The portal vein injection model, in which tumor cells are delivered directly to the liver via a surgical procedure, allows for tumor cell injection into the portal vein. Under antiseptic conditions, in an anesthetized mouse, a ~1-inch surgical incision is made on the left side of the mouse between the median and sagittal planes, starting just above the plane of the fourth inguinal mammary gland teat and ending just below the ribs. The large and small intestines are gently pulled through the incision to provide visualization of the portal vein (Figure 1A). Accurate anatomical identification of the portal vein and successful intra-portal injection can be confirmed by practicing the injection protocol with India ink or a similar dye. Correct injection via the portal vein will result in the ink being delivered immediately and specifically to the liver, and will not result in India ink spread to the lung (Figure 1B). Further, using D2A1 mouse mammary tumor cells tagged with GFP, dispersal of tumor cells throughout the liver is apparent at ninety minutes post-injection, confirming portal vein injection delivery to the liver (Figure 1C). At higher magnification it becomes apparent that at 90 min post-injection, tumor cells are found within sinusoids, as well as within the liver parenchyma in close proximity to portal triads, where the portal vein blood enters the liver (Figure 1C). These data suggest that active tumor cell extravasation is occurring at 90 min post-tumor cell injection. Taken together, these data confirm that the portal vein injection model delivers the injection volume directly to the liver, with ink or tumor cells dispersed throughout the liver and no appreciable transport of injection volume to the lung.
To assess robustness of the portal vein injection model, three separate syngeneic mouse mammary tumor cell lines were tested in adult female Balb/c mice. These mammary tumor lines were selected based on their characterized behavior in mammary fat pad models and include the highly aggressive and metastatic 4T1 cell line, the less aggressive metastatic D2A1 line, and the low/non-metastatic D2.OR line37,61,73,74. 2,000 and 10,000 cells per injection were tested with no notable differences in the time to development of overt metastasis with these low cell concentrations. For these studies surrogate markers of metastasis were used such as lack of grooming, pallor, and weight loss to justify necropsy, upon which the presence or absence of liver metastases were confirmed by visual assessment of the liver and other organs to confirm intra-portal delivery. These data confirm previous reports that the 4T1 and D2A1 cell lines represent more aggressive mammary tumor lines, as shorter metastasis free survival rates are observed compared to mice injected with the less aggressive D2.OR line (Figure 2A). Mice injected with 4T1 or D2A1 tumor cells developed overt liver metastasis by ~ 30 – 40 days post-injection, and some developed metastasis as early as 18 days post-injection (Figure 2A), whereas only one mouse injected with D2.OR cells had developed overt liver metastasis by study end, which was 60 – 65 days post-tumor cell injection. Metastases were subsequently confirmed by sectioning through the liver in 250 µm levels and analyzing hematoxylin and eosin (H&E) stained sections (Figure 2B-D).
In addition to detection of overt metastatic lesions in the mouse liver, the portal vein model can also be utilized to study earlier events in the metastatic cascade including detection of single cells/cell clusters following extravasation, and formation of micro-metastatic lesions. Multiplex immunofluorescence-staining was used to detect 4T1, D2A1, and D2.OR mammary tumor cells in liver when they are present as single cells or micro-metastatic lesions, as H&E is not sufficient to confirm the presence of small lesions. Figure 3A shows a representative Balb/c mouse liver with a putative micrometastatic foci of D2A1 tumor cells that are positive for the epithelial keratin CK18, negative for the pan-immune marker CD45, and negative for the hepatocyte marker Heppar-1. Hepatocytes also stain positive for CK18, necessitating use of Heppar-1 in this staining panel. One important note is that bile duct epithelium and liver progenitor cells stain positive for CK18, requiring careful discrimination between tumor cells and bile ducts, particularly when assessing periportal regions (Figure 3A). An alternative to multiplex immunofluorescence to identify single disseminated cells and micrometastatic foci is to utilize syngeneic mammary tumor lines tagged with enhanced green fluorescent protein (eGFP) and/or luciferase and perform IHC for the tag (Figure 1C). Due to the immunogenicity of eGFP, luciferase, and other proteins, it is essential to use mouse models that are tolerized to these proteins, such as the novel immune competent "glowing head" mouse that expresses eGFP and luciferase in the anterior pituitary gland75. For identification of macrometastatic lesions of untagged syngeneic lines such as the D2A1 tumor line, the CK18/Heppar-1/CD45 multiplex immunofluorescence is ideal (Figure 3B).
