Long-term reduction in tremor in the treated extremity is on average 50% at 3 months and 40% at 12 months. Treatment success can be immediately evaluated after sonication through radiologic findings of a lesion at the Vim (Figure 1) and performance on clinical measures such as the hand-drawn spiral test (Figure 2). Additionally, intraoperative MR thermography provides real-time feedback to the target temperature. A permanent lesion is expected when the temperature reaches 55 – 60 °C.
A patient should be assessed for adverse events radiologically and clinically. MRI should reveal any edema, hemorrhage, and mal-placement of the lesion. While edema is usually seen with the lesion, it is typically asymptomatic for the patient and does not warrant any clinical intervention. The pin sites should be examined for infection and scalp for any post-treatment lesions. Soft tissue infection at the pin sites (e.g., redness, tenderness, and swelling) can be treated with a short course of oral antibiotics. If a careful neurological exam reveals any new neurologic deficits, such as weakness, sensory problems, and ataxia, the patient should be assessed and treated by the appropriate physician.
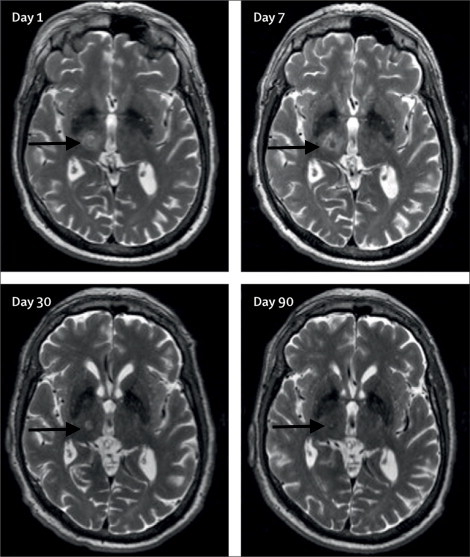
Figure 1: Axial T2-weighted 3T-MRI. Images of the right unilateral thalamotomy for a patient with medically-refractory essential tremor at days 1, 7, 30, and 90 after treatment. Black arrows are pointing to the Vim. This figure has been modified from reference6.
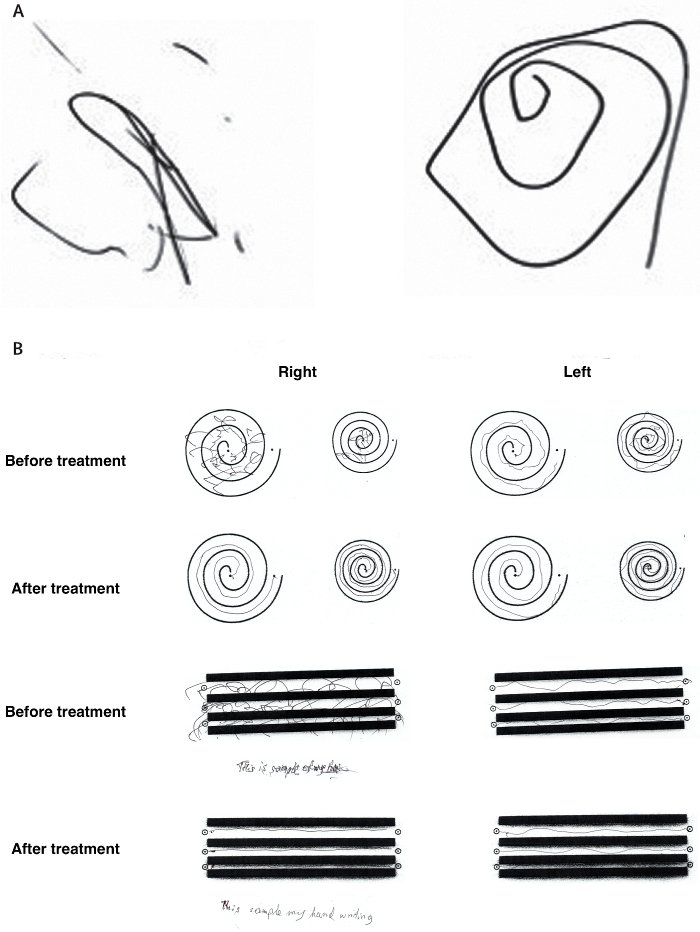
Figure 2: Representative clinical improvement on spiral drawing test. (A) The Archimedean spiral is a clinical tool used to measure severity of essential tremor. The spiral also provides information about the tremor orientation axis. Freehand spiral drawings of a patient immediately before (left) and immediately after (right) thalamotomy demonstrate dramatic improvement. (B) During the clinical rating scale for tremor (CRST), the patient is asked to complete several line drawings. The drawings of the patient before treatment and 3 months after treatment again demonstrate significant improvement. This figure has been modified from reference6. Please click here to view a larger version of this figure.
| Alertness and orientation | |
| Cranial nerves | Cranial nerves II to XII |
| Sensory exam | Pain |
| Position | |
| Vibration | |
| Light touch | |
| Motor exam | Strength |
| Tone | |
| Reflexes | Deep tendon reflexes |
| Pathological reflexes | |
| Coordination and balance | Finger to nose testing |
| Heel to shin testing | |
| Rapid alternating movements | |
| Heel-to-toe walking | |
| Romberg’s test |
Table 1: Checklist for a full neurological exam.
