Figure 1 demonstrates the set-up of olfactory fMRI inside and outside of the magnet room, taking into account MR-compatibility. Figure 2a demonstrates a standard fixed-timing paradigm, while Figure 2b demonstrates a paradigm where the "respiration trigger" allows for the synchronization of odor delivery and inhalation.
A regular respiration pattern with clear inhalation peaks is vital to the implementation of an accurate respiration-triggered paradigm. Thus, adjustment of the respiration sensor is an important step in experiment setup. Figure 3 demonstrates sample respiration traces when the respiration sensor was set up incorrectly (Figure 3a) and correctly (Figure 3b). If the respiration pattern is irregular or the respiration signal plateaus, the olfactometer will be unable to accurately determine the respiration pattern, and the odor presentation cannot be synchronized with the subject's inhalation.
With a respiration-triggered, odor stimulation paradigm, the onset and duration vectors for the odor stimulation will vary among subjects. To analyze olfactory fMRI data, the actual onset and duration vectors can be determined with ONSET, and the fMRI data can be processed following standard procedures with these vectors. Figure 4 shows a sample brain activation map responding to respiration-triggered odor stimulation processed by open-source software SPM8 (www.fil.ion.ucl.ac.uk/spm) with actual odor onset and duration vectors following standard processing procedures. Significant odor-related activation was detected in the bilateral primary olfactory cortex, right insular cortex, right supramarginal/angular gyrus, left caudate nucleus, and left postcentral/supramarginal gyrus (family-wise error corrected, p < 0.05, extent threshold = 6 voxels).
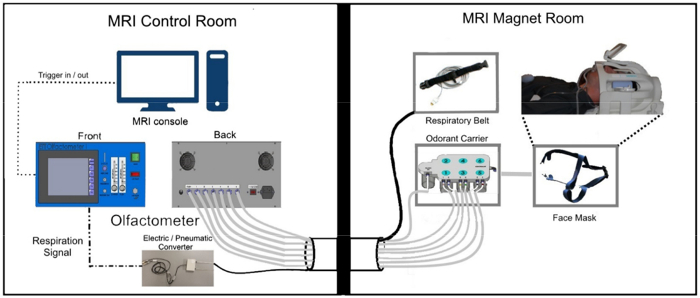
Figure 1: Schematic diagram for experimental set-up. MRI-compatible elements placed in the magnet room are connected to the MRI console and olfactometer box housed in the control room through a penetration panel with a waveguide in the wall that separates the two rooms. Please click here to view a larger version of this figure.
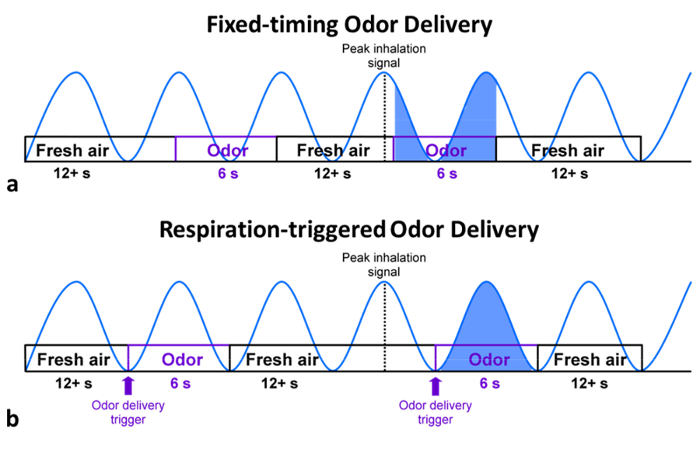
Figure 2: Illustration of odor delivery paradigms. (a) Fixed-timing paradigms, frequent problems in synchronization between respiration and odor delivery lead to variability in the amount and onset of odor delivery in the fixed-timing paradigm. (b) Respiration-triggered paradigms tend to produce more consistent results across subjects. Please click here to view a larger version of this figure.
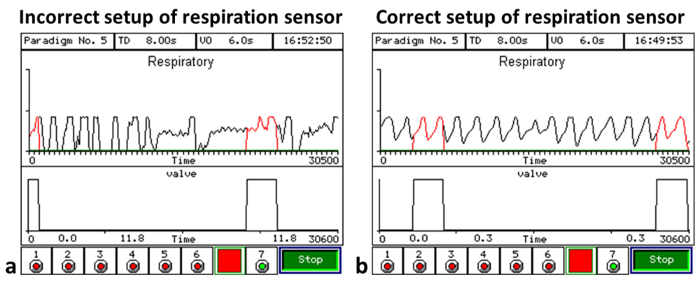
Figure 3: Sample respiratory diagrams. (a) An example respiration trace when the respiration sensor is not set up properly; the respiration patterns plateau and become irregular. (b) A representative regular respiration pattern recorded with a correctly placed respiration sensor; in this case, the respiration patterns are consistent with level peaks, and odor delivery can be synchronized with inhalation. Please click here to view a larger version of this figure.
