Oxygen gradient ektacytometry can be used to characterize sickling behavior in patients with SCD. In this study, blood samples from a total of 38 SCD patients and five healthy controls were included. In healthy controls, the diffraction pattern is circular at rest and elliptical at higher shear stress4. From the elliptical diffraction pattern, the elongation index (EI) is calculated based on the height and width of the diffraction pattern. In oxygen gradient ektacytometry, slow and continuous deoxygenation of the sample by nitrogen gas is followed by swift reoxygenation by ambient air. Under these conditions, RBC sickling can be observed under deoxygenation. This will cause a distortion of the diffraction pattern because sickled red cells will not align properly under the applied shear stress. Hence, they appear to be less deformable as opposed to healthy RBCs (Figure 2).
Figure 3A shows how sickle RBCs change in shape upon deoxygenation, which mimicked conditions during oxygen gradient ektacytometry, whereas control sickle RBCs without deoxygenation show no change in shape. This process results in distortion of the diffraction pattern during oxygen gradient ektacytometry, and thus in a decrease in EI. Figure 3B shows the different diffraction patterns from which different parameters are generated.
A representative curve obtained by the ektacytometer is shown in Figure 3C. Six parameters reflect different characteristics of sickling behavior of RBCs: EImax is the maximum EI at the start of the measurement before deoxygenation. This parameter represents the baseline position and reflects the overall deformability of the total RBC population at ambient air. EImin is the minimum EI, which represents minimal deformability after deoxygenation. This parameter reflects changes in the shape and orientation of (sickle) RBCs upon deoxygenation. ΔEI is the difference between EImax and EImin, which indicates how many cells can sickle during one round of deoxygenation. 5% Point of Sickling (PoS5%) is the pO2 (mmHg) at which a 5% decrease of EImax during deoxygenation is measured. This represents the oxygen tension where the sickling process starts. Area reflects the area under the curve, which is determined by an integral calculation of EI and pO2 measurements between 100 mmHg and pO2min (mmHg). This is the result of previously described parameters EImax, EImin, and PoS. Recovery represents the difference of EI during the final part of reoxygenation compared to EI at baseline. Both EI values are measured at a pO2 of 100–120 mmHg. This parameter reflects the capacity of RBCs that sickle during deoxygenation to reverse sickling during reoxygenation22. Parameters from duplicate measurements generally had a coefficient of variation (CV) <5% (median 1.83%). In case a CV > 5% was obtained, a third measurement was performed. The parameters EImax and Recovery are the most reproducible with median CVs <1%.
Representative curves of RBCs of healthy controls, patients with HbS traits (heterozygous HbS), and a homozygous SCD patient are shown in Figure 4A. The representative curve of the HbSC patient shows a lower recovery, which might indicate a different sickling process (Figure 4B). The representative curves of HbSS patients treated with hydroxyurea (HU) and transfusion are shown in Figure 4C and Figure 4D. Clearly, there is a big difference between the representative curves of HS traits (HbAS cells) and RBCs of HbSS patients treated with transfusion (consisting of a mixture of homozygous sickle (HbSS) and homozygous normal (HbAA) cells, Figure 4A,D). The clear differences in the curves of the untreated SCD patient and the HU and transfusion-treated patients highlights the usefulness of this assay (Figure 4C,D). Levels of HbF and HbS correlated significantly with EImin and, to a lesser extent, with PoS (Figure 5A–D). This indicates that those laboratory parameters that are important in the evaluation of the patient are also reflected in the oxygen gradient ektacytometry. The number of sickled cells at normoxia and percentage of dense RBCs (DRBCs) both influence EImax values, as they are significantly correlated (Figure 5E–F), which indicates that EImax reflects another important factor in the sickling process. These results show how different characteristics such has %HbS, %HbF, sickled cells at normoxia, and %DRBCs influence different parameters.
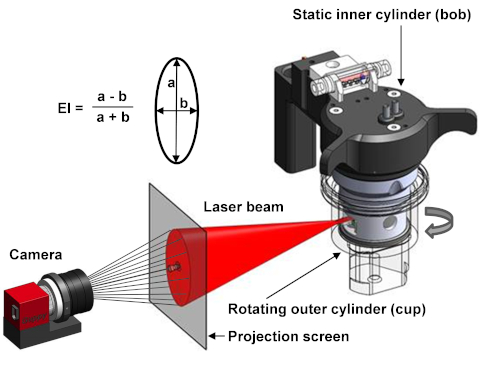
Figure 1. Schematic setup of the ektacytometer. The ektacytometer uses a Couette system to apply shear stress on the cells. A rotation outer cylinder (cup) and a static inner cylinder (bob) are used to induce shear stress by the creation of laminar flow at 37 ˚C. Between the bob and cup there is a small gap in which the blood suspension is injected. A laser beam shines from the bob through the blood suspension and is scattered by the presence of RBCs. The diffraction pattern is projected and analyzed by a camera. The elongation index (EI) is calculated with the height (a) and the width (b) of the diffraction pattern4. Please click here to view a larger version of this figure.
