1. Oscillatory Lower Body Negative Pressure (OLBNP)
- Equipment Setup
- Electrocardiogram Lead II (ECG): Affix the three (or more) electrodes to the subject’s torso for the monitoring of heart rate throughout the study.
- Neoprene Skirt: Use a custom made neoprene skirt that seals the subject into lower body negative pressure chamber up to the iliac crest. Put it around the subject’s chest before they are placed supine in the tank and ensure that the ECG signal is still adequate. Ensure that it is snug but not so tight as to restrict breathing.
- Lower Body Negative Pressure Chamber: Have the subject lie supine on the bed and maneuver the LBNP chamber underneath them. If the LBNP chamber has an adjustable bicycle seat (to minimize movement artifact without counteracting the effect of the suction), make sure the subject is comfortably seated upon it. Use a custom made Plexiglas spacer cut to the subject’s waist size to help seal the chamber. Seal the neoprene skirt around the LBNP chamber with duct tape.
- LBNP Chamber Pressure: Connect the LBNP chamber to a standard pressure transducer. Calibrate the pressure transducer to mmHg.
- Repeat Cycle Timer Attached to Mechanical Valve: Attach the custom built mechanical valve and repeat cycle timer to the LBNP chamber.
NOTE: A time delay relay attached to two motors that control a mechanical valve is used to alternate between negative pressure and ambient pressure. The time delay relay alternates voltage to the motors at a fixed interval to open and close a valve between the chamber and the vacuum. This creates an LBNP chamber pressure waveform that is roughly square wave in shape. Adjust the cycle time to the desired OLBNP frequency. - Variable Transformer and Vacuum: Attach a standard household vacuum cleaner to the mechanical valve. Plug the vacuum into a variable transformer that allows the voltage to the vacuum to be controlled. Turn on the vacuum cleaner and adjust the variable transformer until the target LBNP pressure (e.g., 30 mmHg) is achieved.
- Arterial Blood Pressure: Attach non-invasive photoplethysmographic arterial pressure cuffs (e.g., Portapres, Finapres) to the finger(s) of one hand. Ensure accuracy by comparing pressure to oscillometric pressures from the brachial artery of the opposite arm.
- 2 MHz Transcranial Doppler and Probe Fixation Device
- Use a 2 MHz pulse wave Doppler probe to insonate the M1 segment of the middle cerebral artery at the temple (i.e., the transtemporal window).
- Alter probe angle, insonation depth (~55 mm), gain, and transmission power to maximize the spectral intensity of the signal.
- Fix the Doppler probe in place using a fixation device that has no back (i.e., not a headband) so that movement artifact is not introduced into the signal as the volunteer moves with negative pressure oscillations.
NOTE: Cerebral blood flow can be measured unilaterally or bilaterally, but no difference in cerebral autoregulation is expected between hemispheres unless a localized injury like stroke or traumatic brain injury is present.20
- Expired CO2: Use a nasal cannula attached to an infrared CO2 analyzer to monitor expired CO2 and instruct the subject to breathe only through their nose. Given the profound effect arterial CO2 has on cerebral blood flow,21 monitor CO2 throughout every study.
- Data Acquisition
- Set up the analog to digital conversion of arterial pressure, cerebral blood flow, LBNP chamber pressure, and expired CO2 to acquire at a minimum of 50 Hz per channel. Acquire ECG at 1 kHz.
NOTE: While subsequent analysis deals with much lower frequency information (≤0.07 Hz), it is critical to monitor the quality of the signals being acquired during a study. A sampling rate of 50 Hz will allow accurate visualization of blood pressure and cerebral blood flow for the detection of artifact.
- Set up the analog to digital conversion of arterial pressure, cerebral blood flow, LBNP chamber pressure, and expired CO2 to acquire at a minimum of 50 Hz per channel. Acquire ECG at 1 kHz.
- Oscillatory LBNP Protocol
- Turn on vacuum and ensure tank pressure is stable at –30 mmHg.
- Set repeat cycle timer to 33 sec for 0.03 Hz OLBNP.
- Adjust Doppler probe(s) to ensure optimal signal.
- Acquire data for at least 15 cycles (500 sec at 0.03 Hz) to ensure sufficient confidence in PPR estimates. If time permits, collect more data than this as it will further improve the signal-to-noise ratio.
- Repeat the above steps for any frequencies between 0.03 Hz-0.08 Hz by changing the repeat cycle timer duration.
NOTE: Apply frequencies in order but randomly vary the starting frequency between subjects.