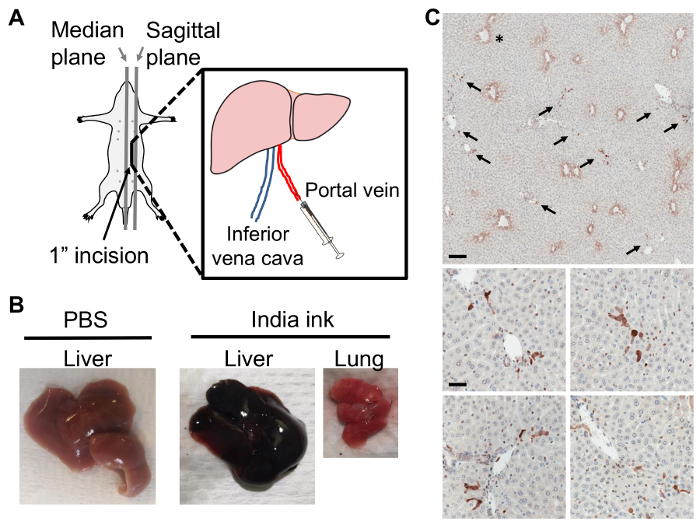
Figure 1: Portal Vein Injection Delivers Tumor Cells Directly to the Liver. A) Portal vein injection; the incision is made between the median and left sagittal planes, from above the plane of the fourth inguinal mammary gland teat and ending just below the rib cage. B) Balb/c liver with PBS injection (left). Following India ink injection via the portal vein, the liver (middle) but not the lung (right) takes up ink. C) Representative thin section images of D2A1 mouse mammary tumor cells tagged with GFP in a Balb/c mouse liver at 90 min post-injection of 1 x 106 tumor cells via the portal vein. Livers were formalin fixed, paraffin embedded, sectioned, and stained with anti-GFP antibody for tumor cell detection. Top panel shows dark brown stained tumor cells (arrows) dispersed throughout the liver, asterisk denotes non-specific hepatocyte staining around central veins; scale bar = 300 µm. Lower panels show representative images of tumor cells at 90 min post-injection still closely associated with vasculature; scale bar = 50 µm. Please click here to view a larger version of this figure.
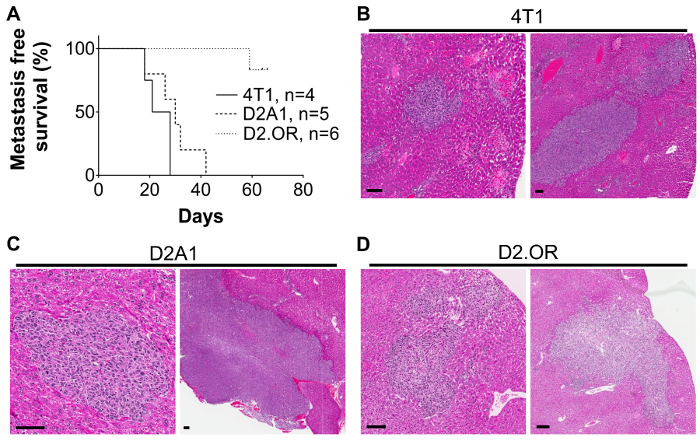
Figure 2: Outgrowth of Mouse Mammary Tumor Cell Lines in the Liver Following Portal Vein Injection. A) Kaplan-Meier curve showing metastasis-free survival rates in mice injected with 2,000-10,000 4T1, D2A1, or D2.OR mouse mammary tumor cells. Mice were injected with tumor cells and monitored for signs of metastasis including lack of grooming, pale eyes, and weight changes. Metastasis was confirmed at time of necropsy and by H&E on histological sections of the livers. N= 2 4T1 2,000 cells; 2 4T1 10,000 cells. N= 2 D2A1 2,000 cells; 3 D2A1 10,000 cells. N= 3 D2.OR 2,000 cells; 3 D2.OR 10,000 cells. Representative H&E images of B) 4T1 lesions at 21 days post-injection of 10,000 cells, C) D2A1 lesions at 26 days post-injection of 10,000 tumor cells, and D) D2.OR lesions at 59 days post-injection of 10,000 cells; scale bars = 75 µm. Similar lesions are observed when 2,000 4T1 or D2A1 tumor cells were injected. No lesions were detected with 2,000 D2.OR cells. No evidence of metastasis in other organs or at the surgical incision site was apparent in any mouse on these studies. Please click here to view a larger version of this figure.
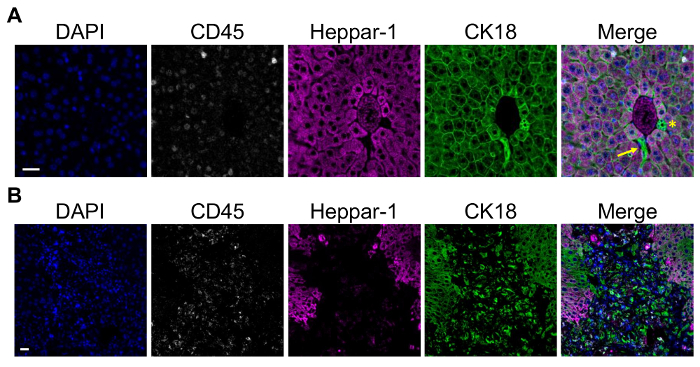
Figure 3: Detection of Single Cells and Metastatic Lesions in the Mouse Liver using Multiplex Immunofluorescence. A) Representative multiplex immunofluorescence of D2A1 tumor cells in a Balb/c mouse liver at 90 min post-injection using the portal vein injection model. Staining was done using a multiplex kit. From left to right shows DAPI; CD45 to mark leukocytes; Heppar-1 to mark hepatocytes; and CK18 to mark tumor cells, hepatocytes, and bile duct epithelium. Merged image shows a putative cluster of CK18+Heppar-1–CD45– D2A1 tumor cells closely associated with a portal triad. Arrow = D2A1 tumor cells, asterisk = bile duct epithelium; scale bar = 25 µm. B) A representative overt D2A1 metastatic lesion using the same staining panel as in A. Tumor cells are CK18+ whereas adjacent hepatocytes are CK18+Heppar-1+; scale bar =25 µm. Images were captured on a microscope with 20 x 0.8, 40 x 1.3, and 60 x 1.4 objectives and CCD camera, using the microscope software. Please click here to view a larger version of this figure.
