Biomaterials are often studied and used as scaffolds for cell-based tissue regeneration and depots for targeted, sustained delivery of therapeutics1. Within this field, injectable biomaterials are growing in popularity as they are minimally invasive, which reduces the risk of infection, pain and scarring associated with implantation2. Further, because they are usually applied as fluids, they conform perfectly to tissue defects, and drugs and cells may be mixed into them immediately prior to the application3,4,5. As such, while injectable biomaterials may be manufactured as pre-loaded syringes, they are often prepared by clinicians directly prior to application. For example, cements begin to set once the powder and liquid phases are mixed, and so cannot be stored for long periods before use6. The characterization of these materials is thus time dependent and inextricably linked to their preparation.
Common injectable biomaterials include calcium cements, polymethyl methacrylate, bioglasses, and various polymeric hydrogels3,7. Unlike traditional injections of drugs, which have the same rheological properties as water, these injectable biomaterials are typically more viscous, non-Newtonian, may have some elastic character, and may also change over time. Therefore, the injectability of these materials cannot be assumed but must be assessed experimentally. By quantifying the force required for injection and correlating it to the ease of injection, early decisions about which biomaterial formulations, syringe, and needle sizes to take forward may be made early in the developmental process8. Such experiments may also quantify the effects of changing formulations on injectability9.
There are several methods to assess the properties of injectable materials. Rotational rheology is often utilized to assess viscosity, non-Newtonian behavior, post-shear recovery, setting time, and other properties of these materials10,11,12. Whilst this type of test is useful to establish fundamental properties of the materials, these properties do not correlate directly to injectability. For a Newtonian fluid and cylindrical syringe and needle, the injection force can be estimated from a form of the Hagen–Poiseuille equation13:
Where F is the force required for injection (N), Rs is the internal syringe radius (m), Rn is the internal needle radius (m), L is the needle length (m), Q is fluid flow rate (m3 s-1), η is the dynamic viscosity (Pa.s) and Ff is the friction force between the plunger and barrel wall (N). Thus, if the viscosity is measured via rotational rheology, the dimensions of the syringe and needle are known and the flow rate estimated, the injection force can be estimated. However, this equation does not account for the conical end of the syringe or any other geometries, such as off-center outlets, and Ff must be estimated or found experimentally by mechanical testing. Further, biomaterials are typically not Newtonian, but exhibit complex rheological properties. For a simple shear thinning fluid, the equation becomes14:

Where n is the power index (-) and K is the consistency index (Pa.sn) from the Ostwald de Waele expression:  , where
, where  is the shear rate (s-1). The complexity vastly increases for materials whose rheological properties cannot be characterized by two values, and particularly for time-dependent materials such as setting cements. Additionally, if the material properties are shear dependent, then the material must be tested at the shear rate expected in the needle, which may far exceed the range of a rotational rheometer15.
is the shear rate (s-1). The complexity vastly increases for materials whose rheological properties cannot be characterized by two values, and particularly for time-dependent materials such as setting cements. Additionally, if the material properties are shear dependent, then the material must be tested at the shear rate expected in the needle, which may far exceed the range of a rotational rheometer15.
Another quantitative method for measuring injectability involves attaching pressure and displacement sensors to a syringe while performing an injection, either by hand or using a syringe pump. This equipment is relatively inexpensive, however, requires users to generate scripts and calibration curves to convert into force data16. Further, a syringe pump may not possess sufficient torque to compress the plunger at a precise rate if high forces are required to extrude viscous or semi-solid materials. Alternatively, utilizing these sensors when injecting by hand may be useful as they can be used in a real clinical scenario, during clinical procedures17. However, this will take much longer and may introduce user bias, and will, therefore, need larger numbers of repetitions with different users to obtain reliable results. This may, thus, be more appropriate for materials that are further down the translational pipeline, or products already in clinical use.
In this protocol, a mechanical tester is used to compress the plunger at a set rate, and measure the force required to do so. This type of mechanical tester is common in materials laboratories and has been used to quantify injectability for various biomaterials18,19,20,21,22,23,24. This test can be used with any size and geometry of syringe and needle, containing any material. Further, in the case of biomaterials that are made immediately prior to the use, the exact formulation procedure that would be used in the clinic or surgery can be followed prior to testing. A further advantage of this procedure is that it is relatively fast; once the mechanical tester is set up, tens of samples can be studied in an hour, depending on extrusion speed and syringe volume. This is in contrast to rotational rheology, which typically takes at least 5 – 10 minutes per test, plus loading, equilibration and cleaning time. Using a mechanical tester produces a reliable extrusion rate equally over the plunger, which is particularly advantageous for viscous formulations or those with time dependent properties. Following testing, minimal post-processing of data is required to pull out important values for objective comparisons.
The set-up of the mechanical tester and clamping system is shown in Figure 1A. This protocol generates a table and graph of force versus displacement for each tested sample. A typical force displacement curve consists of three sections (Figure 1B): an initial gradient, as the plunger overcomes friction from the barrel and the material is accelerated, a force maximum, and a plateau, as the material is extruded at a steady state.
However, a distinct maximum only exists where the plateau force is lower than the force required to accelerate the plunger. As such, peaks are only seen for inviscid samples passing through wide needles. For viscous samples passing through a more narrow orifice, the force needed to inject the sample at constant speed is greater than the force required to overcome friction in the barrel and accelerate the material, and no distinct peak is seen (Figure 1C). For highly viscous samples or very narrow needles, the force required to extrude the material may be so great that the syringe buckles and fails, often with very little extrusion of the material (Figure 1D). If the material being injected contains particles or is undergoing setting, such as cement, filter pressing (preferential expulsion of the liquid phase) or bulk setting may occur, leading to incomplete injection (Figure 1E).
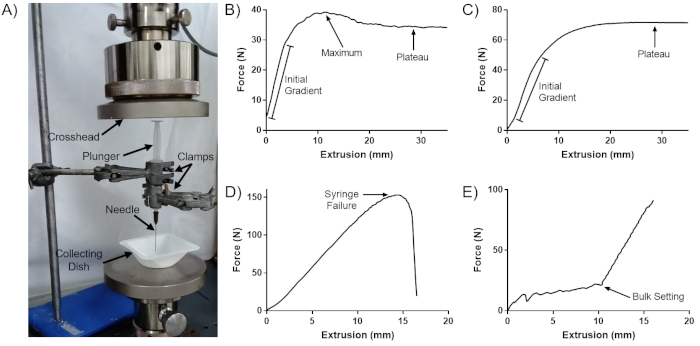
Figure 1: Sample curves generated by this protocol. (A) Set up of the mechanical tester for this protocol. (B) Typical force-extrusion curve. (C) Force-extrusion curve with no distinct maximum peak. (D) Force-extrusion curve for syringe failure. (E) Force-extrusion curve for a setting cement. This figure is adapted from Robinson et al.8. Please click here to view a larger version of this figure.
