The guillotine previously used in our laboratory was developed in 2004 and was based on models published by Einhorn21. The design did not permit adjustments to adequately account for any differences in bone morphology and did not permit a reproducible positioning of the limb. Furthermore, the previous apparatus required two people to operate it. Therefore, we designed, engineered, and built a new fracture apparatus. The main design goal was the possibility to the high-fidelity adjustment of the fracture depth, impact force, three-point contact, and animal positioning. The design is based on a fracture apparatus described by Marturano in 200822. A limiting factor of their design was the link between the fracture depth and the impact speed. The impact speed could not be adjusted without changing the fracture depth and the animal positioning. This made it impossible to change just one variable at a time when optimizing the fracture parameters. Additionally, it did not provide a way to easily adjust the location of a fracture in a long bone. Modifying how the depth of the fracture and the ram speed is adjusted, the design presented here permits a high-resolution, independent adjustment of all fracture variables. Additionally, the apparatus can be operated by a single user, it is cost-effective, and it allows adjustable animal positioning for generating location-specific fractures.
An optimization of tibia fractures in 17-week-old C57BL/6J male mice was performed using five specimens. The goal was to generate simple transverse fractures just below the level of the insertion of the fibula into the tibia. The distal tibia site is a common site of human bone fracture that results in non-union and, additionally, provides a homogeneous region of the tibia and avoids complications in the analysis associated with fibula damage. Mice were euthanized and radiographed. The mean FL from the calcaneal-tibial joint to the distal portion of the insertion of the fibula into the tibia was 0.556 ± 0.025 cm. Using an anvil width of 0.4 cm, the CGI was 0.2 cm, from which a JD of 0.356 cm was calculated. A positioning jig was constructed using computer-aided design software and printed at a resolution of 0.01 mm in acrylonitrile butadiene styrene (ABS) using a 3D printer (Figure 3B). Using one trial tibia, the jig design and the location of the fracture was confirmed by radiograph (Figure 1B).
For the results presented herein, the PL was calculated to be 1.579 cm, based on 90% of the mean tibial length (1.754 ± 0.031 cm). The mean medullary diameter (MD) was 0.05 cm. A needle size of 27 G x 3.175 cm was selected to exceed the necessary PL and fill the intramedullary canal (27 G = 0.041 cm). A cutting gauge was constructed with a length of 1.596 cm to demarcate the level of pin cutting (Figure 3B). Each of the remaining nine tibiae was then pinned. The mean cortical diameter was 0.098 cm, which was used to calculate an impact depth (ID) of 0.073 cm.
The initial tibia was impacted at a drop height of 1 cm, which resulted in no fracture. The drop height was increased by 1 cm to 2 cm. The new height resulted in a simple transverse fracture. For the subsequent fracture, the drop height was increased by 10% to 2.2 cm. This produced a simple transverse fracture on the first drop. All the remaining tibia fractured at 2.2 cm. In total, 9/9 (100%) of the pinned and fractured tibia resulted in simple transverse fractures without pin bending. The percentage of the experimental pin length to the target pin length and the experimental fracture length to the target fracture length were 101.1% and 97.6%, respectively. The final parameters are reported in Table 1, which also includes representative femur data.
Using the optimized parameters developed above, a trial was undertaken to compare pre- and post-optimization fractures. Retrospective radiographs were obtained from previous tibia fractures that were generated in our lab using a simple guillotine21 without optimization. Briefly, the tibiae were pinned using a 0.029-cm wire. The wire was inserted until resistance was felt, retracted 3 mm, cut, and driven into place. Subsequently, the mouse was placed under the guillotine with the point of impact approximately at the insertion of the fibula into the tibia. The guillotine was then dropped from a level of 10 cm. An additional dataset of fractures was collected which were generated using the adjustable guillotine and parameters derived from the optimization protocol (Table 1). Each group contained 58 fractures in 14-week-old, genotype-matched mice. The radiographs were analyzed for experimental fracture length (EFL): the distance from the calcaneal-tibial joint to the fracture, the experimental pin length (EPL), the bone length, and the fracture pattern.
