The aim of this method was to induce an ischemic stroke in animal models (mouse and rat) following a bolus injection of RB through the tail vein and subsequent illumination of a thinned skull with a 561 nm laser light. The images in Figure 4 demonstrate the progression of clot formation within a single vessel following irradiation of the area at 0, 1, 1.5 and 2 min. Prior to clot formation the entire vessel is white due to free flowing Rose Bengal. Following the induction of irradiation of the vessel there is an obvious darkening in portions of the vessel and indicates the induction of clot formation (frames 1 and 1.5 min). Following complete occlusion there is a marked accumulation of Rose Bengal dye (white area) preceding the clot (black area) within the vessel. The 2 minute frame demonstrates the complete occlusion of the artery.
To verify the presence of an ischemic stroke TTC staining can be utilized. TTC is a commonly used stain for the detection of cerebral infarction by the formation of red formazan TTC products in healthy tissue. The lack of formazan production (white tissue) indicates the infarct area. The areas indicated by the boxes in Figure 5 demonstrate the typical lesion sizes obtained 1 and 5 days from two separate animals following a clot produced within a vessel approximately 80mm in diameter. Image analysis is performed on a flat bed scanner and the use of ImageJ software. Regions of interest can be drawn within ImageJ to measure the area of the stroke volume for each brain.
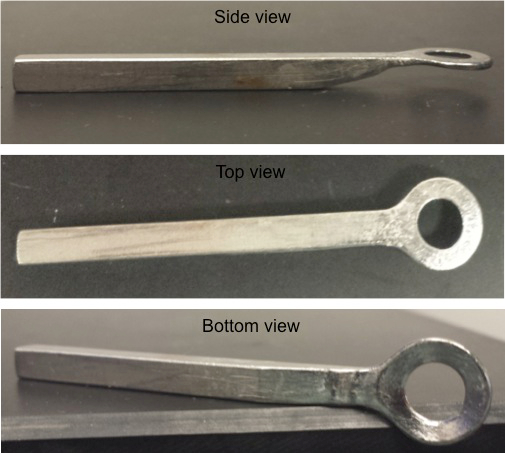
Figure 1: Stainless Steel Ring. Three views (top, side and bottom views) are shown of the stainless steel ring holder that is applied to the skull of the mouse to affix it to the stereotaxic holder.
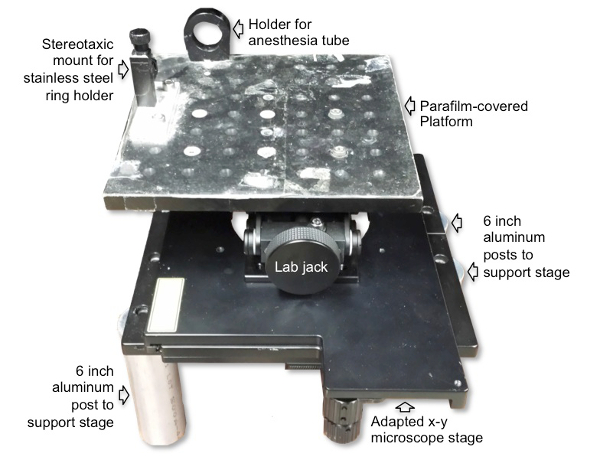
Figure 2: Microscope imaging platform setup for RB photothrombosis. The surgical/imaging platform contains a holder for the anesthesia tube with nosecone and a stereotaxic holder for the stainless steel ring that is affixed to the skull of the animal to decrease movement of the animal during imaging. The platform is placed on top of and secured to the laboratory jack to allow vertical movement for positioning the mouse under the microscope objective. The laboratory jack is then attached to a microscope stage, which allows for horizontal movement. The microscope stage is placed on top of and secured to four cylindrical poles.
