Glucose infusion rate during the hyperinsulinemic-euglycemic clamp (insulin sensitivity) was 180.21 ± 19.81 µmol/kg/min. Local application of paraffin oil on the adductor muscle compartment to stabilize the vessel did not change the average baseline diameter of the arteries (73.6 ± 29.0 µm vs. 68.8 ± 17.9 µm; p = 0.58) but helped reduce the variation the animals tested (Figure 4A). Insulin consistently increased the gracilis artery diameter (by 14.58 ± 6.2% at 60 min; N = 9) which was significantly different (p <0.0001) from the diameter change caused by saline infusion (-6.3 ± 4.9%; N = 6). Insulin-induced vasodilation was appreciable after 10 min (10.09 ± 5.1%; p = 0.002) and reached approximately 95% of its maximum dilatory capacity after 30 min.
Using CEUS, insulin consistently increased muscle MBV (Figure 5A) by 33.5% (± 31.04%, N =7; p = 0.0009) when compared to saline infusion (-10.63 ± 27.87%, N = 6) (Figure 5B). The data presented are the signal intensities of the muscle MBV divided by that in the femoral vessels. This reduces experimental variation between different measurements and between different mice (data not shown). The signal intensity in the femoral vessels corresponds linearly with the concentration of microbubbles in the circulation (Figure 3C). Correcting for the femoral vessels' signal theoretically corrects for differences in concentrations of microbubbles used (Figure 3D). Data are presented in this section as mean ± standard deviation.
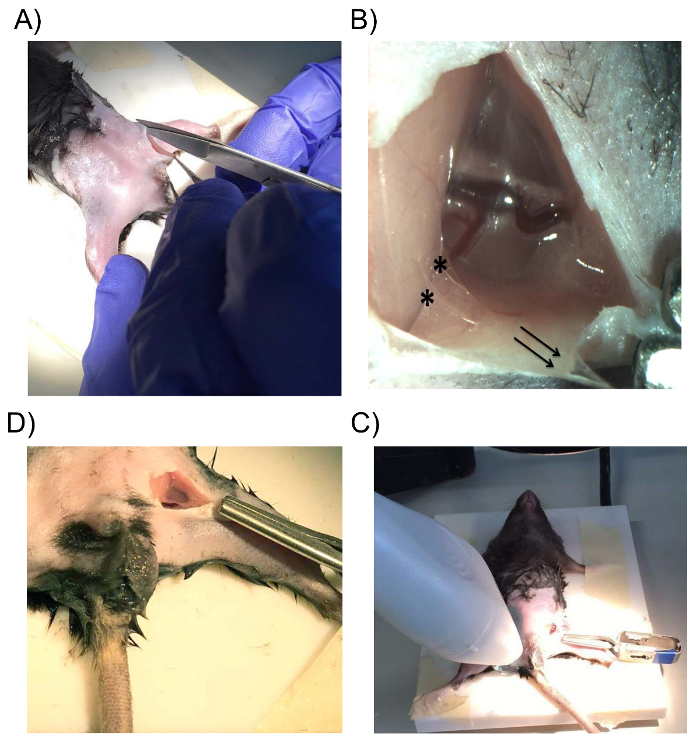
Figure 1: Surgical Exposition of the Adductor Compartment of the Hindlimb. (A) An incision is made at the groin, parallel to the direction of the inguinal ligament. (B) Gentle traction at the fat pad in the distal directions (black arrows) will present the connective tissue (*) between the fat pad and the abdominal wall. (C) The skin folds of the incision can be adjusted using the bulldog clamp to create a small cavity to hold the paraffin oil that bathes the vessels. (D) The ultrasound probe is positioned on the contralateral upper hindlimb after the prepared gracilis artery is viewed using a calibrated microscope. Please click here to view a larger version of this figure.