Using an adjustable fracture device and optimized parameters significantly (p < 0.001) improved the generation of simple transverse fractures (Figure 5). The pre-optimization group only generated a simple transverse fracture 46.55% (27/58) of the time, compared to the post-optimization group which generated a simple transverse fracture 98.28% (57/58) of the time. Only one specimen in the post-optimization group had a complex fracture due to a malalignment in the positioning jig. Based on the methods described in the optimization protocol, the cut pin length should capture 90% of the total bone length. Using the optimization parameters and the pin cutting gauge, the percentage of the experimental pin length to bone length in the post-optimization group was 92.43% compared to only 83.67% in the pre-optimization group (p < 0.001). The optimization also significantly decreased the variability of the fracture locations, the pin length, and the pin-to-bone length percentage (p < 0.001). The results are reported in Table 2.
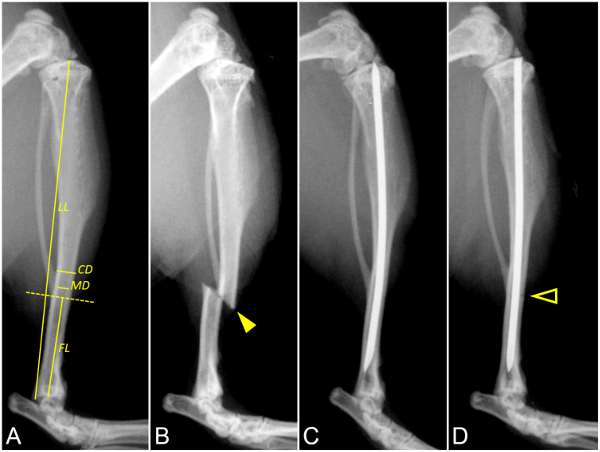
Figure 1: The optimization and generation of a simple tibia fracture. These panels show lateral radiographs of a murine tibia. (A) This panel shows the pre-fracture measurements. The dashed yellow line marks the ideal fracture location. The measurement overlays for the fracture length (FL), limb length (LL), medullary diameter (MD), and cortical diameter (CD) are indicated in the radiograph. (B) This panel shows a fracture location test. The solid arrowhead indicates the level of fracture in a non-stabilized tibia to test the positioning jig parameters. (C) This panel shows a pin length test with a pre-fracture radiograph to test the pin length (PL) and cutting gauge. PL should be 90% of LL, fill the intramedullary canal, and not protrude proximally or distally. (D) This panel shows a post-optimization fracture generation. The arrowhead outline indicates the level of the simple transverse tibia fracture. The pin is not bent at the level of impact. Please click here to view a larger version of this figure.
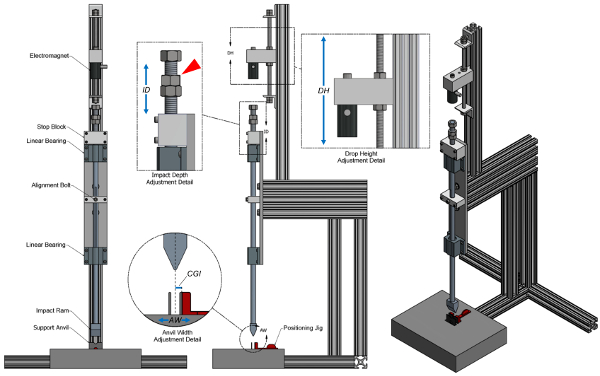
Figure 2: Adjustable fracture device design. This figure shows frontal, lateral, and perspective views of the fracture device. The frontal view includes annotations of major device components. The lateral view includes magnified details illustrating the adjustments for the impact depth (ID), the drop height (DH), and the anvil width (AW). Additional weight can be added to the ram by threading on weights at the top of the impact ram indicated by the red arrowhead. The dotted line in the Anvil Width Adjustment Detail indicates the line of impact. The center of guillotine impact to the outside surface a support anvil (CGI) is used to calculate the depth of the positioning jig to produce an accurate and precise fracture level. The positioning jig is shown in detail in Figure 3A. Please click here to view a larger version of this figure.
