By following the procedure above, each stage of the surgery should mimic the results for each stage of the surgery outlined in Figure 2. Special care must be taken when applying the silicone elastomer to eliminate air bubbles under the glass or at least ensure that they are located at the periphery of the area of interest (Figure 2L). For an experienced surgeon, surgical complications requiring euthanasia either during surgery or within the first 24 hr postsurgery occur in approximately 20% of operations. These complications most frequently arise from excessive soft tissue hemorrhaging or failure to securely attach the chamber to the vertebral column.
In successfully implanted chambers, the window typically remains optically transparent for multiple weeks (Figure 3). Despite best efforts, an opaque, fibrous, neoplastic growth often forms within a few days, resulting in partial obscuring of the window (Figure 3C – F, black dashed line). Fluorescent structures are difficult to see using 2PEF microscopy underneath this fibrous tissue. We find a bimodal distribution of results, with approximately 50% of successfully implanted windows remaining clear for more than 5 weeks postoperatively, and approximately 50% becoming obfuscated within 1 – 3 weeks. For windows that remain clear, most places within the viewing window experience only a modest degree of neovascularization in or above the dura (Figure 3D – F, green asterisks), which does not hinder 2PEF imaging. Our previous study30 showed an increase in microglia but not astrocyte density under the window and adjacent vertebrae, indicating mild inflammation analogous to that seen in cranial window preparations5.
In transgenic mice expressing yellow fluorescent protein (YFP) in a subset of dorsal root ganglia (DRG) neurons (YFPH line; Jackson Labs), axons were clearly distinguishable for weeks post-operatively (Figure 4A and b) and as long as four months in one animal (data not shown). Blood vessels (Figure 4A and B) were made visible by retro-orbitally injecting fluorescent Texas Red labeled dextran into the blood plasma. Microglia were also visualized in mice expressing GFP in a CX3CR1 knock-in mouse (CX3CR1-GFP; Jackson Labs) crossed to the YFPH line (Figure 4C). Contrast and resolution deteriorated modestly over time (Figure 4C) due to the formation of a fibrous overgrowth described previously30. We routinely imaged for 3 hr in a single session without mortality and as often as every 12 hr. Session duration and frequency is limited by the tolerance of the animal for anesthetic induction, concomitant with the ethical considerations accompanying pain and distress to laboratory animals.
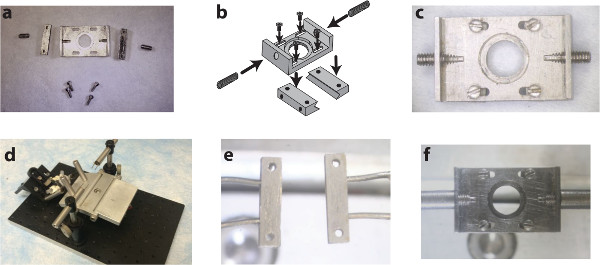
Figure1. A custom surgical suite facilitates chamber delivery during implantation and stabilizes the chamber during subsequent imaging sessions. Two side-bars and a top plate (A) are assembled (B) using small screws into the spinal chamber (C). A surgical table with extendable posts (D) allows for the delivery and clamping of the side-bars to the vertebrae using holding pins (E). Subsequent imaging sessions instead use internally threaded posts to attach to the chamber via the set screws on the wings of the implant (F). Panel b of this figure has been modified from Farrar et al., Nature Methods, 201230 with permission from Nature Publishing Group. Please click here to view a larger version of this figure.
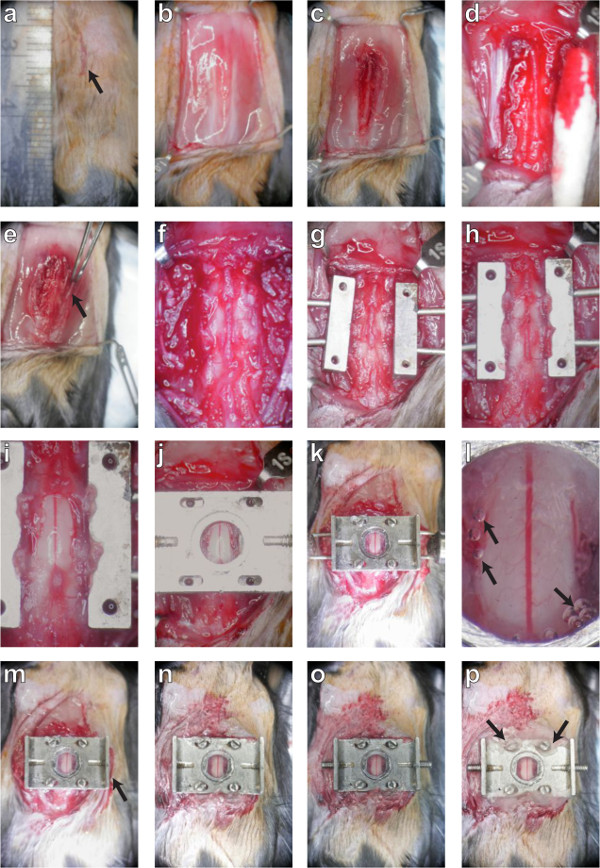
Figure 2. A dorsal laminectomy is performed and a chronic imaging chamber is implanted to provide optical access to the spinal cord. The procedure is described in montage. First, the skin (panels A, B; protocol sections 3.1 – 3.4) and muscles (C; 3.5) are retracted to expose the three underlying vertebrae. The tissue overlying these three vertebrae is removed (D, E, F; 3.6 – 3.10) and the lateral processes are scraped clean before they are clamped on both sides (G, H; 3.12). Carefully, the dorsal lamina of the central vertebra is removed and the edges of the bone sealed (I; 4. 6). A top plate is applied (J; 5.1) and screws fastened into position (K; 5.3) to secure the chamber before sealing the chamber with silicone elastomer and cover glass (L; 5.5). After the delivery pins are removed (M; 5.8), the skin is glued to the sides of the chamber (M, N; 5.8) and the set screws are inserted into the wings (O; 5.9). Finally, the screw slots are sealed with dental acrylic (P; 5.10) and the mouse is placed in a clean cage to recover. Please click here to view a larger version of this figure.