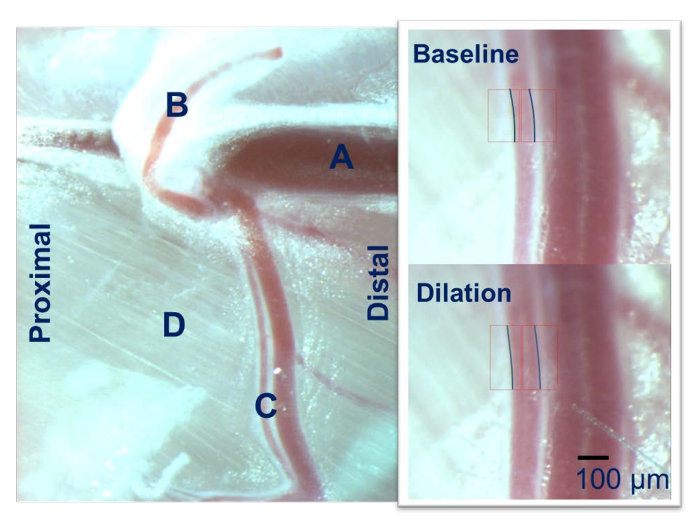
Figure 2: Intravital Microscopy of the Mouse Hindlimb. The femoral artery (A) gives rise to the epigastric artery (B) and the gracilis artery (C) which runs over the adductor muscle group (D). The gracilis artery is used for the IVM using a calibrated microscope. Please click here to view a larger version of this figure.
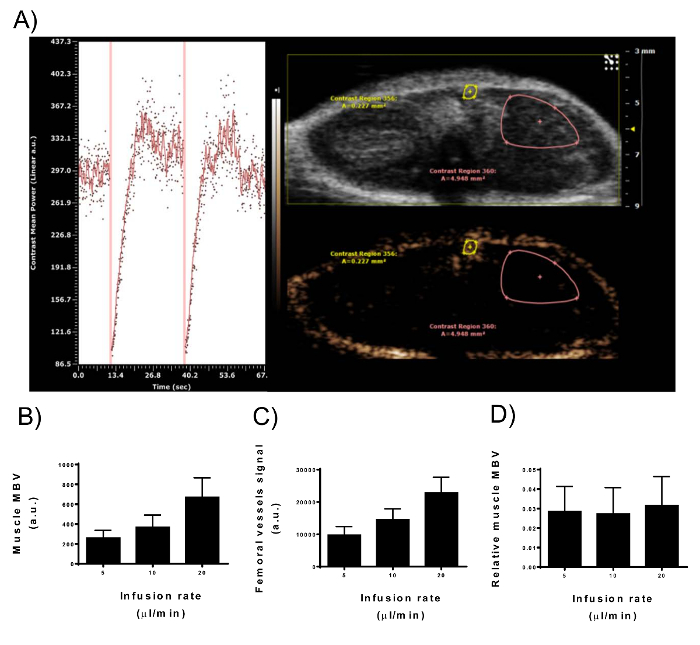
Figure 3: Signal Intensity of Contrast-enhanced Ultrasonography in Muscle Microvascular Blood Volume and Femoral Vessels. (A) View of the nonlinear contrast imaging mode of the digital imaging platform during microbubbles constant infusion in a male mouse upper hindlimb. Right panel: two ROIs are drawn to represent the muscle MBV and the femoral vessels. Only the superficial part of the adductor muscle compartment is included in the ROI as the signal intensity decreases with depth. Left panel: time-intensity curve from the muscle MBV ROI. Vertical lines represent the destruction of the microbubbles (MBD) with high energy waves. Immediately after the MBD, no contrast agent is present in the imaging plane which starts to fill with microbubbles gradually. After 10-15 s, the peak of the contrast enhancement has been reached. (B–D) After a steady-state signal was reached, the infusion rate of 2.5 x 109 bubbles/mL was doubled (5, 10, 20 µL/min). Signal intensity from muscle MBV (B) and femoral vessels (C) paralleled the doubling of the microbubble concentration in the circulation. (D) Correcting muscle MBV for the femoral vessels signal removes the variability in signal intensity caused by different microbubble concentrations (N = 9; error-bars represent standard deviation). Please click here to view a larger version of this figure.
