The mouse footpad inoculation model allows for characterization of the immunopathogenesis of alphaherpesvirus infection in vivo, including replication and spread of the infection from the inoculated footpad to the nervous system and the induction of specific neuroinflammatory responses.
In this study, we first abraded the mouse hind footpad and either mock-inoculated or inoculated the abraded region with a virulent strain of PRV (PRV-Becker). The site of abrasion was visible in the control footpad. A crust was formed at the abrasion site as part of the healing process (Figure 1, black arrow). In contrast, mice inoculated with PRV showed severe inflammation at the humane endpoint (82 hpi), characterized by swelling of the footpad and redness.
Following footpad inoculation with the virulent PRV-Becker strain, mice began showing clinical signs at 72 hpi, characterized by swelling of the inoculated footpad and increasingly frequent tremors. By 82 hpi, PRV-Becker infected mice showed constant tremors in the inoculated leg and distinctive PRV symptoms, including intense scratching and biting of the foot. Severe inflammation was also observed in the footpad. The inflammatory response induced during PRV infection was then further characterized, including the infiltration of immune cells into tissues.
Histopathological examination of several tissues was performed, including the inoculated footpad and DRG, followed by H&E staining of paraffin-embedded tissue sections. Epidermal necrosis and severe dermal inflammation (edema and fibrin) were observed in PRV-infected foot sections (Figure 2A, panel b). The epidermis, dermis, and connective tissues of infected mice showed a massive infiltration of neutrophils (identified by multilobed nuclei) marked with black arrows. Footpads of control mice were normal (Figure 2A, panel a). PRV-infected DRG showed minimal neuronal necrosis and mixed inflammation in infected mice while the DRG of control mice were normal (Figure 2B, panels a and b). The mixed inflammation infiltrate consisted mainly of neutrophils and lymphocytes.
Next, the kinetics of inflammatory cytokine production in mouse tissue after PRV footpad inoculation were established. Levels of specific inflammatory cytokines were quantified (i.e, interleukin-6 [IL-6] and granulocyte-colony stimulating factor [G-CSF]) from several tissues collected and homogenized from control and PRV-infected mice. The results demonstrated a significant increase of G-CSF levels in the footpad and DRG compared to controls at 7 hpi and 82 hpi (Figure 3A). Significant G-CSF levels were observed at 82 hpi in spinal cord, brain, heart, and liver tissue of PRV-infected mice compared to controls. Moreover, significant IL-6 levels were detected in all tissues of PRV-infected mice compared to controls starting at 24 hpi (Figure 3B).
The footpad inoculation model was further used to investigate PRV replication and spread from the inoculated footpad to the PNS and CNS and potential correlations with neuroinflammatory response development. PRV loads were quantified in several homogenized tissues by qPCR to amplify PRV DNA. DNA concentration was then converted to PFU, as previously described10. PRV loads were detected in the footpad starting at 24 hpi (~1 x 104 PFU/mg of tissue) and in DRG starting at 60 hpi (~1 x 103 PFU/mg of tissue; data not shown).
In a moribund state (82 hpi), PRV was detected in the footpad, DRG, spinal cord, and brain, with the highest concentration of PRV in DRG (~1 x 105 PFU/mg of tissue; Figure 4). PRV infection of DRG was confirmed by indirect immunofluorescence staining of DRG cryosections. PRV infection was detected in DRG neurons using anti-PRV gB antibody. PRV glycoprotein gB was expressed during late stages of infection in the cytoplasm of infected cells. As expected, the cytoplasmic expression of PRV gB (green) was confirmed in infected DRG, while no gB was expressed in control samples (Figure 5). Cell nuclei were identified with DAPI staining (blue).
