Lung injury was induced by a single endotracheal injection of 1.5 U/kg body weight of bleomycin sulfate in 100 µL of sterile saline. Control animals received an endotracheal injection of an equal volume of saline. Two shots of hUC-MSC (2.5 x 105 in 200 µL of sterile saline) were infused into the mouse tail vein, 24 h and 7 days after the bleomycin administration. Control animals received an intravenous infusion of an equal volume of sterile saline. Mice were sacrificed for lung explant and tissue processing at days 8, 14, and 21 after the bleomycin administration (Figure 1).
We demonstrated that a direct instillation of bleomycin into the mouse trachea allowed a rapid diffusion down to the lungs, resulting in extensive inflammation, progressive fibrosis, and a distortion of their normal architecture, consistently with prior studies11. Lung histopathological changes were assessed by hematoxylin-eosin (H&E) and picrosirius red staining10, and fibrosis was confirmed by an increased hydroxyproline content and collagen deposition (Figure 2). Inflammatory changes in tissue were assessed by a histological scoring system based on the inflammatory infiltration around bronchioles, bronchi, and blood vessels, and interstitial pneumonia observed in hematoxylin-eosin stained lung sections10. Following the bleomycin injection, the Ashcroft score of lung sections progressively increased from a mean value of 1.5 at day 8 to a mean value of 4.5 at day 14 and of 6.5 at day 2110. The double infusion of hUC-MSC into the mouse tail vein largely attenuated bleomycin-induced lung injury, with significant reduction, although not complete abrogation, of both the inflammatory infiltration and the extent of fibrosis at each time point (Figure 2). Immunostaining with specific antibodies10 showed that infused hUC-MSC rapidly and effectively reached mouse lungs, although only a few cells were detected, with a decreasing number from day 8 to day 21 (Figure 3). As previously reported12, these data suggest a rapid dislocation of the cells from the site of injury, despite their prolonged protective effect. Immunohistochemistry (IHC) staining of hUC-MSC was performed, also in the saline-treated samples, but no cell could be detected, given the absence of inflammatory foci attracting hUC-MSC.
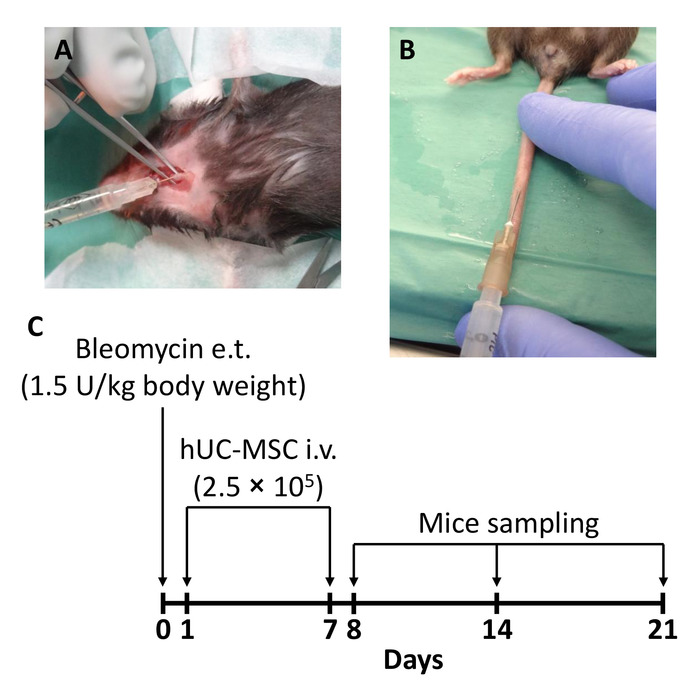
Figure 1: Schematic of the experimental protocol. (A) Mice received a single endotracheal (e.t.) injection of 1.5 U/kg body weight of bleomycin to induce lung injury (day 0). (B) A double intravenous (i.v.) infusion of 2.5 x 105 human mesenchymal stromal cells obtained from whole umbilical cord (hUC-MSC) was performed 24 h (day 1) and 7 days (day 7) after the bleomycin administration. (C) A timeline of the injections and moments of sacrifice is shown here. Mice groups were sacrificed at days 8, 14, and 21 after the bleomycin administration (i.e., 24 h, 7 days, and 14 days after the second hUC-MSC infusion, respectively). This figure has been modified from Moroncini et al.10. Please click here to view a larger version of this figure.