2. Projection Pursuit Regression (PPR)
- Data Preprocessing
- Decimation and Low-pass Filtering
- Open Matlab. Type the command “data = resample(data, 1, SR/5)” (where SR is the original sampling rate) to decimate the arterial pressure and cerebral blood flow to 5 Hz.
NOTE: Optionally, low-pass filter (19th order Chebyshev Type II) with a cutoff of 0.4 Hz. The filtering is redundant, given subsequent processing, but creates mean waveforms that don’t rely on peak detection of the sometimes noisy arterial pressure and cerebral blood flow signals.
- Open Matlab. Type the command “data = resample(data, 1, SR/5)” (where SR is the original sampling rate) to decimate the arterial pressure and cerebral blood flow to 5 Hz.
- Artifact Removal
- Using the original non-decimated waveforms as a guide, remove any sections of the signals with artifacts and linearly interpolate. If these sections account for more than 10% of the recording period, discard the recording entirely.
NOTE: At this point, the waveforms are suitably processed for traditional linear approaches such as transfer function analysis.
- Using the original non-decimated waveforms as a guide, remove any sections of the signals with artifacts and linearly interpolate. If these sections account for more than 10% of the recording period, discard the recording entirely.
- Band-pass Filtering
- In Matlab, type: [B, A] = cheby1(1,1, [F – 0.005 F+0.005]/(SRd/2)) data = filtfilt(B, A, detrend(data, ‘linear’) to band-pass filter the pressure and flow in a ± 0.005 Hz band (1st order Chebyshev Type I with 1 dB of pass band ripple) around the frequency of OLBNP (Figure 2) where F is the dominant OLBNP frequency, SRd is the decimated sampling rate (5 Hz after step 2.1.1), and “data” is the decimated signal (arterial pressure or flow).
NOTE: This minimizes potential interference and increases the signal-to-noise ratio in subsequent PPR analysis. Although the dominant arterial pressure fluctuation occurs at the oscillatory frequency of lower body negative pressure, random noise in the signals may interfere with the derivation of pressure-flow relationships. Results without band-pass filtering will be qualitatively similar but the percent variance explained (i.e., R2) will be lower.19
- In Matlab, type: [B, A] = cheby1(1,1, [F – 0.005 F+0.005]/(SRd/2)) data = filtfilt(B, A, detrend(data, ‘linear’) to band-pass filter the pressure and flow in a ± 0.005 Hz band (1st order Chebyshev Type I with 1 dB of pass band ripple) around the frequency of OLBNP (Figure 2) where F is the dominant OLBNP frequency, SRd is the decimated sampling rate (5 Hz after step 2.1.1), and “data” is the decimated signal (arterial pressure or flow).
- Decimation and Low-pass Filtering
- Projection Pursuit Regression Estimation
NOTE: Using the built-in function ‘ppr’ in R Language and Environment for Statistical Computing, and/or via custom-written functions in other platforms, generate a single ridge function (M=1) for the arterial pressure-cerebral flow relation.- In Matlab, enter the command “CVLabPPR(pressure,flow)”. Enter the Study ID as XXXYYY, where XXX is the 3-letter study code and YYY is the three numeric characters for subject ID. Enter the Study Date in the following format: YYYY-MM-DD. Enter the numeric measurement # (e.g., “1” for day 1).
- Enter the APM (enter FP for finapress or AL for art-line). Enter the Vessel (MCA, ACA, or PCA). Enter “y” or “n” to the query “Do you have right MCA measurements?” Enter “y” or “n” to the query “Do you have left MCA measurements?”
NOTE:

For each input (xt — arterial blood pressure) and output (yt — cerebral blood flow) a linear autoregressive transfer function (Eq 1. — the term within the parentheses) is passed through nonparametric kernel functions (km; called 'ridge functions') that are determined by minimizing the mean squared error. Projection pursuit regression can include more than one ridge function (i.e., M > 1). However, though it will reduce the mean squared error, it may obscure the interpretation of ridge functions due to potential interactions between them. Because the primary purpose is to obtain a relation between arterial pressure and cerebral blood flow that can be interpreted physiologically, PPR should be limited to only one ridge function (M = 1). - Piecewise Linear Parameterization. Parameterize the ridge function as a piecewise linear function for subsequent statistical analysis (Figure 3). For Matlab, use Bruno Luong’s Free-knot spline approximation. Enter the command “BSFK(x, y, k, nknots)” where k=2 for a linear fit and nknots=3 for three regions.