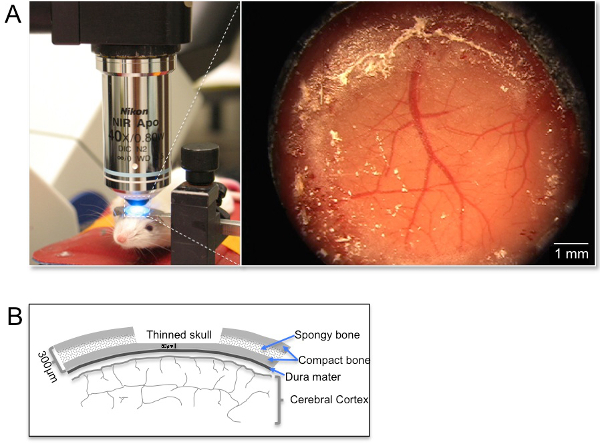
Figure 3: Picture of imaging/surgical platform design and orientation under the objective inverter. (A) The panel on the left demonstrates a representative image of the positioning of an anesthetized mouse (anesthesia nose cone was removed briefly for taking the picture). Note the use of a custom steel ring to attach the mouse skull to decrease the contribution of breathing artifacts throughout the imaging procedures. The image on the right demonstrates an image of the cortical window under a dissecting microscope. (B) Sketch of the thin skull preparation from a coronal view demonstrating the layers of the skull in relation to the dura mater and the thickness of the thinned area in relation to the full skull thickness.
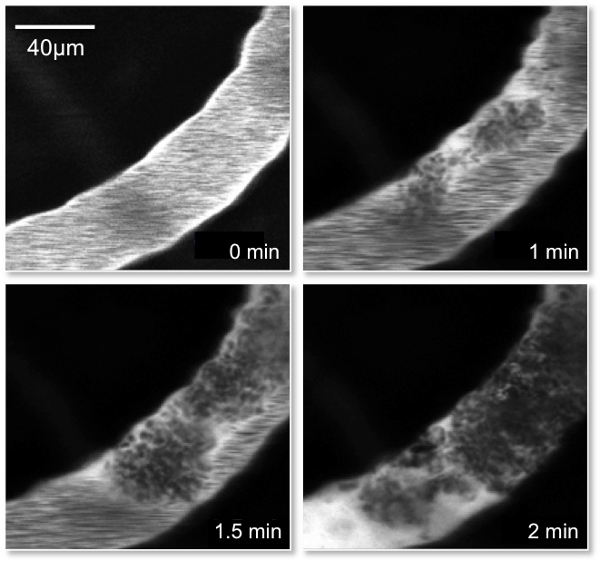
Figure 4: Picture of Rose Bengal Clot formation. Representative images of a single vessel containing Rose Bengal dye that was injected through the tail vein of the mouse. The images demonstrate the progression of clot formation within the vessel following irradiation of the area at 0, 1, 1.5 and 2 min. Note the accumulation of the Rose Bengal dye (white) preceding the clot (black) in the 2 min frame demonstrating the complete occlusion of the artery.
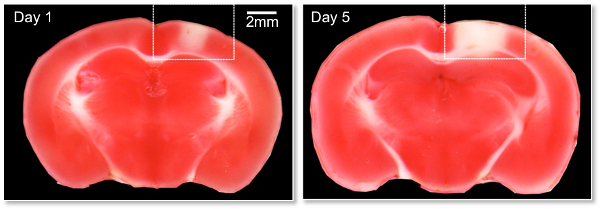
Figure 5: 2,3,5-triphenyltetrazolium chloride (TTC) image of RB induced lesion. Representative images are shown on Day 1 and 5 post-photothrombosis induction. The mice were sacrificed and the brains rapidly removed and sliced into 1mm coronal sections and stained with TTC according to standard methods. TTC is a commonly used stain for the detection of cerebral infarction by the formation of red formazan TTC products in healthy tissue. The lack of formazan production (white tissue) indicates the infarct area. The areas indicated by the boxes demonstrate the typical lesion sizes obtained following a clot produced within a vessel approximately 80 µm in diameter.
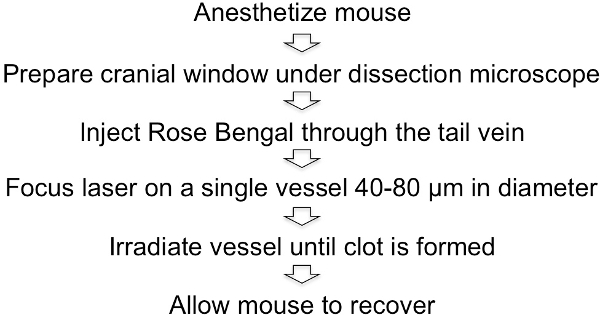
Figure 6: Schematic representation of the Rose Bengal photothrombotic procedure.