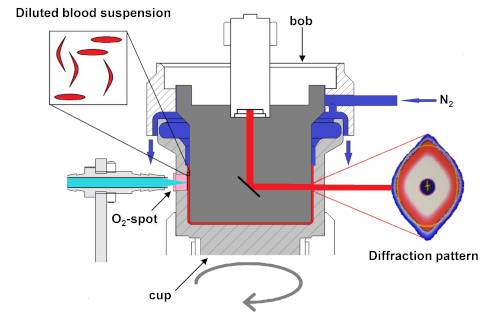
Figure 2. Schematic setup of the ektacytometer with oxygen gradient ektacytometry module. Schematic diagram of the module that shows deoxygenation of the blood suspension slowly with the infusion of nitrogen gas (N2). Oxygen tension is measured by the amount of quenching of the luminophore signal sent from the LED-fiber to the O2-spot. Upon deoxygenation, sickle RBCs will start to sickle, their deformability will decrease, and they will no longer align with elliptical RBCs. The sickled RBCs will distort the diffraction pattern, changing its shape from an ellipse to a rhomboid or diamond-like shape. This change in the shape of the diffraction pattern results in a decrease of EI. Measurements of pO2 and EI are not performed at the same height in the cup. This ensures better discrimination between the deoxygenation and reoxygenation curves and, hence, a better interpretation of the curve. This figure has been modified from Rab et al.22 Please click here to view a larger version of this figure.
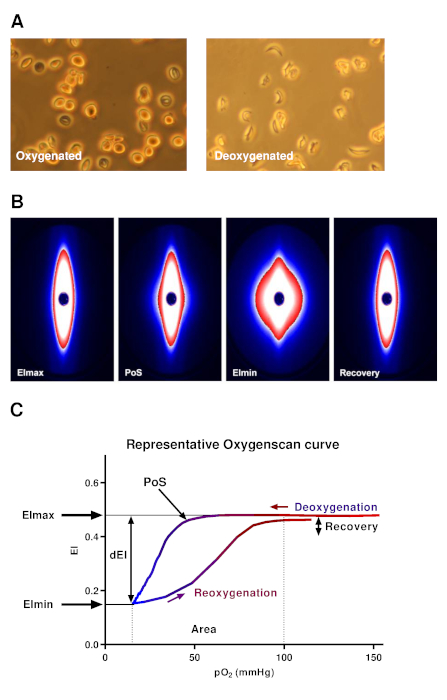
Figure 3. Representative oxygen gradient ektacytometry curve and diffraction patterns. (A) Upon deoxygenation under conditions similar to the oxygen gradient ektacytometry, sickle RBCs were fixed. In control sickle RBCs, the same conditions were used, but without nitrogen gas. Deoxygenated sickle RBCs show a change in shape in contrast to control RBCs. (B) Upon deoxygenation and shear stress (30 Pa), the diffraction pattern changes from an ellipse to a rhomboid. (C) Representative curve of oxygen gradient ektacytometry. The maximum elongation index (EImax) represents the baseline position and shows an overall deformability of the total RBC population. Minimum EI (EImin) represents minimal deformability, which is caused by the change in shape and orientation of RBCs upon deoxygenation. ΔEI (dEI, the difference in EI between EImax and EImin) shows how many cells can sickle during one round of deoxygenation. Point of sickling (PoS, pO2 at 5% EI decrease) shows the oxygen tension when the first RBCs start to sickle. The area under the curve (from pO2min = 100 mmHg) is calculated in the parameter area. This summarizes EImax, EImin, and PoS. The capacity of sickled cells to unsickle during reoxygenation is represented in the parameter Recovery (percentage of EImax reached during reoxygenation). To aid in the interpretation, all data points were connected in every individual experiment by a line to graphically present the results. This figure has been modified from Rab et al.22 Please click here to view a larger version of this figure.
