Injection of Syngeneic Murine Melanoma Cells to Determine Their Metastatic Potential in the Lungs
Summary
Metastasis plays a profound role in the virulence of cancer, accounting for an estimated 90% of deaths. We report a protocol for a metastatic melanoma model in mice that is useful for determining the efficacy of therapeutic agents against this clinical phenomenon.
Abstract
Approximately 90% of human cancer deaths are linked to metastasis. Despite the prevalence and relative harm of metastasis, therapeutics for treatment or prevention are lacking. We report a method for the establishment of pulmonary metastases in mice, useful for the study of this phenomenon. Tail vein injection of B57BL/6J mice with B16-BL6 is among the most used models for melanoma metastases. Some of the circulating tumor cells establish themselves in the lungs of the mouse, creating “experimental” metastatic foci. With this model it is possible to measure the relative effects of therapeutic agents on the development of cancer metastasis. The difference in enumerated lung foci between treated and untreated mice indicates the efficacy of metastases neutralization. However, prior to the investigation of a therapeutic agent, it is necessary to determine an optimal number of injected B16-BL6 cells for the quantitative analysis of metastatic foci. Injection of too many cells may result in an overabundance of metastatic foci, impairing proper quantification and overwhelming the effects of anti-cancer therapies, while injection of too few cells will hinder the comparison between treated and controls.
Introduction
Metastasis is a major cause of death among patients with malignancies. The process of metastatic dissemination of cancer cells is poorly understood but appears to involve several steps, including invasion of adjacent tissues, intravasation into the lymphatics and vasculature, survival and translocation within the circulatory system, extravasation from the vasculature at the site of metastasis, adaptation to the new microenvironment of the new site, and colonization at the new site by proliferation and formation of secondary tumors.1 Each of these biological events involve the transformation, dissemination and survival of metastatic tumor cells. For example, the transformation of the epithelial phenotype of the tumor cell into a mesenchymal phenotype, coupled with the successful interaction with the extracellular matrix, enable them to invade adjacent tissues and metastasize to other parts of the body.2,3 Furthermore, these metastatic cells must survive within the circulating bloodstream and evade immune surveillance from the host.4,5 Finally, when implanted at a distant site within the body, the tumor cells must adapt to their microenvironment in order to proliferate and form secondary tumors.6,7 Therefore, although metastasis is a common phenomenon among cancer patients, metastatic tumor cells have multiple areas of vulnerability that are amenable to therapeutic intervention.
Given the immunogenic nature of melanoma, and the recent interest in immunotherapies, models for melanoma are increasingly useful.8 In the United States alone, melanoma is the cause of an estimated 9,000 deaths per year.9 Common locations of melanoma metastasis are bones, brain, liver, and lungs. The majority of metastases to distant sites occur through the bloodstream. Circulating tumor cells in the blood must evade immune clearance, reach a capillary bed of a distal organ and invade through the endothelial cells of the blood vessel in order to successfully establish themselves.4-7,10, 11
To mimic the common and virulent phenomena of metastasis, the murine B16-BL6 cell line was created. A decedent of the parental C57BL/6 melanoma cell line B16-F0, B16-BL6 is the end product of 10 successive selections for lung metastasis from intravenous injection (resulting in B16-F10), followed by 6 successive selections for bladder membrane penetration.12 As such, it is a reliable melanoma cell line for the establishment of metastatic foci in the mouse, particularly when injected intravenously.13
After injection of a sufficient quantity of B16-BL6 cells into the tail vein of a B57BL/6 mouse, followed by two or more weeks to allow implantation and growth of the B16/BL6 cells, metastatic foci will form in the lungs. Upon euthanasia and inspection by dissecting microscopy, the number of individual foci present can be quantified. This, in turn, can be used to establish a dose-metastasis effect, as the number of injected B16-BL6 cells correlates with the number of foci formed on the surface of the lungs. This model is known as "experimental metastasis," where known-metastatic cells are introduced directly into the bloodstream, facilitating a rapid and predictable spread and establishment in the lungs, liver, or other organ of investigation. This is in contrast to "spontaneous metastasis," where tumor cells are implanted, often subcutaneously, and metastases originate from organically shed cancer cells.14,15
It is important to inject an appropriate quantity of B16/BL6 cells into the tail veins of the mice. Too many, and the lungs will be covered with metastases and neighboring foci will be indistinguishable from one another. Too few, and the influence of a therapeutic agent will be indiscernible due to inherent variations between injections. In order to obtain an optimal number of foci on the lungs of the C57BL/6 mice, it is necessary to correlate the number of injected cells with the quantity of established metastatic foci on the surface of the lungs while taking into account the distinguishability of individual foci. This protocol will demonstrate a metastatic murine melanoma model for C57BL/6 mice.
