A total of 24 adult male C57BL/6 mice, weighing between 24–31 g at the time of surgery, were used in the study. One animal died following middle cerebral artery occlusion (MCAO) and one was excluded due to surgical complications. The data presented here are taken from a previously published work by the authors. These were used to illustrate the effect of vessel repair on MCAO outcomes11. All data are expressed as thr mean ± standard deviation. The data were statistically assessed for normality using the D'Agostino-Pearson omnibus normality test. Parametric data were compared using Student's t-test (for two means) and one-way ANOVA with the Sidak test (multiple means). Non-parametric data were compared using the Mann-Whitney U test. The variability of the parametric data was assessed using an F-test, and non-parametric data variability was assessed using Levene's test.
Typically, in MCAO procedures, the occluding filament is inserted into the CCA and the ECA is ligated to prevent this filament from passing into the ECA rather than the ICA. An avoidance of ECA ligation and the addition of analgesia showed a trend toward reduced weight loss at 48 h post-MCAO, when compared to data from previous studies undertaken by the same surgeon for the same MCAO time using ECA ligation with no analgesia, whereas the LV appeared unaffected, see Figure 1.
Mice underwent a 60 min MCAO-induced ischemia followed by reperfusion with CCA vessel repair or with the typical ligation of the CCA approach. A schematic of the ligated and unligated repaired CCA is shown in Figure 2.
Laser Doppler flowmetry was used to confirm the blood flow perfusion in the territory of the MCA at MCAO, before and after the CCA vessel repair. Figure 3 demonstrates that 5 min following the filament removal, the regional cerebral blood flow (rCBF) significantly increased in the brain region of the MCA. The perfusion was maintained up to the vessel repair, with an increase in the perfusion to the MCA territory shown following the CCA vessel repair, suggesting that the CCA repair allowed an increased blood perfusion to the ischemic territory compared to reliance on the Circle of Willis alone.
T2-weighted MRI was used to determine the total LV, and DTI scans were used to determine the core LV, 48 h after the MCAO. Figure 4A shows no significant difference in the total or core LV between the repair and ligated procedure groups. However, the data variability for both total and core LV, as assessed using Lavene's test for non-parametric or the F-test for parametric data, was significantly reduced within the CCA repair group. The total LV was broken down into cortical and subcortical LV, as shown in Figure 4B. The cortical portion was significantly less variable in the CCA repair group, whereas the sub-cortical portion of the lesion was unaffected between the two procedural groups.
A power analysis indicated that fewer animals per treatment group would be required to demonstrate a 30% reduction in the LV following MCAO using CCA repair versus the typical CCA-ligated procedure, see Table 1. An assumption of power 1-β= 0.8 and significance level α = 0.05 and a prediction of 30% reduction in the LV between the hypothetical control and test groups were used for the power analysis. Furthermore, an equal variance was assumed between the groups. Table 1 shows the number of animals required for the test and control groups when either the typical CCA-ligated method is used or the updated CCA repair method, as described here, is used. Note that the test group refers to a hypothetical treated group of animals and the control group refers to a hypothetical control group; both groups would undergo MCAO.
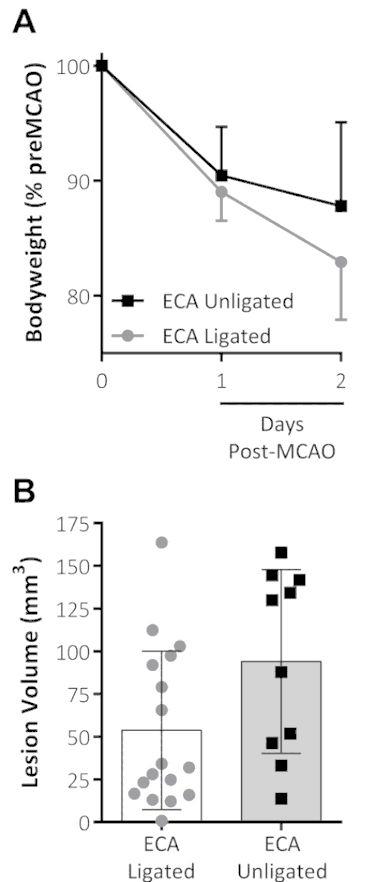
Figure 1: Combined analgesia treatment and the omission of ECA ligation on outcomes following MCAO. (A) Body weight, shown as a percentage of pre-MCAO weight, decreased the first 2 d following the MCAO for both groups. The ECA-unligated group (analgesia-treated with no ECA ligation at MCAO) showed a trend toward reduced weight loss on the second day following the MCAO. (B) This panel shows the lesion volume (mm3) measured by standard triphenyltetrazolium chloride (TTC) staining 48 h after the MCAO. The data shown are the mean ± standard deviation. ECA ligated: n = 17, ECA unligated: n = 10. This figure has been modified from Trotman-Lucas et al.11. Please click here to view a larger version of this figure.