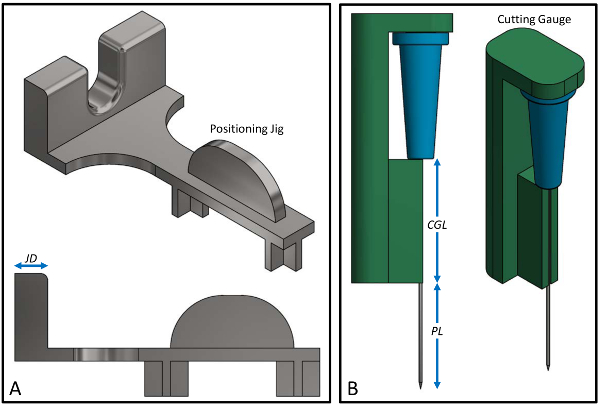
Figure 3: Positioning jig and cutting gauge design. (A) This panel shows details of the mouse positioning jig. The jig depth (JD) can be adjusted to change the fracture location on the limb. Increasing JD will move the fracture proximally and decreasing JD will move the fracture distally. (B) This panel shows details of the needle and the pin cutting gauge. The pin length (PL) should be 90% of the limb length (LL) (Figure 1A). The cutting gauge length (CGL) is derived from subtracting the PL from the needle length. In this example, a cutting gauge has been constructed (CGL = 1.6 cm) to demarcate a 27-G needle (length = 3.175 cm), leaving a PL of 1.58 cm after cutting. Please click here to view a larger version of this figure.
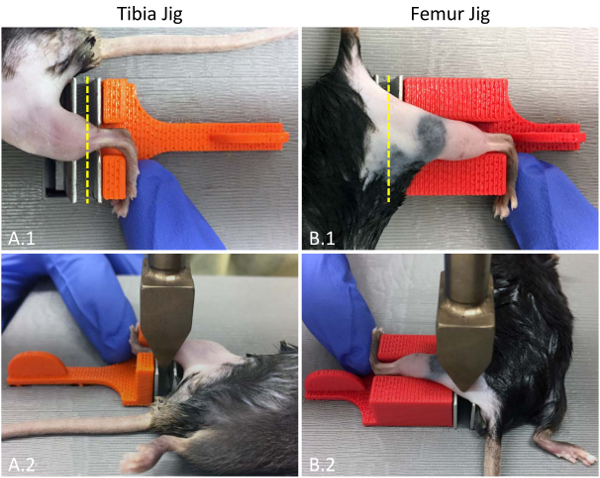
Figure 4: Tibia- and femur-fracture positioning. These are top-down photographs of (A) a mouse tibiaand (B) femur in the positing jig. (A.1) For tibia fractures, the mouse is placed in a supine position with the tibia in the center of the support anvils and the dorsum of the foot pressed against the jig. (B.1) For femur fractures, the mouse is placed in a prone position with the dorsum of the foot pressed against the jig. The dashed yellow line indicates the location of the anvil impact. (A.2 and B.2) The bottom photographs demonstrate the anvil location at the time of impact. The positioning of the researcher's hands should not interfere with the ram actuation. Please click here to view a larger version of this figure.
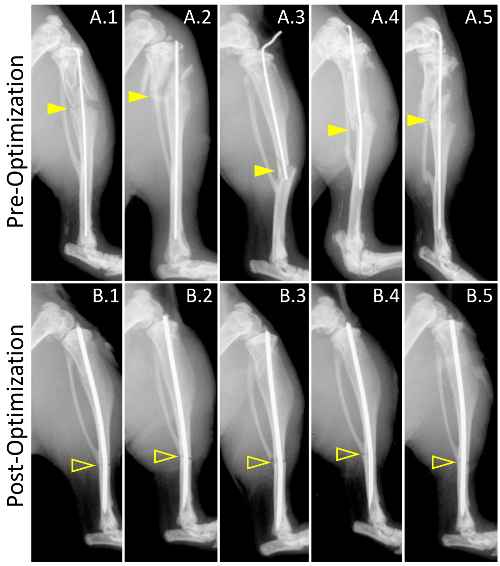
Figure 5. Pre- and post-optimization of the fracture generation. These panels show lateral radiographs of representative fractures from (A) pre-optimization and (B) post-optimization fracture groups. The size of the group was 58 mice. Solid arrowheads and arrowhead outlines indicate the level of fracture in the pre- and post-optimization groups, respectively. (A.1 – A.5) The fractures generated pre-optimization demonstrate a high degree of comminution and fracture-level variability. The pin diameter only partially fills the intramedullary canal with a high degree of length variability. The pin length inconsistency resulted in (A.3) non-stabilized fractures and (A.3 – A.5) pin exposure. A lack of fracture depth control resulted in (A.4) bent pins and contributed to (A.1 – A.5) comminution. In fractures generated post-optimization (see Table 1 for the full set of parameters), the use of a positioning jig (Figure 3A) resulted in a low variability of fracture locations (yellow arrowhead outlines). The optimization of the pin width based on pre-fracture radiographs resulted in a pin selection that filled the intramedullary canal. The use of a pin cutting gauge (Figure 3B) resulted in a consistent pin length. The optimization of the drop height and the impact depth produced simple transverse fractures with no comminution or bent pins. Please click here to view a larger version of this figure.