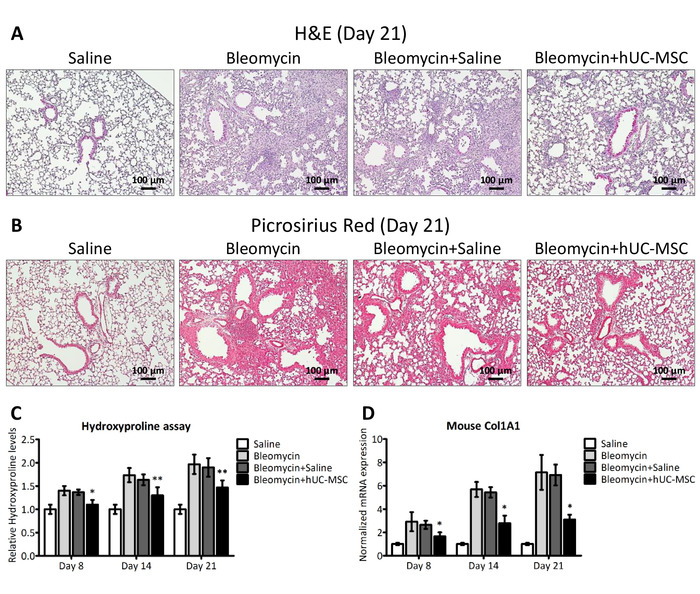
Figure 2: hUC-MSC downregulate bleomycin-induced lung inflammation and fibrosis. (A and B) Representative microscopic images (10x magnification) of hematoxylin-eosin (H&E) and picrosirius red staining of lung sections obtained from C57BL/6 mice, 21 days after the endotracheal injection of sterile saline (saline) or bleomycin (bleomycin), the latter also followed by an intravenous infusion of hUC-MSC (bleomycin+hUC-MSC) or sterile saline (bleomycin+saline). The saline controls demonstrated normal lung architecture. Widespread inflammatory infiltrates were observed 21 days after the bleomycin injury, with a severe distortion of the lung architecture and the formation of fibrotic foci. Bleomycin-induced alterations were significantly attenuated by the hUC-MSC treatment but not by saline. (C) Hydroxyproline content at days 8, 14, and 21 in the lungs of C57BL/6 mice that received the aforementioned treatments. The results are the mean ± SD (n = 8 per group), expressed as a percentage of the value obtained from endotracheal saline-treated mice and are representative of three independent experiments. *P < 0.05, **P < 0.01, compared to bleomycin-treated mice. (D) Mouse Col1A1 expression levels in whole lung mRNA obtained at days 8, 14, and 21 from C57BL/6 mice that received the aforementioned treatments. The results are the mean ± SD (n = 5 per group) and are representative of three independent experiments performed in triplicate. *P < 0.05, **P < 0.01, compared to bleomycin-treated mice. This figure has been modified from Moroncini et al.10. Please click here to view a larger version of this figure.
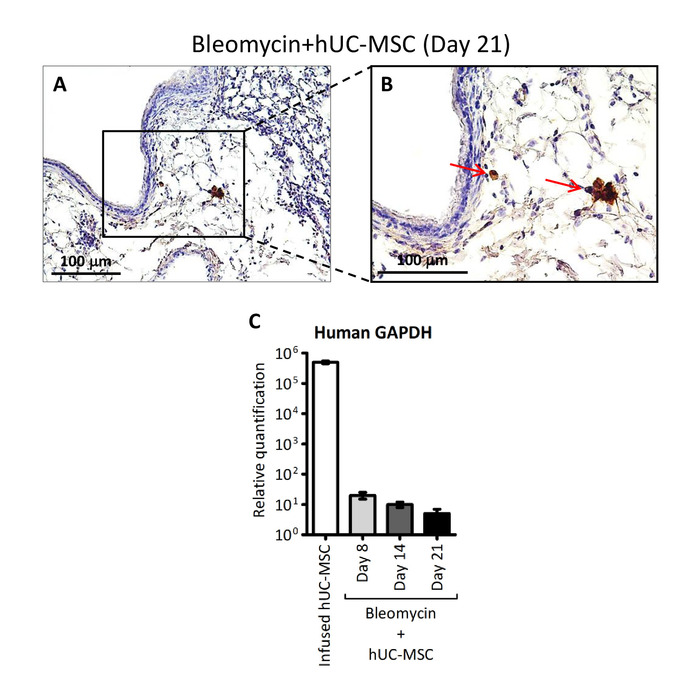
Figure 3: Detection of hUC-MSC in lung tissue. (A and B) Representative microscopic images (200x and 400x magnification, respectively) of immunostaining with anti-HLA-1 antibody of lung sections obtained from C57BL/6 mice receiving endotracheal bleomycin followed by intravenous hUC-MSC. The red arrows indicate positive-stained hUC-MSC. (C) Human GAPDH assessed by quantitative real-time polymerase chain reaction (PCR) assay in whole mRNA extracted from cultured hUC-MSC prior to infusion (infused hUC-MSC) or from lung tissue at days 8, 14, and 21 of C57BL/6 mice receiving endotracheal bleomycin followed by intravenous hUC-MSC (bleomycin+hUC-MSC). The results are the mean ± SD (n = 5 per group) and are representative of three independent experiments performed in triplicate. Of note, the source of human GAPDH transcript in this experimental protocol can be provided exclusively by the intravenously infused hUC-MSC. This figure has been modified from Moroncini et al.10. Please click here to view a larger version of this figure.