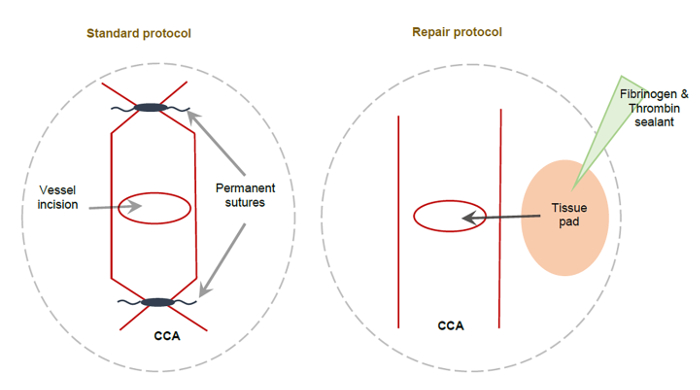
Figure 2: Schematic showing the standard CCA method and the alternative CCA repair method following MCAO. (A) This schematic depicts a permanently ligated CCA using non-dissolvable sutures applied to either side of the CCA incision, resulting in the permanent ligation of the right CCA. (B) This schematic depicts the alternative CCA repair method. A small tissue pad coated with fibrinogen and thrombin sealant is used to cover the CCA incision, sealing it to allow the full perfusion of the right CCA. This figure has been modified from Trotman-Lucas et al.11. Please click here to view a larger version of this figure.
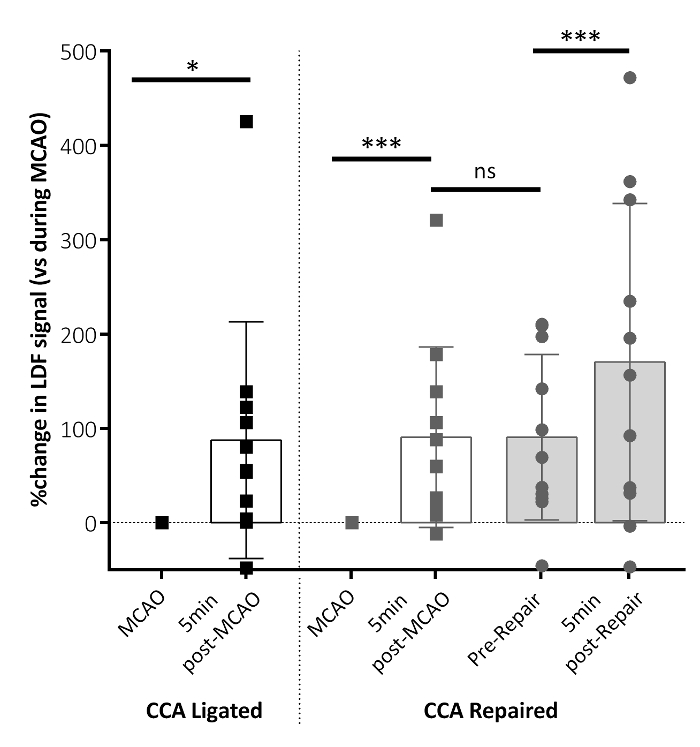
Figure 3: Regional cerebral blood flow (rCBF) parameters following MCAO. The rCBF changed 5 min after the MCAO filament removal for both the CCA-ligated and CCA-repaired groups (post-MCAO), relative to the rCBF measured during MCAO. This panel shows the rCBF data immediately before the CCA vessel repair (pre-repair) and 5 min following the CCA repair (post-repair). Significant increases in the rCBF are shown 5 min after the filament removal (post-MCAO) in both groups. An additional increase in the rCBF is shown following the CCA repair (post-repair) in the CCA repair group. No difference in the rCBF is shown between 5 min post-MCAO and pre-repair. The data shown are condensed from the analyzed time-course data reporting key time points, here as the mean ± standard deviation. CCA ligated: n = 10, CCA repaired: n = 10; **P < 0.01, ***P < 0.001, ns: non-significant. This figure has been modified from Trotman-Lucas et al.11. Please click here to view a larger version of this figure.