| Abbreviation | Tibia | Femur | ||
| Pre-fracture parameters | ||||
| Anvil Width (cm) | AW | 0.40 | 0.40 | |
| Ram Weight (g) | RW | 272.00 | 272.00 | |
| Pre-fracture measurements | ||||
| Limb Length (cm), mean±SD | LL | 1.75±0.03 | 1.32±0.05 | |
| Cortical Diameter (cm), mean±SD | CD | 0.10±0.00 | 0.15±0.01 | |
| Medullary Diameter (cm), mean±SD | MD | 0.05±0.00 | 0.09±0.01 | |
| Pin Size (gauge/cm) | PS | 27/3.175 | 23/3.810 | |
| Center of Guillotine Impact (cm) = AW / 2 | CGI | 0.20 | 0.2 | |
| Fracture Length (cm), mean±SD | FL | 0.56±0.02 | 0.64±0.01 | |
| Optimization | ||||
| Pin Length (cm) = 0.9 * LL | PL | 1.58 | 1.19 | |
| Impact Depth (cm) = 0.75 * CD | ID | 0.07 | 0.11 | |
| Cutting Gauge Length (cm) = PS – PL | CGL | 1.60 | 2.62 | |
| Jig Depth (cm) = FL – CGI | JD | 0.36 | 0.44 | |
| Drop Height (cm) | DH | 2.20 | 4.40 | |
| Post-fracture measurements | ||||
| Experimental Pin Length (cm), mean±SD | EPL | 1.60±0.06 | 1.19±0.04 | |
| Experimental Pin Length to Pin Length (%) | 101.1% | 100.0% | ||
| Experimental Fracture Length (cm), mean±SD | EFL | 0.54±0.01 | 0.62±0.06 | |
| Experimental Fracture Length to Fracture Length (%) | 97.6% | 97.1% | ||
| Simple Transverse Fracture (%) | 9/9 (100%) | 9/9 (100%) | ||
Table 1: Parameters of the fracture generation before and after the development of the new guillotine system.
| Pre-Optimization | Post-Optimization | Test | Significance | |
| Experimental Fracture Length (cm), mean±SD | 0.74±0.28 | 0.52±0.05 | t | <0.001 |
| F | <0.001 | |||
| Experimental Pin Length (cm), mean±SD | 1.47±0.21 | 1.57±0.09 | t | <0.001 |
| F | <0.001 | |||
| Pin to Bone Length (%), mean±SD | 83.67±11.97 | 92.43±5.29 | t | <0.001 |
| F | <0.001 | |||
| Simple Transverse Fracture (%) | 46.55 | 98.28 | Pearson | <0.001 |
Table 2: Fracture results before and after the parameter optimization.