NOTE: This identifies those points where the arterial pressure-cerebral flow relationship changes, and the ranges wherein the relationship is approximately linear. Figure 3 shows a schematic of the results. The gain (i.e., the linear slope) of the pressure–flow relation within each region provides a measure of the effectiveness of cerebral autoregulation within that region. A lower gain indicates more effective counter-regulation of pressure fluctuations whereas higher gains indicate more passive flow responses to pressure changes.
OLBNP amplitudes from 10 mmHg22 up to 120 mmHg17 have been used to augment arterial pressure fluctuations, but 30 mmHg OLBNP is sufficient23,24 and not beyond the regulatory capacity of the cerebrovasculature.17 This level of OLBNP results in blood pressure oscillations that are about 15-20 mmHg in magnitude at 0.03 Hz, which is not greater than the blood pressure changes occurring when going from seated to standing.25 There are some limitations to the range within which OLBNP can generate arterial pressure fluctuations. Autoregulation is only active at ~0.07 Hz and slower, so the upper limit is not an issue. However the difficulty in generating low frequency oscillations below 0.03 Hz is that the cardiovascular system counter-regulates against the LBNP-induced arterial pressure changes before the cycle is finished. As Figure 4 shows, at 0.025 Hz OLBNP we actually see the largest peak in the arterial pressure oscillations at 0.05 Hz. While the frequency response of cerebral autoregulation can be characterized from 0.03 Hz-0.08 Hz to define the time scales within which autoregulation is active,23,24 0.03 Hz and 0.08 Hz OLBNP are sufficient since they represent a range of autoregulatory function (i.e., a pronounced autoregulatory region to none or a modest one).
OLBNP generates larger fluctuations in arterial pressure as the frequency of negative pressure oscillations become slower. Figure 5 shows the arterial pressure and consequent cerebral blood flow fluctuations with OLBNP from 0.08 Hz (12.5 sec cycles) to 0.03 Hz (33 sec cycles). At the higher frequencies, cerebral blood flow fluctuates in concert with arterial pressure. The PPR demonstrates this; there is a proportional linear relation between arterial pressure and cerebral blood flow at the higher frequencies of 0.08 Hz, 0.07 Hz (14 sec cycles), and 0.06 Hz (16.6 sec cycles). At slower frequencies of OLBNP, though arterial pressure fluctuations become larger, fluctuations in cerebral blood flow are progressively more effectively dampened. Hence, the PPR shows an increasingly more prominent autoregulatory region at OLBNP frequencies from 0.05 Hz (20 sec cycles), to 0.04 Hz (25 sec cycles), to 0.03 Hz. In the example shown, at 0.03 Hz, the PPR curve clearly resembles the “classic autoregulatory curve” described by Lassen (Figure 1). We have previously shown that this observation cannot be explained simply by the increase in magnitude of arterial pressure fluctuations as the frequency of oscillations become slower. We have previously applied PPR to data from 48 individuals during different magnitudes of OLBNP (thus, different magnitude of pressure fluctuations).19 While we did not explicitly explore a potential relation between autoregulatory range and the magnitude of pressure fluctuations, we reported that the variation in autoregulatory range was only ~6%. Thus, our prior results clearly show that the change in PPR curve with frequency cannot be fully explained by a change in the magnitude of pressure fluctuations. In the same study, we assessed whether the PPR characterization of autoregulation is reproducible across separate sessions. This analysis showed that the slope of the autoregulatory range during 0.03 Hz OLBNP did not change (Lin’s Concordance = 0.96, p < 0.001) and thus the nonlinear pressure-flow relation is consistent across study days.
Although the cerebrovascular bed is well innervated by sympathetic nerve fibers, their role in autoregulation has not been widely accepted.26 Therefore, some of our previous work explored the potential role of the sympathetic nervous system in cerebrovascular autoregulation.24 We found a clear role for the sympathetic system in regulating cerebral flow, but we were not able to characterize how the relationship changed with removal of sympathetic effects due to the limitations of linear methods for characterizing autoregulation. Figure 6 shows the results from PPR application to data before (baseline) and after sympathetic blockade during 0.05 Hz. The overall curve becomes markedly more linear. Moreover, PPR analysis of 0.03 Hz data where autoregulation is most apparent showed that the range of the autoregulatory region remains unchanged, but the slope within that region increases, reflecting less effective autoregulation (Figure 7).