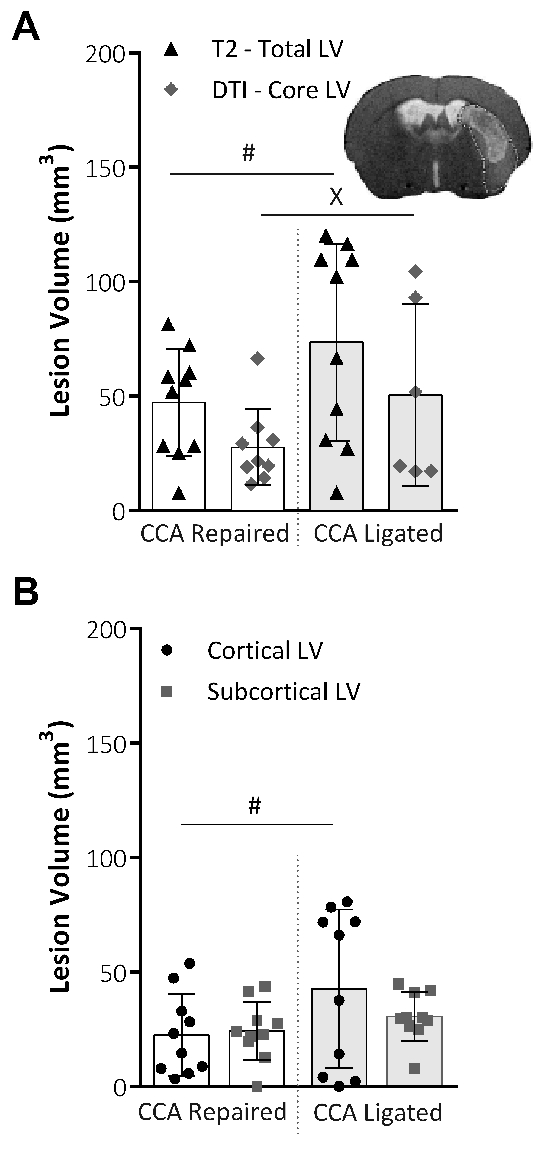
Figure 4: Analysis of the lesion volume obtained by MRI techniques. (A) This panel shows the lesion volume (LV; mm3) at 48 h following MCAO, the total LV taken from T2-weighted MRI images (Total LV), and the core LV taken from DTI scans and analysis (Core LV). Representative images show the total lesion volume from a T2 scan slice image with the DTI core lesion volume mask applied. The variability within the groups was significantly reduced for both the total LV (P = 0.015, CCA repair: n = 10, CCA ligated: n = 10, F-test) and the core LV (P = 0.043, CCA repair: n = 9, CCA ligated: n = 6, Lavene's test), assessed using an F-test for parametric data or Levene's test for non-parametric data. (B) This panel shows the LV at 48 h following MCAO, taken from T2-weighted MRI images and divided into cortical and subcortical lesion areas. The CCA repair significantly reduced the data variability (P = 0.03, F-test) in the cortical portion of the lesion, but no effect on the data variability in the subcortical portion of the lesion was shown. CCA repair: n = 10, CCA ligated: n = 10. The data shown are the mean ± standard deviation. #P < 0.05 (F-test), xP < 0.05 (Lavene's test). This figure has been modified from Trotman-Lucas et al.11. Please click here to view a larger version of this figure.
| Approach | Lesion Volume (LV; mm3; mean ± s.d.) |
Power | Significance Level | Anticiapted difference | Group size required |
| CCA Ligated (traditional approach) | 94.08 ± 53.79 | 0.8 | 0.05 | 30% | n = 58 |
| CCA Repaired (new approach) | 51.73 ± 22.78 | 0.8 | 0.05 | 30% | n = 35 |
Table 1: Representative power analysis comparing traditional CCA ligation with the alternative CCA repair method explained here. This table shows the power analysis conducted to calculate the anticipated group size required to detect a significant difference in the LV between a control group, the traditional or alternative (new) approach, and a test group (predicted). The table shows the group sizes as required if a power of 0.8 is assumed, a significance level of 0.05 is applied, and if the predicted test group shows a 30% difference in the LV compared to the control group. The table shows results for both MCAO approaches (the CCA-ligated and the CCA-repaired) to determine if there is a difference in the number of animals required to gain a 30% difference in the LV. For both methods, an equal variance is assumed between the test and the control group. This figure has been modified from Trotman-Lucas et al.11.