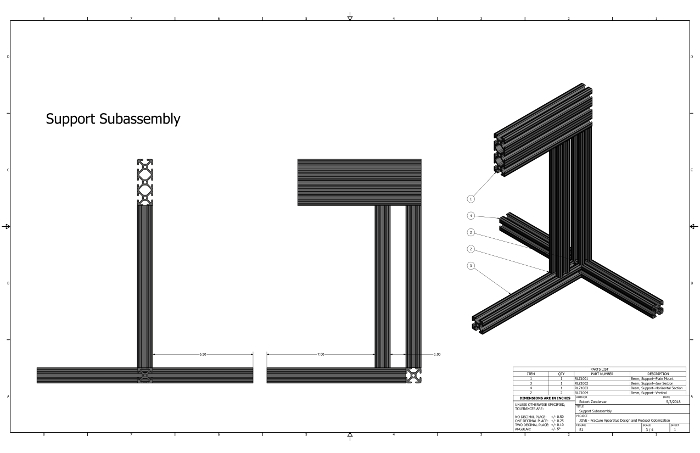
Supplementary Figure 1: Support Subassembly technical drawing. This figure shows a technical drawing for the assembly of the support components. Please click here to view a larger version of this figure.
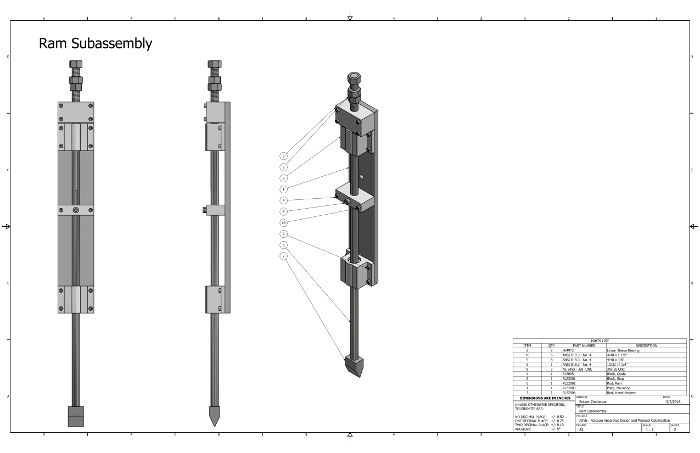
Supplementary Figure 2: Ram Subassembly technical drawing. This figure shows a technical drawing for the assembly of the ram components. Please click here to view a larger version of this figure.
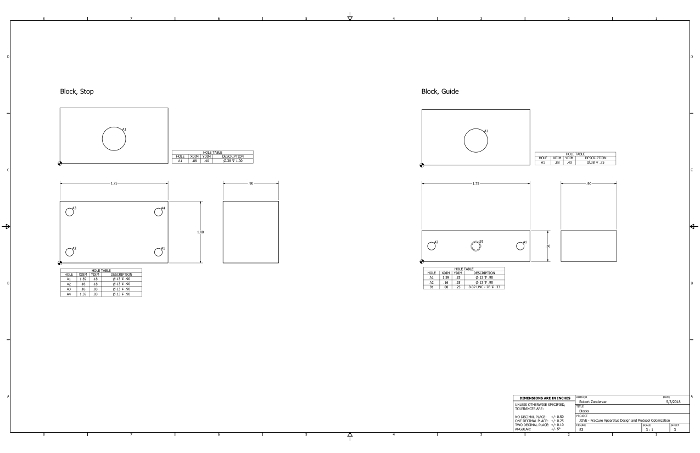
Supplementary Figure 3: Blocks technical drawing. This figure shows a technical drawing which can be used to manufacture the stop and guide blocks for the fracture apparatus. We used aluminum. Please click here to view a larger version of this figure.
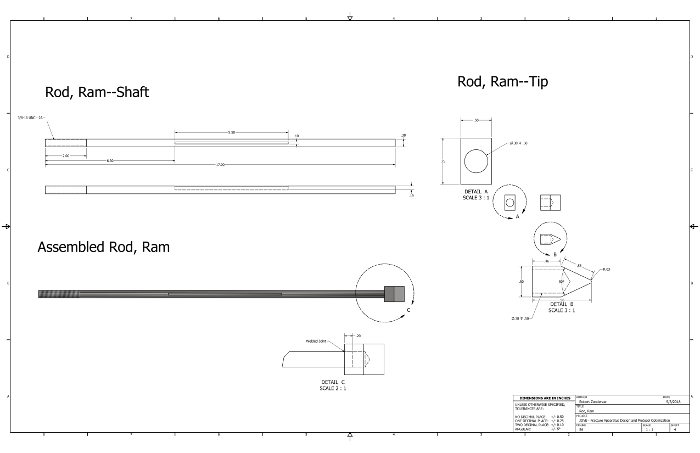
Supplementary Figure 4: Rod, Ram technical drawing. This figure shows a technical drawing which can be used to manufacture the ram for the fracture apparatus. We used stainless steel. Please click here to view a larger version of this figure.