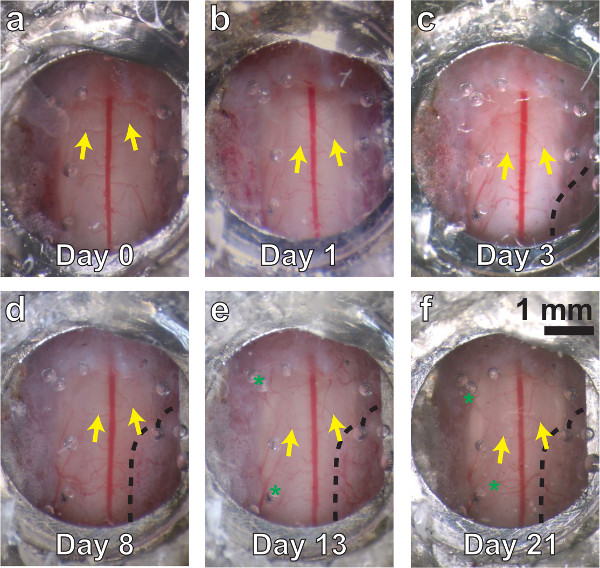
Figure 3. A chronic spinal chamber remains optically transparent over multiple weeks. White light images of the spinal cord, ranging from several minutes (A) to three weeks postoperatively (F). Vascular landmarks are identifiable at all time points (yellow arrows). Little change is seen at one day postsurgery (B). Dense fibrous overgrowth (C – F, bounded by dashed line on lower right) is present as early as three days and results in partial obfuscation of the imaging area. Mild neovascularization (D, E, F, green asterisks) is also present, but does not obscure the original vasculature in white light or 2PEF imaging.Please click here to view a larger version of this figure.
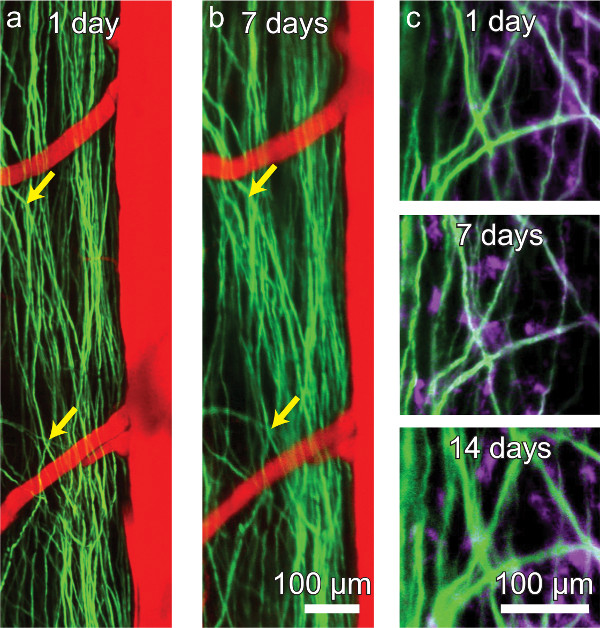
Figure 4. A chronic spinal chamber allows for repeated multi-photon imaging without the need for repeat surgeries. Repeated imaging of transgenic mice expressing YFP in a subset of DRG axons (green) in the dorsal funiculi of the spinal cord and vasculature (red) labeled by intravascular dye injection (A, B). The activity of microglia (mauve) can also be tracked over time in Thy1-YFP/CX3CR1-GFP double transgenic mice (C). While axons and microglia remain visible, contrast and resolution decline modestly over time (C). Please click here to view a larger version of this figure.