Protocol
Ethics Statement: The use of mice in research is only acceptable in instances where it might advance human understanding of fundamental biology or towards the eventual treatment of disease.
1. Ordering
- Purchase female C57BL/6 mice (age of 6 – 8 weeks), 5 mice per group. Allow several days for the mice to adjust.
2. Preparation of B16-BL6 Cells
- Remove cell culture plates from 37-degree incubator and place in a sterile hood. Plates should be approximately 70% confluent with B16-BL6 murine melanoma cells. A greater confluence may alter the cells metastatic potential.
- Add 1 ml of 0.05% Trypsin-EDTA per plate, let sit for 1 min, and then aspirate the trypsin-media solution.
- Add 1 ml of trypsin per plate and return plates to the incubator for 10 min.
- After moving the plates from the incubator to the sterile hood, add 4 ml of serum-free Rosewell Park Memorial Institute Medium (RPMI) to each plate.
- Collect the cells with a sterile, motorized pipette. Eject cells against the bottom of the plate, with the tip pressed at a very slight angle, to break up the cells. Repeat several times in order to ensure adequate separation of cell clumps, which might otherwise clog the ejection needle. Recollect and transfer to a 50 ml conical tube.
- Use a hemocytometer to determine the cell density. Keeping the total number of B16-BL6 cells constant, determine the volume of serum-free RPMI needed to reach final concentrations of 0, 0.065, 0.015, 0.25, and 0.5 million cells/ml.
- Equally aliquot the media in the 50 ml tube to 15 ml conical tubes. Centrifuge the conical tubes at 2,250 x g for 5 min. Decant the media. Add an appropriate volume of serum-free RPMI and confirm the desired cell density via hemacytometer. Adjust densities- by adding additional RPMI or spinning and resuspending in a smaller volume- accordingly.
- Aliquot 500 µl of each cell suspension into labeled 1.8 ml tubes on ice.
3. Tail Vein Injection
- Take a mouse, held by the tail, and guide it rear-first into the mouse restrainer. With the torso in the main chamber of the restrainer, with the tail outside it, pull the mouse towards the end of the restrainer. Insert the restrainer-plunger, continuing to push until the mouse is secure.
- Rotate the mouse 90 degrees such that one of the lateral tail veins is facing upwards. Using an alcohol pad, vigorously clean the side of the mouse's tail, particularly where the tail vein is most visible.
Note: Good lighting is essential for effective tail vein visualization on B57BL/6J mice. Heat lamps or heated surgery pads, while not necessary, will also help by increasing the volume of the tail vein. - In a sterile culture hood, collect 300 µl of cell culture media from the 2 million cells/ml tube. Invert the needle, flicking the side and pushing the plunger, to eject bubbles from the syringe. Eject culture-RPMI to result in a final volume of 250 µl.
- Extend the mouse-tail with non-dominant hand. Hold the tail with the proximal end of the tail elevated with the forefinger of the non-dominant hand, and the distal portion of the tail depressed with the thumb.
Note: In this way, the tail vein is held in a lateral position, parallel to the restrainer surface, with a congruent entry possible in the more distal part of the tail. - Insert the needle into the tail vein, towards the distal end, at a minute downward angle to begin with, and then adjust the needle to match the angle of the tail vein upon further insertion (lowering plunger end of the syringe relative to the needle).
- Insert the needle approximately 1 cm into the tail vein. After insertion, begin to push the plunger, holding the needle steady.
Note: If the needle is in the tail vein and the end of the needle is not obstructed the media should flow unimpeded into the vein. Effective injection is characterized by blood clearance from the vein. If there is resistance, or a bubble begins to form at the site in injection, remove the needle and try again at a more proximal location along the tail vein. - Remove the needle from the vein and discard it. Hold gauze against the entry site to stop any bleeding.
- Remove the plunger from the restrainer and place the mouse in the recipient cage.
- Repeat for all other concentrations.
Note: Lung foci establishment takes approximately 2 – 3 weeks, with variability depending on cell line and the desired size of the foci.9 In the interim, mice should be monitored for symptoms that could warrant early euthanasia, like excessive panting.
4. Counting the Lung Foci
- Euthanize the mouse by placing in a CO2 chamber and exposing to 100% CO2 introduced at 10-30% of chamber volume per minute for 5 min. Follow with a cervical dislocation.
- Splay the mouse on Styrofoam. Using surgical scissors, create a surgical incision along the sternum.