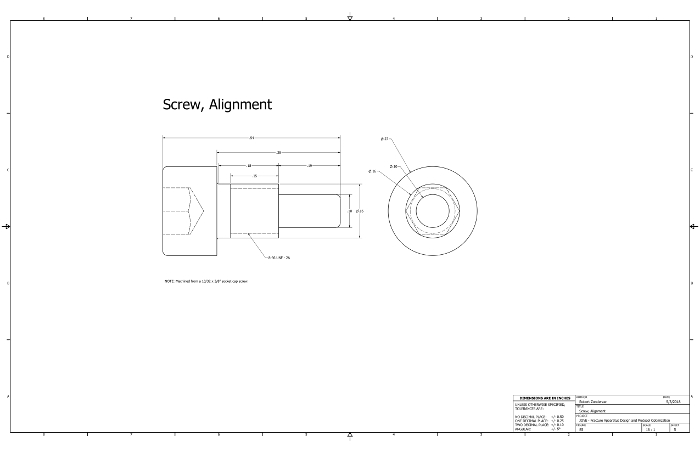
Supplementary Figure 5: Screw, Alignment technical drawing. This figure shows a technical drawing which can be used to modify a socket cap screw to align the ram. Please click here to view a larger version of this figure.
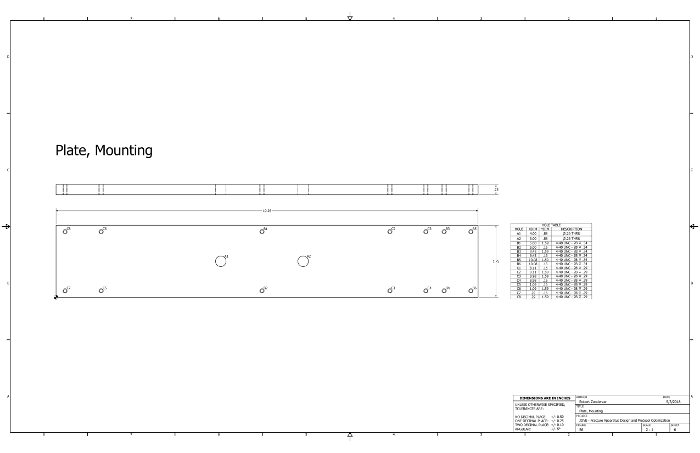
Supplementary Figure 6: Pate, Mounting technical drawing. This figure shows a technical drawing to manufacture the mounting plate for the fracture apparatus. We used aluminum. Please click here to view a larger version of this figure.
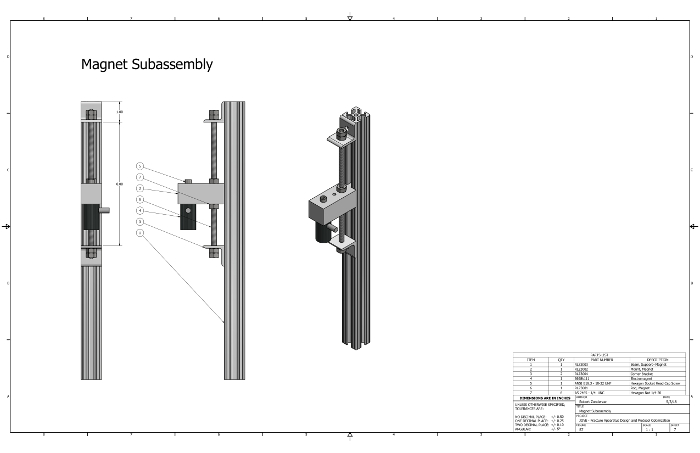
Supplementary Figure 7: Magnet Subassembly technical drawing. This figure shows a technical drawing for the assembly of the magnet components. Please click here to view a larger version of this figure.