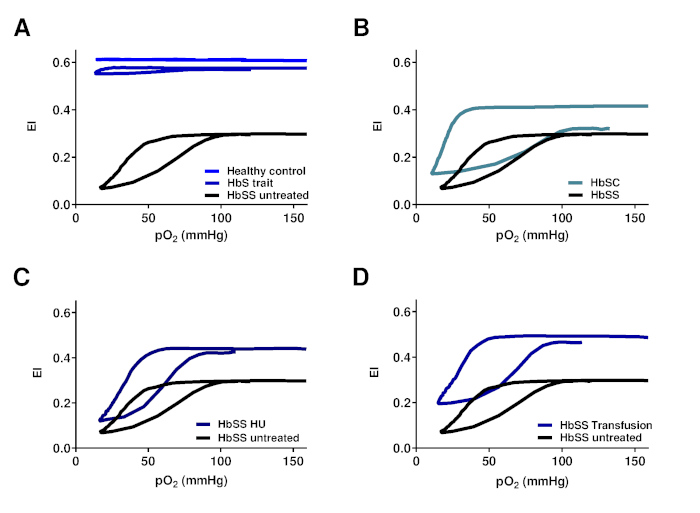
Figure 4. Oxygen gradient ektacytometry parameters correlate with genotype and treatment regimens of SCD patients with SCD. (A) Representative graph of RBCs of HbS carriers (HbS trait) and healthy controls in relation to untreated HbSS patients. (B) Representative graph of RBCs of patients with Hemoglobin SC Disease (HbSC) in relation to untreated HbSS patients. (C) Representative graph of RBCs of hydroxyurea treated homozygous SCD patients (HbSS HU) in relation to untreated HbSS patients. (D) Representative graph of RBCs of HbSS patients treated with blood transfusion (HbSS transfusion) in relation to untreated HbSS patients. This figure has been modified from Rab et al.22 Please click here to view a larger version of this figure.
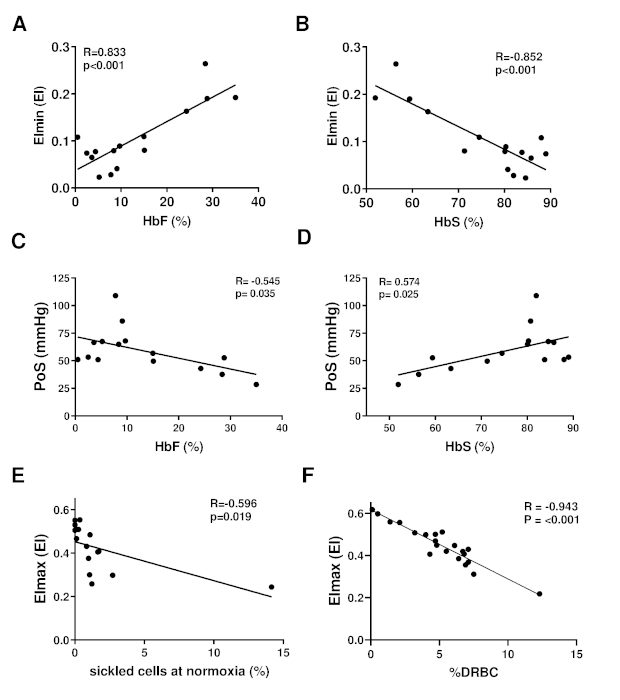
Figure 5. Oxygen gradient ektacytometry parameters are associated with %HbF, %HbS, %sickled cells at normoxia and %dense RBCs. (A) Linear correlation of minimum elongation index (EImin) and %HbF of 15 HbSS or HbS/β-thalassemia patients without transfusion. (B) Linear correlation of EImin and %HbS. (C) Linear correlation of PoS and %HbF. (D) Linear correlation of PoS and %HbS. (E) Linear correlation of maximum EI (EImax) and percent of sickled cells at normoxia measured with digital microscopy. (F) Linear correlation of EImax and percentage dense RBCs (%DRBCs) of 21 patients with HbSS. This figure has been modified from Rab et al.22 Please click here to view a larger version of this figure.
| Settings | ||
| Files | Storage directory | |
| General options | Default medium viscosity | Viscosity of PVP |
| pO2 scan | Minimum aspiration time (s) | 60 |
| pO2 scan shear stress (Pa) | 30 | |
| Determine pO2 every (S) | 20 | |
| Moving average size | 2 | |
| pO2 scan step; Edit | 0 -OFF; 60 -ON; 1360 –OFF; 1640 -OFF | |
| Cal. Area between (mmHg) | 10 and 100 | |
| pO2 control | Off (unchecked) |
Table 1. The preferred setting of the ektacytometer.