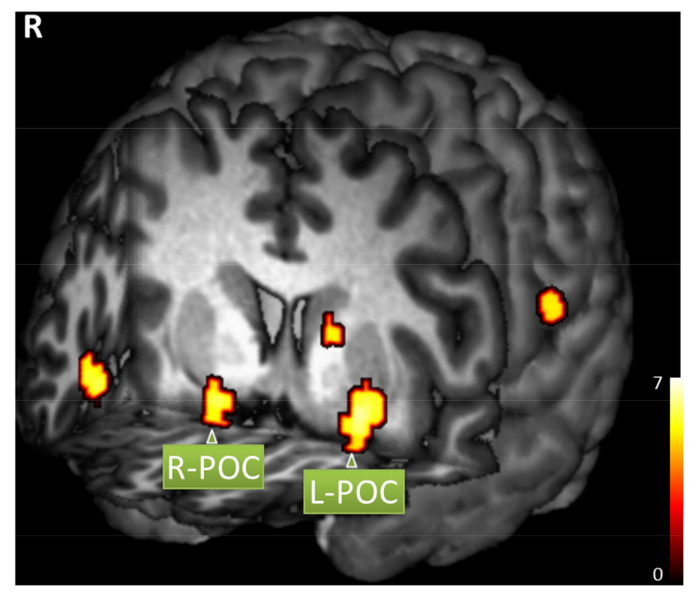
Figure 4: Sample brain activation map. A healthy subject responded to respiration-triggered lavender odor simulation (family-wise error corrected, p < 0.05, extent threshold = 6 voxels). Significant activation includes right primary olfactory cortex (POC, MNI coordinates x = 20, y = 6, z = -14), left POC (x = -22, y = 4, z = -10), right insular cortex (x = 46, y = 20, z = -10), right supramarginal/angular gyrus (x = 66, y = -48, z = 28), left caudate nucleus (x = -14, y = 6, z = 10), and left postcentral/supramarginal gyrus (x = -66, y = -24, z = 20). Please click here to view a larger version of this figure.
| Odorant | Smells like | Compound | Trigeminal stimulation | Solvent |
| Acetaldehyde29 | Green, sweet | Simple | No | Water |
| Ammonia29 | Pungent, cleaner | Simple | Yes | Water |
| Amyl Acetate30 | Banana, apple | Simple | Some | Water |
| n-Butanol31,32 | Mildly alcoholic | Simple | No | Water |
| n-Butyl Acetate31 | Sweet and fruity | Simple | Yes | Water |
| Butyric Acid33 | Sour, rancid | Simple | Yes | Water |
| Citral30,33 | Lemon | Simple | Some | Water |
| Carbon Dioxide34,35 | Odorless | Simple | Yes | N/A |
| Ethyl Butyrate30 | Pineapple | Simple | Yes | Water |
| Eucalyptol35 | Eucalyptus | Simple | Yes | Ethanol |
| Eugenol33,36 | Clove, spicy | Simple | No | Ethanol |
| Geraniol33 | Sweet rose, floral | Simple | No | Ethanol |
| Hydrosulfuric Acid34,36 | Rotten eggs | Simple | No | Water |
| Lavender24,37 | Lavender | Complex | No | Ethanol |
| Menthol33 | Peppermint | Simple | Yes | Ethanol |
| Methyl Salicylate33 | Wintergreen mint | Simple | Yes | Ethanol |
| Patchouli38 | Wet soil | Complex | Yes | Ethanol |
| 1-Propanol31 | Rubbing alcohol | Simple | Yes | Ethanol |
| Phenethyl Alcohol36,39 | Rose | Simple | No | Ethanol |
| Rosemary Oil38 | Rosemary | Complex | Yes | Ethanol |
| Sulfur Dioxide29 | Irritating, pungent | Simple | Yes | Water |
| Valeric Acid33 | Rancid cheese | Simple | Yes | Water |
| Vanillin29 | Vanilla | Simple | No | Ethanol |
| Ylang Ylang38 | Floral perfume | Complex | Yes | Ethanol |
| ***See end of manuscript for references | ||||
Table 1: Common odorants used in olfactory fMRI studies.