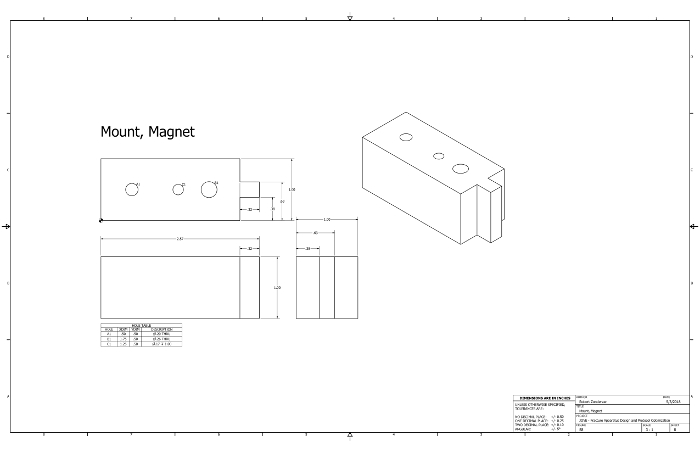
Supplementary Figure 8: Mount, Magnet technical drawing and CAD file. This figure shows (A) a technical drawing and (B) CAD file which can be used to manufacture the magnet mount (file format: *.stl). We 3D-printed the part using polylactic acid (PLA). Please click here to view a larger version of this figure.
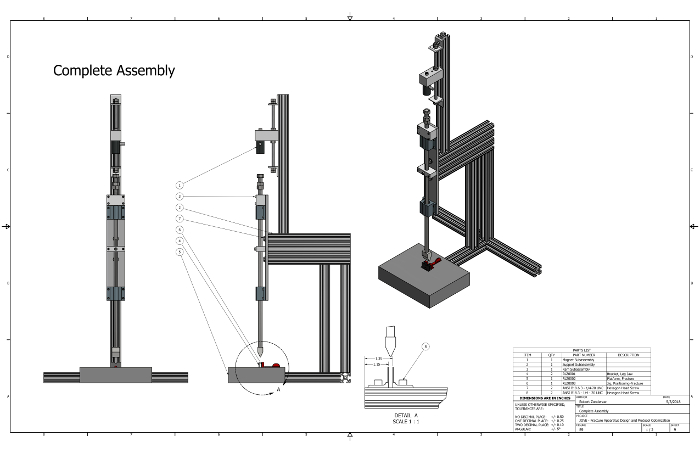
Supplementary Figure 9: Complete Assembly technical drawing and CAD file. This figure shows (A) a technical drawing of the complete fracture assembly with its components and (B) the CAD file (file format: *.iam). Please click here to view a larger version of this figure.
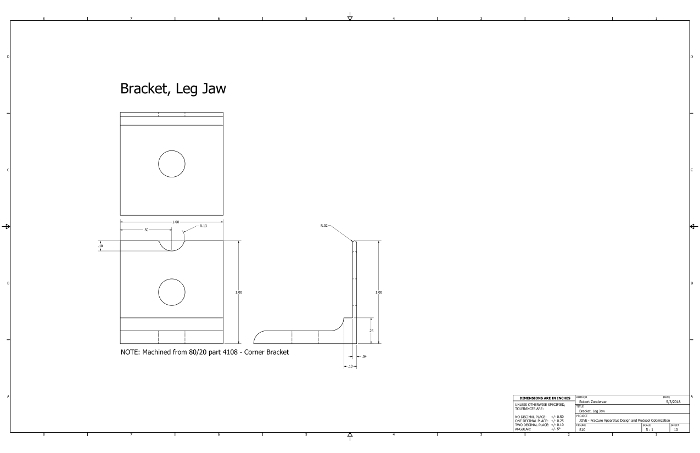
Supplementary Figure 10: Bracket, Leg Jaw technical drawing. This figure shows a technical drawing which can be used to manufacture the leg brackets for the fracture apparatus. The brackets are machined from off-the-shelf 8020 corner brackets. Please click here to view a larger version of this figure.