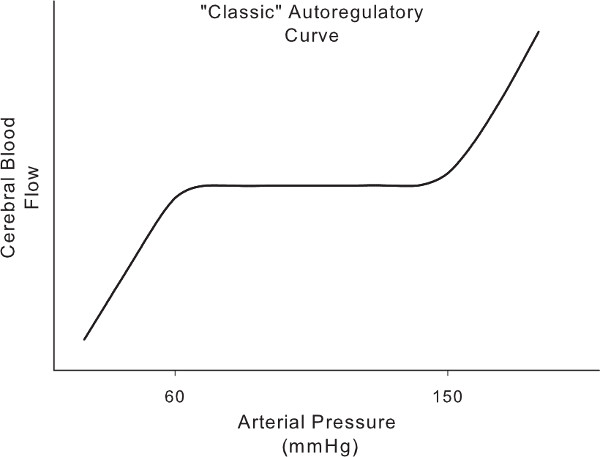
Figure 1. The 'classic' autoregulatory curve derived from the relationship between static increases and decreases in pressure and steady state cerebral blood flow. A region of unchanging flow despite changing pressure (i.e., slope = 0) is bounded by regions wherein increasing and decreasing pressures result in proportional cerebral blood flow changes.
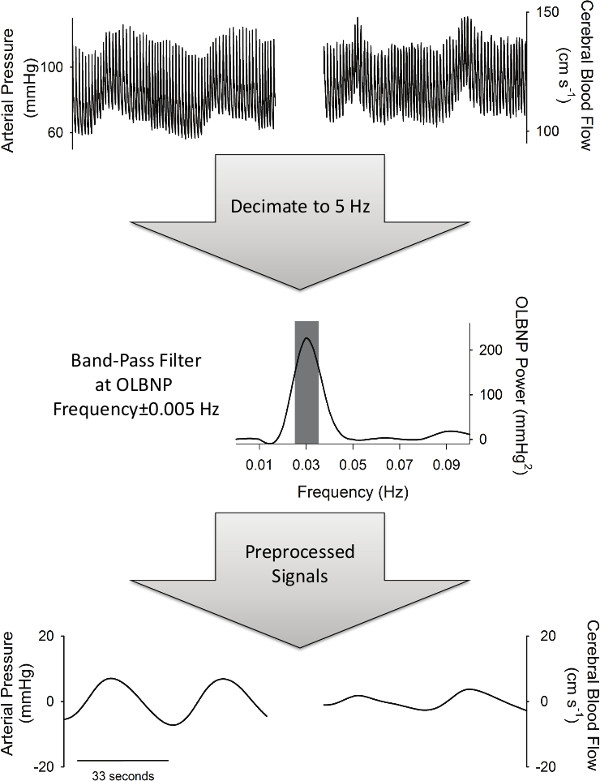
Figure 2. The preprocessing necessary to perform PPR analysis. Signals are first decimated to 5 Hz and then band-pass filtered at the frequency of OLBNP (±0.005 Hz).
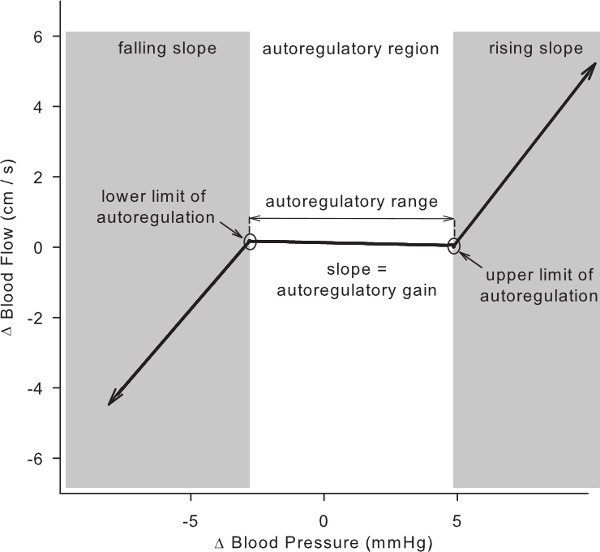
Figure 3. Parameters of the cerebral autoregulation curve derived from PPR analysis of arterial pressure and cerebral blood flow during 0.03 Hz OLBNP.