- Make two additional incisions, both from the top of the sternum incision and branching towards the shoulders of the mouse, exposing the rib cage.
- Make two cuts, each along the lateral sides of sternum, to remove the rib cage from the torso, exposing the lungs and heart.
- Holding the heart with surgical tweezers, cut the esophagus and windpipe, freeing the heart and lungs from the mouse. Place beneath a dissecting microscope, at 10X magnification, for better visualization.
- Dissect the heart from the lungs and remove the thymus, leaving only the two lungs.
- With the lungs beneath a dissecting scope, begin to count the lung foci. Each foci should appear as a circular, brown obtrusion on the surface of the lungs.
- For consistency between mice, count the number of foci on the surface of a lobe, and then invert that lobe. Doing each of the four lobes individually allows for easier counting.
- Save and fix the lungs if performing IHC, otherwise, discard the remains.
Representative Results
Upon visual inspection, the variation in surface foci is evident. Counting the number of tumors under a dissecting microscope should yield a linear relationship between the number of injected tumor cells and number of resulting and countable foci. Using an optimal number of injectable cells, the goal is one where the lungs are not completely covered, as they are at 500,000 cells/ml in Figure 1A, and not too sparsely covered, as they are at 62,500 cells/ml and 125,000 cells/ml. This is also quantifiable by linear correlation (Figure 1B).
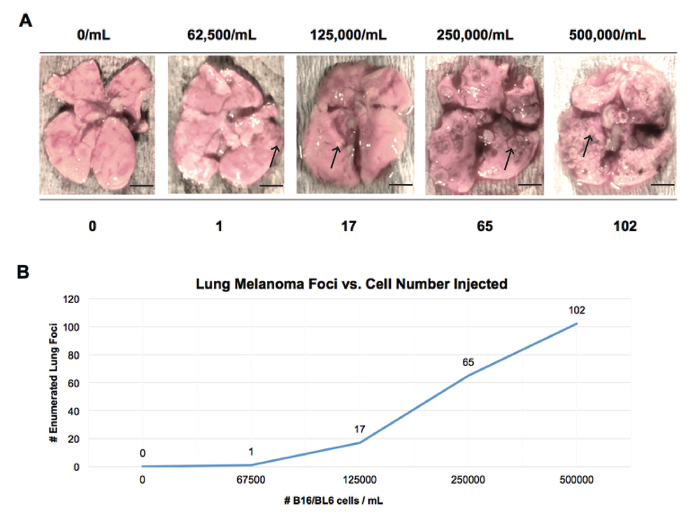
Figure 1. Lung Foci Resulting from Tail Vein Injected B16/BL6 Cells. (A) Lung foci can be visualized on the surface of lungs from C57BL/6 mice as brown circular masses (representative foci under arrows). As the density of the injected cell culture (above each image) increases, so does the corresponding number of resulting lung foci (below each image). The lungs from the mouse with the highest density of injected cells has the greatest visual coverage of lung foci. Scale bars represent 20 mm. (B) Enumeration of the lung foci relative to the cell culture density. There is an approximately linear relationship above 125,000 cells/ml, as determined by hemacytometer. Please click here to view a larger version of this figure.
Discussion
Circulating tumor cells from a tail vein injection represent the metastases that evade sites of primary growth and migrate through routes like the bloodstream or lymphatic system, occasionally establishing themselves in the capillary beds of distant locations.14 The protocol described above serves as a model for secondary metastases. With an optimal number of B16-BL6 cells injected, experimenters can determine the relative effect of an administered drug or immune cell population, post-neutralization, on cancer cell metastasis.
This protocol has limitations. The circulating tumor cells have been selected for their ability to metastasize and are therefore non-immunogenic, having lower levels of major histocompatibility complex class 1 molecules.12 Furthermore, the sudden and clustered introduction of large number of metastases is unlike the typical scenario in patients where small numbers of metastatic tumor cells dissipate over a prolonged period of time from the primary tumor location. Additionally, the intravenously introduced tumor cells are from tissue culture and not of a primary tumor origin. Therefore, these cells are unlike the secondary metastases that result from alterations in cell adhesion, migration, immune recognition and recipient organ establishment.15,16
An alternative protocol would be the subcutaneous injection of B16/BL6 for the generation of primary tumors and the analysis of the resulting "spontaneous" pulmonary metastases. These "spontaneous" metastases have been found to contain more heterogeneity than their "experimental" counterparts, more closely matching those of human patients. The protocol is limiting in its ability to determine the influence of an experimental compound on metastasis. With a lateral tail vein injection, the number of melanoma cells injected into the bloodstream can be approximated via hemocytometer. With "spontaneous" metastasis, however, there is greater heterogeneity between tumors, adding an additional variable to the number of resulting lung foci.16
In conclusion, the tail vein B16-BL6 murine melanoma model represents a simple model for determining the influence of a treatment or immunotherapy on metastasis. By intravenously injecting circulating tumor cells, researchers can replicate, to some extent, patients post-metastasis. Considering the destructive effects of metastatic tumor cells in the cancer patients, this model is a powerful tool for understanding the multistep process of metastasis.
