Functional MRI is the most widely used functional imaging technique to address the underlying neural mechanisms of motor or cognitive functions. More recently, fMRI has also been used to evaluate tDCS effects on cortical activity and connectivity. However, most of these studies administered tDCS outside of the scanner and evaluated offline effects of the stimulation (i.e. administered tDCS prior to scanning22,23). Only a few studies so far have administered tDCS during simultaneous fMRI, using different blood oxygenation level dependent contrast (BOLD)14-17,24 or perfusion imaging sequences13,19. Those studies used within subjects designs to compare functional brain activity or perfusion changes during atDCS vs. sham tDCS to shed light on the neural mechanisms underlying immediate behavioral effects of tDCS in health and disease1,3.
For example, in two recent studies, Meinzer and colleagues assessed neural underpinnings of atDCS-induced performance improvements during semantic word-generation in healthy younger15 and older adults14. In both studies, performance was superior during atDCS administered to the left IFG compared to sham stimulation, indicated by a significantly reduced number of errors during the task. Most notably, performance of older adults during semantic word-generation, a task that is known to be negatively affected by advanced age25-28, was improved up to the level of a matched group of younger adults14.
Task-related fMRI revealed that improved performance during atDCS compared to sham was associated with highly localized task-related activity reduction in the ventral portion of the IFG in both studies (Figure 8). Please note, activity in the left dorsal IFG (an area in the vicinity of the stimulation site) was not affected by the stimulation. In line with a previous study in healthy older adults that employed a different type of word-retrieval task (picture naming17), these activity reductions may be related to more efficient neural processing in task-relevant brain regions14,15. Moreover, in the older group, atDCS reduced age-related enhancement of right-hemisphere activity and reduced activity was correlated with behavioral improvement14. These findings illustrate the potential of this novel technique to identify neural underpinnings of tDCS-action at the stimulation site and also in distant brain regions.
In addition, large-scale network effects of atDCS were confirmed in both studies using RS-fMRI. A graph-based functional connectivity approach revealed: (1) enhanced connectivity (i.e. enhanced communication) between major hubs of the language system in younger adults during atDCS compared to sham (for an example see Figure 9, adapted from Meinzer et al.15). In older adults, atDCS resulted in partial reversal of altered network structure compared to younger adults14. These findings show that large-scale network effects of the stimulation can be identified using this technique.
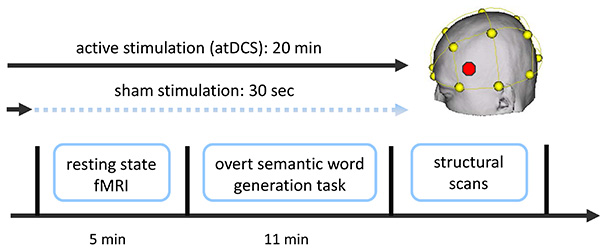
Figure 1. Overview of combined tDCS-fMRI experiment. Two functional fMRI scans were acquired (a resting-state scan followed by a semantic word-generation task). Stimulation (sham or atDCS) started approximately 1-2 min prior to the resting-state scan and commenced until the end of the language task (atDCS), or was ramped down prior to the start of the resting-state scan (sham; not described here; for details see Meinzer et al.14,15). Additional structural scans were acquired after the end of the stimulation. Stimulation location (IFG, red dot in schematic) was determined using the EEG 10-20 system (yellow). Please click here to view a larger version of this figure.
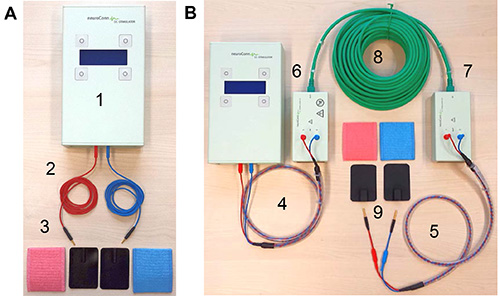
Figure 2. tDCS equipment. (A) Shows standard equipment for a tDCS study. This includes (1) the stimulator, (2) two standard electrode cables, and (3) rubber electrodes and sponge pockets for electrodes. (B) Illustrates additional components required for intrascanner tDCS: (4) stimulator cable, (5) electrode cable equipped with resistors, (6) outer and (7) inner filter boxes, (8) box cable to connect the two filter boxes, and (9) MRI-compatible rubber electrodes. Please click here to view a larger version of this figure.
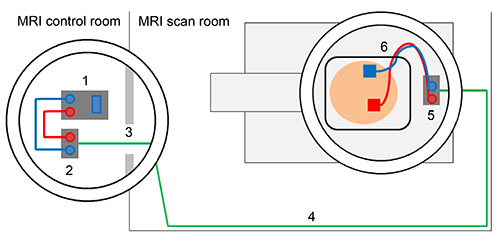
Figure 3. Schematic overview of tDCS set-up outside and inside of the scanner. Direct current stimulator (1) is connected with outer filter box using stimulator cable (2). Box cable enters scanner room through radio frequency filter tube (3). Box cable should be aligned with the wall of the MRI scan room (4) and connected to inner filter box that is positioned inside the MRI scanner (5). Electrodes are attached to the head of the subject and electrode cable is fed through the lower left part of the head coil and connected with the inner filter box (6). Please click here to view a larger version of this figure.