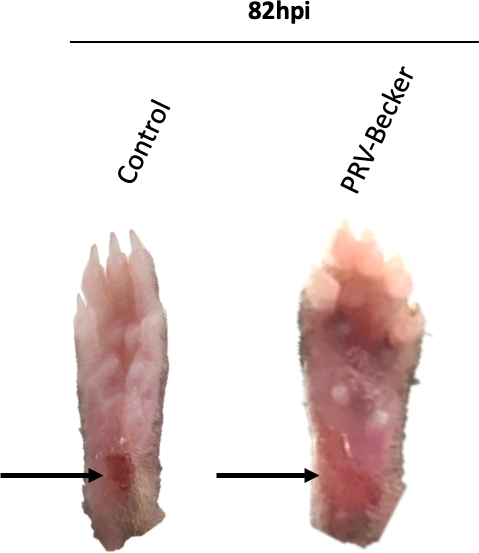
Figure 1: Representative images of mouse right hind paws after PRV inoculation. Mice are either mock-inoculated or inoculated with PRV in the abraded right hind footpad. PRV-inoculated footpad shows signs of inflammation, including redness and swelling at humane endpoint (82 hpi). The footpad of control mice appears normal with a dark red crust at the abraded site, indicating that the wound is healing. Black arrows indicate the site of abrasion. This figure has been modified from a previous publication11. Please click here to view a larger version of this figure.
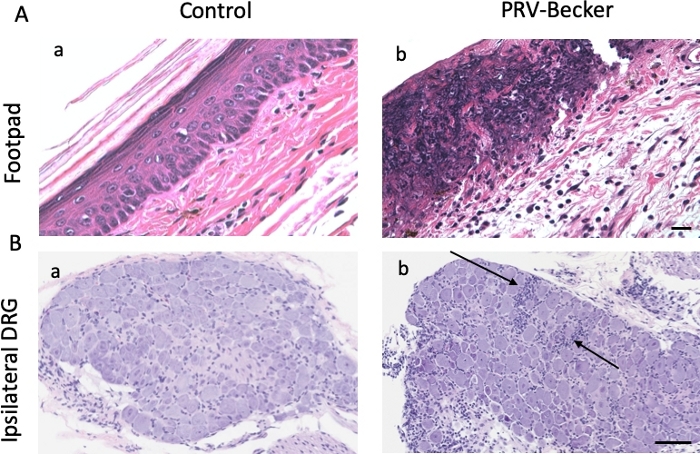
Figure 2: Histopathological findings in footpad and DRG after PRV footpad inoculation. Hematoxylin and eosin (H&E) staining of (A) mouse inoculated footpads and (B) and ipsilateral DRG from control (panel a) and PRV-infected (panel b) mice at 82 hpi. Histopathological manifestations observed in PRV-infected tissues (epidermal and neuronal necrosis and neutrophil infiltration) are absent from all examined mock-infected mice. Results are representative of three biological replicates for a given type of tissue. Black arrows indicate representative areas of inflammation with immune cell infiltration. Scale bars (50 μm) are indicated for each picture. This figure has been modified from11. Please click here to view a larger version of this figure.
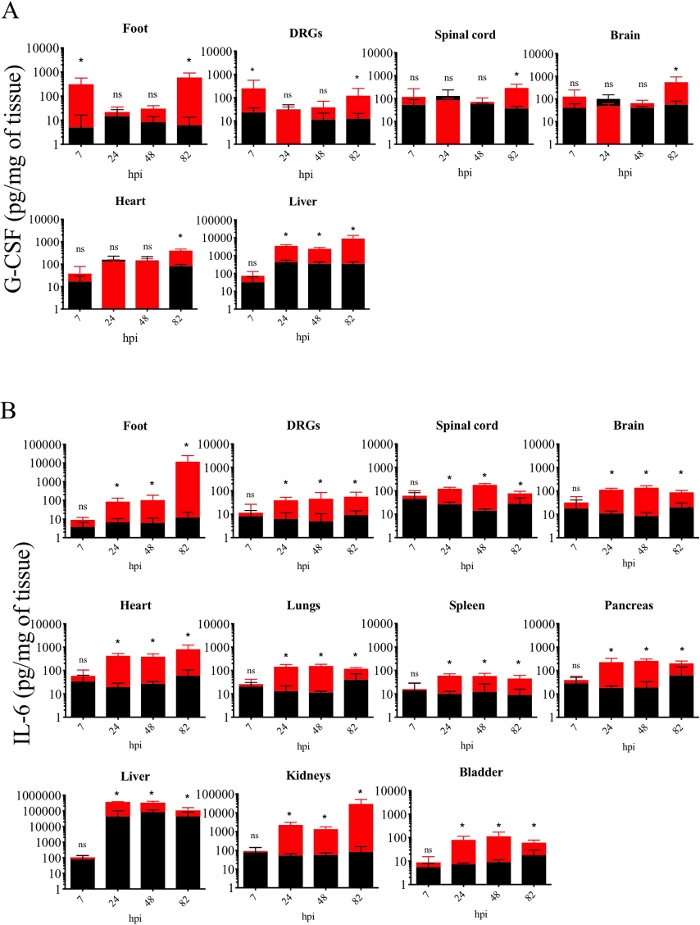
Figure 3: Kinetics of inflammatory cytokine production in homogenized mouse tissues after PRV footpad inoculation. (A) G-CSF and (B) IL-6 protein levels detected in PRV-infected (red) and control (black) mouse homogenized tissues at different hpi. Protein levels are quantified by ELISA and expressed as picogram (pg) per milligram (mg) of homogenized tissue (n = 5 per group, *p < 0.05, ns = not significant). This figure has been modified from a previous publication12. Please click here to view a larger version of this figure.