Disclosures
The authors have nothing to disclose.
Acknowledgements
Supported in part by a National Cancer Institute grant 1R03CA172923.
Materials
| Trypsin | Corning | MT25052CV | |
| RPMI 1640 Medium | Corning | MT15040CM | |
| Phase Contraast Hemacytometer | Hausser | 02-671-54 | |
| Micro-Fine IV Insulin Syringes | BD | 14-829-1D | |
| Sterile Alcohol Prep Pads | Fisherbrand | 22-363-750 | |
| Mouse Restrainer | Braintree Scientific | NC9999969 | Restrainer choice depends on age/size of mice |
| Heating Pad | Harry Schein | NC0012697 | Optional |
References
- Chaffer, C. L., Weinberg, R. A. A perspective on cancer cell metastasis. Science. 331, 1559-1564 (2011).
- Kalluri, R., Weinberg, R. A. The basics of epithelial-mesenchymal transition. J Clin Invest. 119 (6), 1420-1428 (2009).
- Stetler-Stevenson, W. G., Aznavoorian, S., Liotta, L. A. Tumor cell interactions with the extracellular matrix during invasion and metastasis. Annu Rev Cell Biol. 9, 541-573 (1993).
- Allard, W. J., Matera, J., Miller, M. C., et al. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant disease. Clin Cancer Res. 10, 6897-6904 (2004).
- Dunn, G. P., Bruce, A. T., Ikeda, H., et al. Cancer immunoediting: from iimmunosurveillance to tumor escape. Nat Immunol. 3, 991-998 (2002).
- Hugo, H., Ackland, M. L., Blick, T., et al. Epithelial-mesenchymal and mesenchymal-epithelial transition in carcinoma progression. J Cell Physiol. 213, 374-383 (2007).
- Kang, Y., Massague, J. Epithelial-mesenchymal transitions: Twist in development and metastasis. Cell. 118, 277-279 (2004).
- Hodi, S. F., et al. Improved survival with Ipilimumab in patients with metastatic melanoma. NEJM. 363 (13), 711-723 (2002).
- Ekwueme, D. U., Guy, G. P., Li, C., Rim, S. H., Parelkar, P., Chen, S. C. The health burden and economic costs of cutaneous melanoma motality by race/ethnicity-United States. J. Am. Acad. Dermatol. 65, 133-143 (2011).
- Alizadeh, A. M., Shiri, S., Farsinejad, S. Metastasis review: from bench to bedside. Tumor. Bio.Volume. 35, 8483-8523 (2014).
- Weinberg, R. A. Is metastasis predetermined. Mol. Oncol. 1 (3), 263-264 (2007).
- Ishiguro, T., Nakajima, M., Naito, M., Muto, T., Tsuruo, T. Identification of genes differentially expressed in B16 murine melanoma sublines with different metastatic potentials. Cancer Res. 56 (4), 875-879 (1996).
- Clark, E. A., Todd, R. G., Lander, E. S., Hynes, R. O. Genomic analysis of metastasis reveals an essential role for RhoC. Nature. 406, 532-535 (2000).
- Terranova, V. P., Hic, S., Diflorio, R. M., Lyall, R. M. Tumor cell metastasis. Crit. Rev. Oncol. Hematol. 5 (2), 87-114 (1986).
- Elkin, M., Vlodavsky, I. Tail vein assay of cancer metastasis. Curr Protoc in Cell Biol. , (2001).
- Hagedorn, H. G., Bachmeier, B. E., Nerlich, A. G. Synthesis and degradation of basement membranes and extracellular matrix and their regulation by TGF-beta in invasive carcinomas (Review). Int. J. Oncol. 18 (4), 669-681 (2001).
- Hart, I. The selection and characterization of an invasive variant of the B16 melanoma. Am J Pathol. 97 (3), 587-600 (1979).
- Overwijk, W. W., Restifo, N.P. B16 as a Mouse Model for Human Melanoma. Curr Protoc Immunol. 20 (1), (2001).