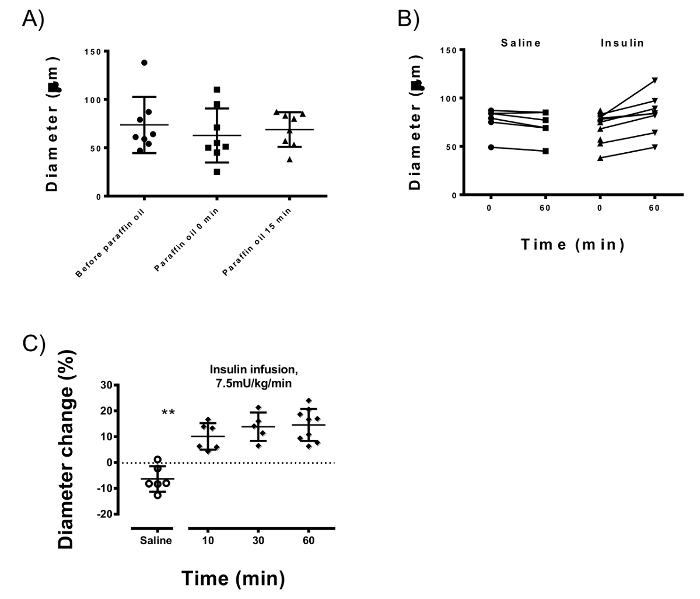
Figure 4: Intravital Microscopy Measurements of the Gracilis Artery. (A) Paraffin oil reduces the variation of the gracilis arteries of different animals (which is 29.0 µm without paraffin vs 17.9 µm after applying the oil) while keeping the average baseline diameter stable (73.6 µm vs. 68.8 µm; p = 0.58). (B) Arterial diameters at baseline and after 60 min of insulin or saline infusions. Insulin after 60 min infusion consistently dilated the gracilis artery (p <0.0001) when compared to saline infusion. (C) Insulin-induced vasodilation occurs at 10 min after the start of infusion (p = 0.002) and reaches 95% of the maximum at 30 min. Error-bars represent standard deviation; unpaired Student's T-test is used for statistics. Please click here to view a larger version of this figure.
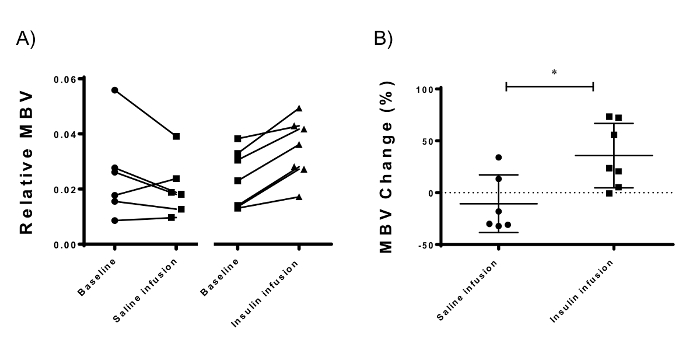
Figure 5: Microvascular Blood Volume Measurements using Contrast-enhanced Ultrasonography of the Adductor Muscle Compartment of the Mouse Hindlimb. (A) Insulin resulted in a consistent increase in MBV 30 min after the start of insulin infusion. (B) The difference between the hyperinsulinemic and the baseline measurements (MBV change) is denoted as the insulin-mediated microvascular recruitment. Insulin induced a 33.5% (± 31.04%, p = 0.016; N = 7) microvascular recruitment compared to saline infusion (-10.63 ± 27.87%, N = 6). Error-bars represent standard deviation; unpaired Student's T-test is used for statistics. Please click here to view a larger version of this figure.