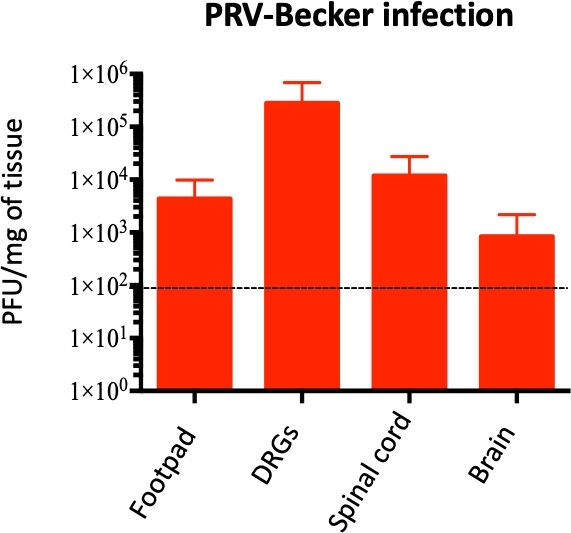
Figure 4: Quantification of PRV genome in mouse homogenized tissues. PRV DNA is quantified in homogenized mouse tissues by qPCR using PRV UL54 primers. PRV loads are expressed as plaque forming units (PFU) per mg of tissue. PRV DNA is detected only in the foot, DRG, spinal cord, and brain (and not in other tissues), n = 10 per group. Dotted line shows the detection limit. This figure has been modified from a previous publication11. Please click here to view a larger version of this figure.
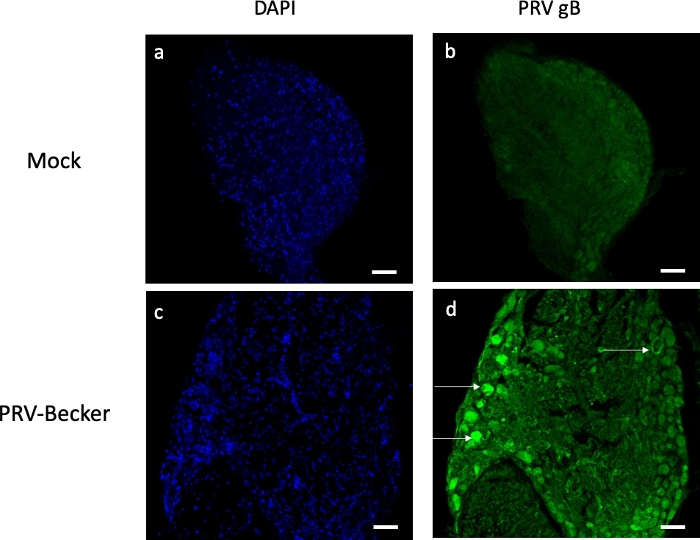
Figure 5: Assessment of PRV infection in DRG neurons by immunofluorescence staining. Confocal Z-stack images of mock- and PRV-infected DRG neurons after immunofluorescence staining using a mouse antibody specific for PRV gB (green). Cell nuclei are stained with DAPI (blue, panels a and c). Panel d shows several PRV-infected neurons expressing gB (white arrows). No gB expression is detected in the control DRG sections (panel b). Scale bars (50 μm) are indicated for each picture. Please click here to view a larger version of this figure.