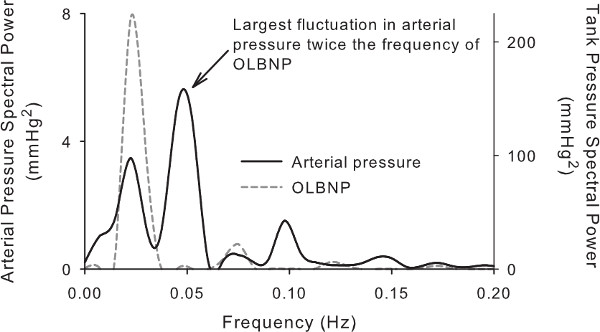
Figure 4. Power spectrum shows the magnitude of fluctuations in arterial pressure when OLBNP frequency is below 0.03 Hz (33-second cycle). Note that there are two large peaks in the arterial pressure spectral power at 0.025 and 0.05 Hz (40 and 20 sec cycles), however there is only a single peak in the LBNP spectral power at 0.025 Hz. Moreover, the largest fluctuation in pressure is at 0.05 Hz and would confound the interpretation of the cerebral blood flow responses.
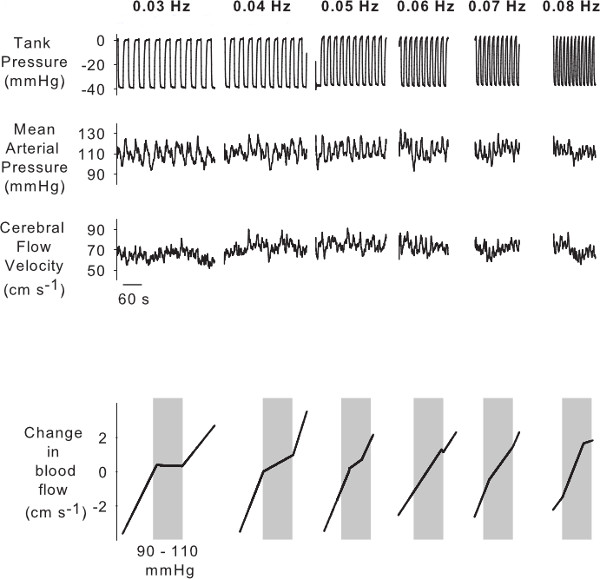
Figure 5. Example of the effects of OLBNP from 0.08 to 0.03 Hz on arterial pressure and cerebral blood flow. Arterial pressure fluctuations become larger with slower OLBNP whereas cerebral blood flow fluctuations become smaller. This autoregulatory function is described by the results of the PPR analysis shown in the bottom panels. The autoregulatory region in cerebral blood flow becomes progressively more pronounced with slower OLBNP.
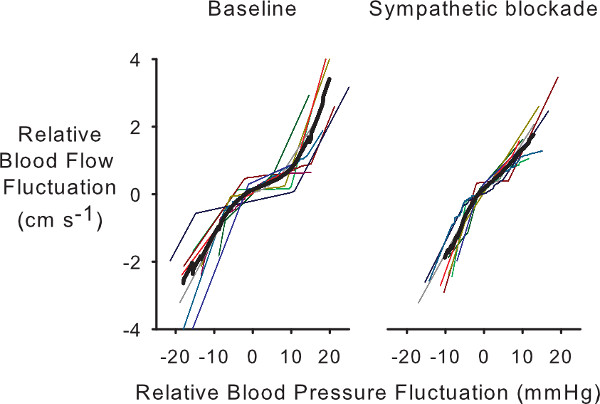
Figure 6. Individual and averaged PPR autoregulatory curves from 0.05 Hz OLBNP data in subjects before (baseline) and after sympathetic blockade. Note that the loss of the narrow autoregulatory region after sympathetic blockade.
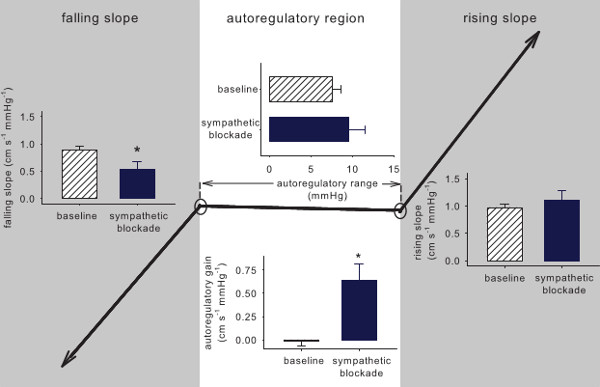
Figure 7. Average of the PPR parameters from 0.03 Hz OLBNP data before and after sympathetic blockade. Sympathetic blockade had a pronounced effect on the cerebral autoregulation curve within the autoregulatory range, markedly increasing the slope (i.e., more proportional cerebral flow changes with pressure changes).
