Tissue Engineering
For bone tissue engineering purposes, a number of different bone substitutes were implanted in the small animal rat AV loop model27,28,33,34. Vascularization could perfectly be demonstrated by 3D micro-computed tomography (micro-CT) (Figure 3A). Vascularization of a processed bovine cancellous bone (PBCB) matrix was significantly higher in the loop group compared to the group without vascularization. A constantly growing and maturating blood vessel network developed within the implantation chamber over 8 weeks. Between 4 and 8 weeks, continuous growth of the vascularized tissue towards the center of the constructs was observed, whereas no increase was detected in the non-vascularized group33. Prevascularization of the PBCB matrix for 6 weeks in the AV loop model led to superior survival of the injected osteoblasts compared to the control osteoblasts. In contrast to the control groups, expression of bone-specific genes was detected in the AV loop group with implanted osteoblasts28. As a further matrix, sintered bioactive glass together with fibrin gel was implanted in the AV loops of the rats. After 3 weeks, a dense network of newly formed vessels has developed demonstrated by micro-CT and histology27.
The implantation chamber was modified in order to accelerate scaffold vascularization. By using a perforated titanium chamber, intrinsic vascularization was supported by extrinsic vessels from the surrounding tissue. At just 2 weeks after implantation of a β-tricalciumphosphate hydroxyapatite (β-TCP/HA)/fibrin matrix, 83% of the vessels were connected to the AV loop with continuous increase over time and reached 97% connection after 8 weeks34. With the implantation of 5 x 106 bone marrow derived mesenchymal stem cells (MSC) and bone morphogenetic protein 2 (BMP-2), a significant increase in bone formation compared to the BMP-2 or MSC alone groups could be induced. At 6 and 12 weeks, the fibrin matrix was completely degraded and replaced by highly vascularized connective tissue in all groups (Figure 3B 6 week implantation). There was a significant decrease in vessel number in the BMP-2/MSC group between 6 and 12 weeks and after 12 weeks in the other groups. This was probably due to maturation of the vascular network or the compact arrangement of bone structures leading to a limited vascular network formation32.
Besides bone, other tissues such as muscle or liver can also be engineered in the AV loop model.
For engineering axially vascularized muscle tissue, experiments with primary myoblasts in an AV loop fibrin matrix were carried out. After a prevascularization time of 2 weeks for 2, 4, and 8 weeks, 1 x 106 myoblasts were transplanted into the AV loop chamber. Transplanted myoblasts could be redetected even after 8 weeks using carboxyfluorescein diacetate succinimidyl ester (CFDA) labeling. The cells kept their myogenic phenotype within the fibrin matrix and expression of the muscle-specific markers MEF-2 and desmin was positive after 4 weeks. However, myogenic marker gene expression was negative after 8 weeks, which was probably due to the absence of myogenic stimuli and rapid absorption of the fibrin matrix35. To increase myogenic stimulation, a new modification of the rat AV loop was developed using the epigastric vein instead of the saphenous vein in order to achieve a more proximal positioning of the isolation chamber. Hence, additional incorporation of the obturator motor nerve was geometrically facilitated. By using this AV loop modification, which is referred to as the EPI loop, we could show myogenic differentiation of co-implanted myoblasts and MSC36.
For hepatic tissue engineering 4 x 106 pkh-26 labeled fetal liver cells were transplanted within a fibrin matrix in the rat AV loop model for 2 weeks. In the control group, matrices without an AV loop and cell-free matrices were implanted. Functional capillaries arose from the AV loop vessels and highly vascularized neo-tissue was observed within the chamber after 14 days of implantation, as shown by CD31 staining and India ink labeling. There was no difference between the cell-free and hepatocyte AV loop group. The AV loop vascularized the fibrin matrix densely and viable fetal cells could be detected after explantation by positive pkh-26 staining and liver cell-specific cytokeratin 18 (CK-18) immunohistology mainly in the proximity of the major vascular axis. mRNA levels of CK-18 were elevated in the AV loop cell group. In contrast, no CK-18 expression could be detected in constructs without a loop or cells37.
Angiogenesis Studies
The AV loop consists of three segments: the vein, the arterial graft and the interpositional venous graft (IVG) segment (Figure 1). Three-dimensional evaluation of the vascular system demonstrated that newly formed vessels originated both from the venous and arterial portion as well as from the venous interponate. A great number of newly formed vessels were observed from the IVG33. With in vivo MRA, scanning electron microscopy of corrosion casts and immune histology, the onset of angiogenesis in a fibrin matrix was observed between day 10 and 14. Above all, the venous and IVG segments gave rise to many capillaries and larger vessels. A gradual reduction in luminal caliber as a sign of arterialization of the IVG due to the increase in endovascular pressure and shear stress was detected from day 7 on38. In further studies, it could be confirmed that vascular sprouting mainly takes place at the non-arterial graft39.
