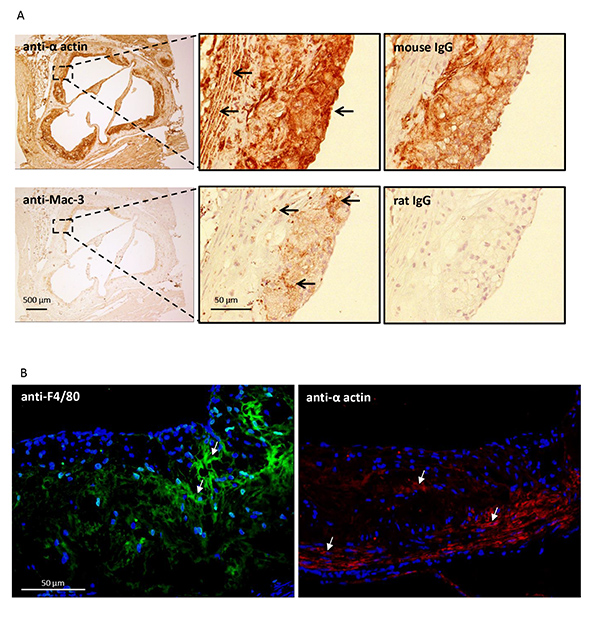
Figure 5. Characterization of the atherosclerotic lesion. Cross sections of the aortic sinus were prepared from 15 week old LDLR-/- mice fed a high fat diet. A) Sections were immunostained for macrophage/foam cells (Mac-3) or vascular smooth muscle cells (anti-alpha actin) using a standard immunohistochemical technique (see protocol 5). Positively stained cells are indicated by the arrows. Serial sections were stained with preimmune IgG as a control. B) Similar sections were immunostained for macrophage/foam cells (F4/80) or vascular smooth muscle cells (anti-alpha actin) using an immunofluorescence technique (see protocol 6). Positively stained cells are indicated by the arrows.