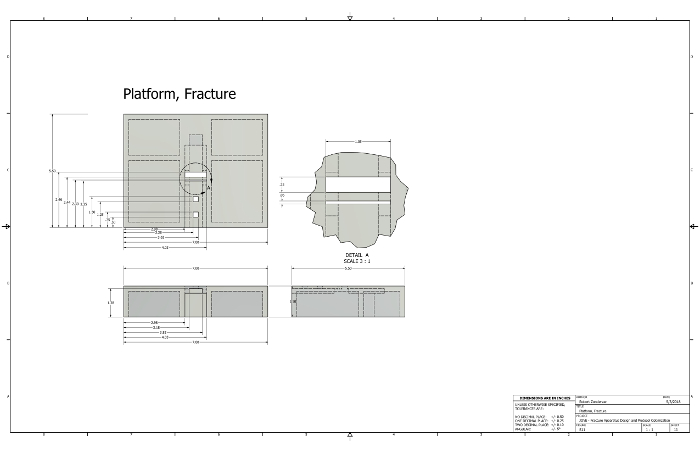
Supplementary Figure 11: Platform, Fracture technical drawing and CAD file. This figure shows (A) a technical drawing and (B) CAD file which can be used to manufacture the fracture platform (file format: *.stl). We 3D-printed the part using polylactic acid (PLA). Please click here to view a larger version of this figure.
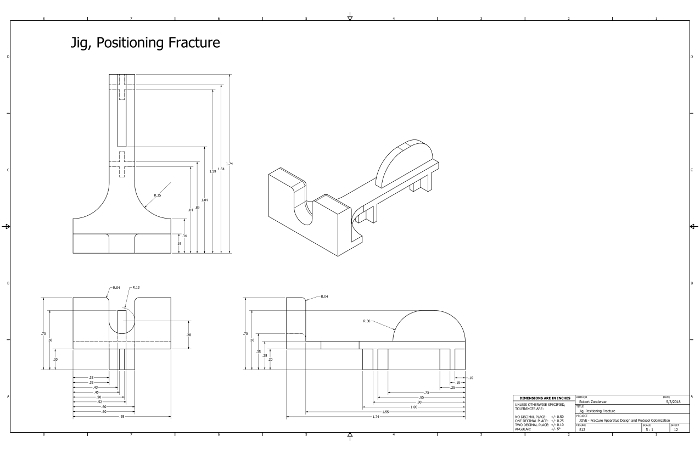
Supplementary Figure 12: Jig, Positioning Fracture technical drawing and CAD file. This figure shows (A) a technical drawing and (B) CAD file which can be used to manufacture the limb-positioning jig (file format: *.stl). We 3D-printed the part using polylactic acid (PLA). Please click here to view a larger version of this figure.
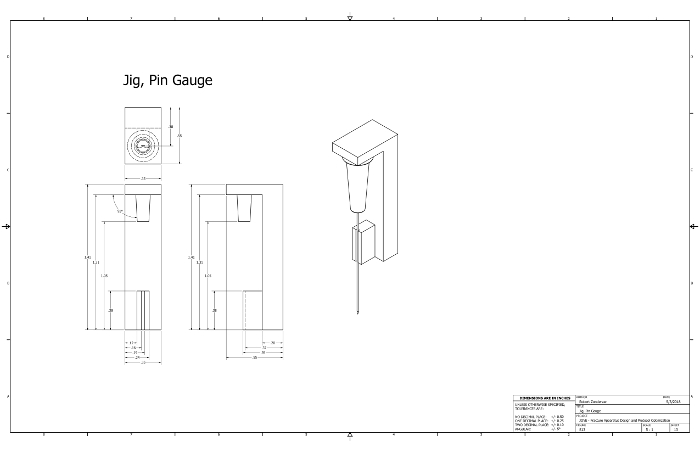
Supplementary Figure 13: Jig, Pin Gauge technical drawing and CAD file. This figure shows (A) a technical drawing and (B) CAD file which can be used to manufacture a pin cutting gauge (file format: *.stl). We 3D-printed the part using polylactic acid (PLA). Please click here to view a larger version of this figure.