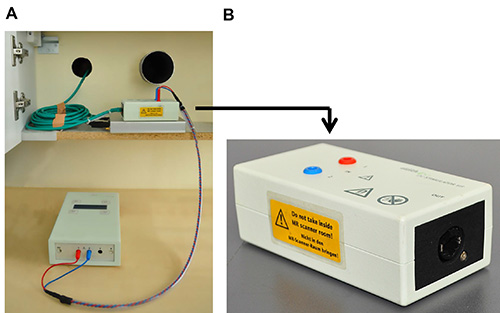
Figure 4. Details of set-up inside of the scanner. (A) Shows placement of outer filter box in the vicinity of the radio frequency filter tubes and box cable that is inserted into the left filter tube. (B) Close-up of outer box that is not MRI-compatible. Please click here to view a larger version of this figure.
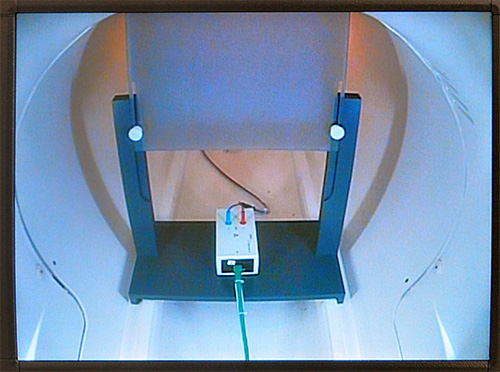
Figure 5. Placement of inner filter box. This figure illustrates the position of inner filter box inside of the scanner (rear end). Filter box is placed underneath a screen on which experimental stimuli are presented using a projector. Please click here to view a larger version of this figure.
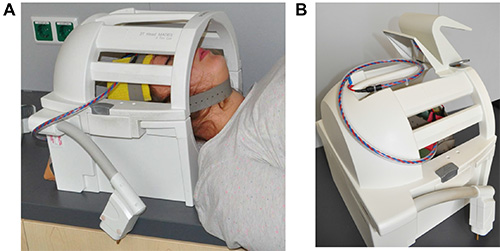
Figure 6. Placement of electrode cable. This figure shows the closed head coil of the scanner. (A) The subject’s head is positioned in head coil with the electrodes attached to the head with rubber electrodes. Electrode cable exits head coil at the lower left side. (B) Electrode is placed on top of the head coil when moving the subject into the scanner bore. Please click here to view a larger version of this figure.
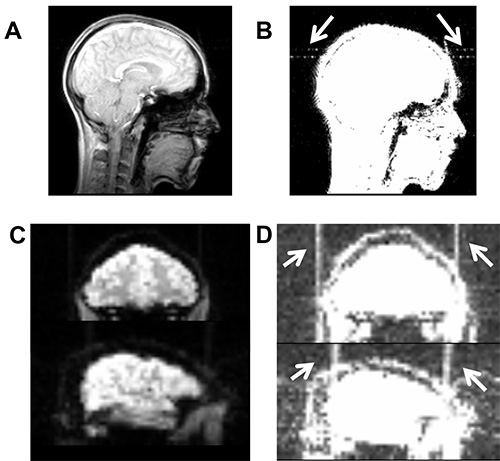
Figure 7. Illustrates high-frequency artifacts induced by a broken cable. (A) Artifact is not visible on axial slice of the localizer scan using the standard contrast in MRIcron (www.mrico.com). (B) Artifact becomes visible after adjusting the contrast settings (white arrows, contrast settings 0-20). Similarly, high-frequency artifact is not visible in functional imaging sequence using default contrast (C), but becomes visible after adjusting contrast (D). Please click here to view a larger version of this figure.
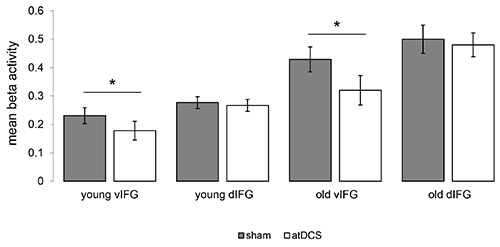
Figure 8. Impact of atDCS on task-related functional activity. Illustrates significant reductions of task-related activity during the semantic word-generation task in the ventral portion of the inferior frontal gyrus (vIFG) in younger and older adults (atDCS < sham, both p<0.05). No significant differences were found in the left dorsal IFG (dIFG) in both groups. Please click here to view a larger version of this figure.
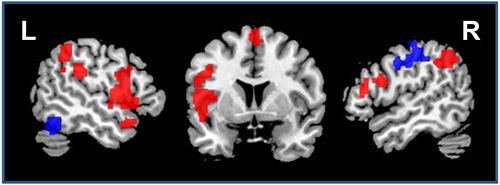
Figure 9. Impact of atDCS on resting-state functional connectivity. Illustrates regions that showed enhanced (red) or reduced (blue) connectivity during atDCS compared to sham stimulation during the resting-state scan (sagittal slices x=-52/52, coronal slice z=5). L=Left hemisphere, R=Right hemisphere. Please click here to view a larger version of this figure.
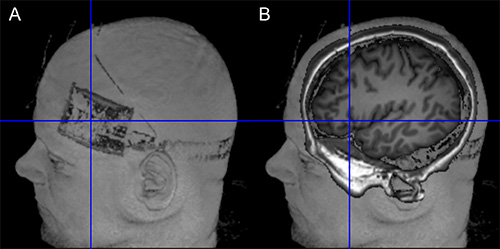
Figure 10. Verification of target position. (A) The left side of the figure shows the location of the electrode on the scalp (Surface rendering based on T1-weighted image using MRIcron). (B) The right side of the image illustrates the projection of the electrode center into the brain of the same subject. Orientation of image is identical in both images. Please click here to view a larger version of this figure.