The exact analysis of angiogenesis processes and the stimulation and inhibition of blood vessel formation could be visualized in the AV loop implantation chamber. The growth factors vascular endothelial growth factor A (VEGFA) and basic fibroblast growth factor (bFGF) induced a higher absolute and relative vascular density and faster resorption of the fibrin matrix compared to the growth factor-free control group31. Further, remodeling phenomena and maturation of the vascular network within the isolation chamber were visualized over an implantation period of 8 weeks. In AV loop chambers processes of intercapillary interconnection and intussusceptive angiogenesis as well as possible lymphatic growth were identified immunohistologically as parameters of neovascular maturation39. By applying the PHD (prolyl hydroxylase domain) inhibitor DMOG (dimethyloxallyl glycine) systemically in rats, it could be shown that the concentration of the hypoxia-inducible factor alpha (HIF-α) correlates with the growing vascularization in the AV loop and is a stimulus for vessel outgrowth40.
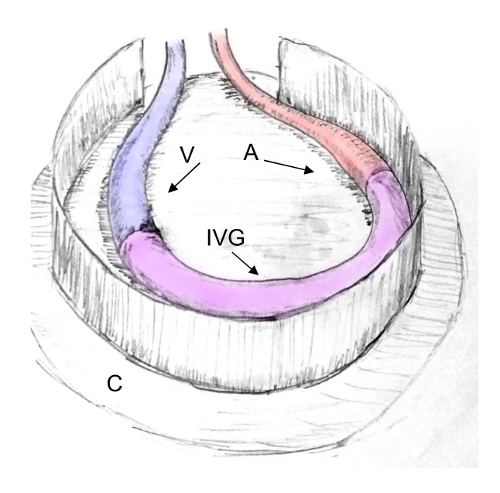
Figure 1: Scheme of an AV Loop in the Rat Model. The AV loop consists of three segments: the vein (V), the arterial (A) graft and the interpositional venous graft (IVG) segment. The AV loop can be embedded into a closed implantation chamber (C) for induction of intrinsic vascularization. Please click here to view a larger version of this figure.
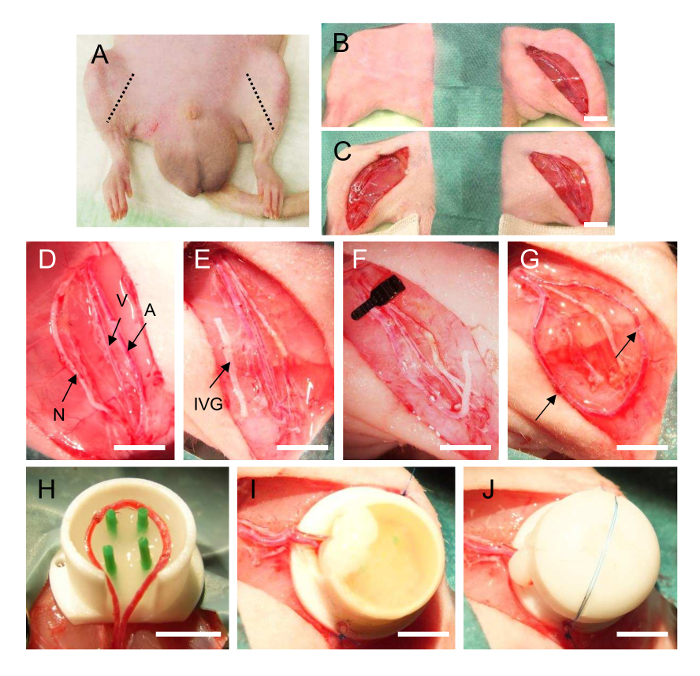
Figure 2: AV Loop Operation in the Rat. (A): Localization of the femoral bundle on the inner side of the hind limbs of the rat. (B/C): Preparation of the femoral vascular bundle in the left and right groin of the rat. The vessels are separated (D), the interpositional vein graft is harvested from the right side (E) and anastomosed with the femoral vein (F) and femoral artery of the left side into an AV loop (G, arrow indicates the anastomoses). The loop vessels are transferred into the implantation chamber prefilled with a matrix (H) and after complete filling (I) the lid is closed (J). A = femoral artery, V = femoral vein, N = femoral nerve, IVG = interpositional venous graft. Scale bar 5 mm (D-J). Please click here to view a larger version of this figure.
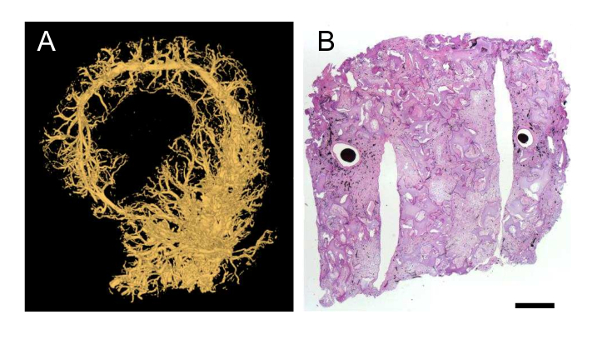
Figure 3: Visualization of Vascularization in the Rat AV Loop Model. (A): Micro-CT after perfusion with a contrast agent (yellow perfused vessels). (B): Hematoxylin-Eosin staining of a β-TCP/HA bone substitute with MSC implanted in the AV loop model rat for 6 weeks. The AV loop vessels are perfused with India ink (black color). Scale bar 1 mm. Please click here to view a larger version of this figure.
