Isolation of Human Primary Valve Cells for In vitro Disease Modeling
Summary
This protocol describes the collection of human aortic valves extracted during surgical aortic valve replacement procedures or from cadaveric tissue, and the subsequent isolation, expansion, and characterization of patient specific primary valve endothelial and interstitial cells. Included are important details regarding the processes needed to ensure cell viability and phenotype specificity.
Abstract
Calcific aortic valve disease (CAVD) is present in nearly a third of the elderly population. Thickening, stiffening, and calcification of the aortic valve causes aortic stenosis and contributes to heart failure and stroke. Disease pathogenesis is multifactorial, and stresses such as inflammation, extracellular matrix remodeling, turbulent flow, and mechanical stress and strain contribute to the osteogenic differentiation of valve endothelial and valve interstitial cells. However, the precise initiating factors that drive the osteogenic transition of a healthy cell into a calcifying cell are not fully defined. Further, the only current therapy for CAVD-induced aortic stenosis is aortic valve replacement, whereby the native valve is removed (surgical aortic valve replacement, SAVR) or a fully collapsible replacement valve is inserted via a catheter (transcatheter aortic valve replacement, TAVR). These surgical procedures come at a high cost and with serious risks; thus, identifying novel therapeutic targets for drug discovery is imperative. To that end, the present study develops a workflow where surgically removed tissues from patients and donor cadaver tissues are used to create patient-specific primary lines of valvular cells for in vitro disease modeling. This protocol introduces the utilization of a cold storage solution, commonly utilized in organ transplant, to reduce the damage caused by the often-lengthy procurement time between tissue excision and laboratory processing with the benefit of greatly stabilizing cells of the excised tissue. The results of the present study demonstrate that isolated valve cells retain their proliferative capacity and endothelial and interstitial phenotypes in culture upwards of several days after valve removal from the donor. Using these materials allows for the collection of control and CAVD cells, from which both control and disease cell lines are established.
Introduction
Calcific aortic valve disease (CAVD) is a chronic pathology characterized by inflammation, fibrosis, and macrocalcification of aortic valve leaflets. Progressive remodeling and calcification of the leaflets (termed aortic sclerosis) can lead to the obstruction of blood flow (aortic stenosis) which contributes to stroke and leads to heart failure. Currently the only treatment for CAVD is surgical or transcatheter aortic valve replacement (SAVR and TAVR, respectively). There is no non-surgical option to halt or reverse CAVD progression, and without valve replacement, mortality rates approach 50% within 2-3 years1,2,3. Defining the underlying mechanisms driving this pathology will identify potential novel therapeutic approaches.
In a healthy adult, aortic valve leaflets are approximately one millimeter thick, and their main function is to maintain the unidirectional flow of blood out of the left ventricle4. Each of the three leaflets is comprised of a layer of valve endothelial cells (VECs) that lines the outer surface of the leaflet and functions as a barrier. VECs maintain valve homeostasis by regulating permeability, inflammatory cell adhesion, and paracrine signaling5,6,7. Valve interstitial cells (VICs) comprise the majority of cells within the valve leaflet8. VICs are arranged in three distinctive layers in the leaflet. These layers are known as the ventricularis, the spongiosa, and the fibrosa9. The ventricularis faces the left ventricle and contains collagen and elastin fibers. The middle layer, the spongiosa, contains high proteoglycan content that provides shear flexibility during the cardiac cycle. The outer fibrosa layer is located close to the outflow surface on the aortic side and is rich in Type I and Type III fibrillar collagen which provide strength to maintain coaptation during diastole10,11,12. VICs reside in a quiescent state, however, factors such as inflammation, remodeling of the extracellular matrix (ECM), and mechanical stress may disrupt VIC homeostasis8,9,13,14,15,16. With loss of homeostasis, VICs activate and acquire a myofibroblast-like phenotype capable of proliferation, contraction, and secretion of proteins that remodel the extracellular millieu17. Activated VICs can transition into calcifying cells which is reminiscent of the differentiation of a mesenchymal stem cell (MSC) into an osteoblast15,17,18,19,20,21,22,23,24,25.
Calcification appears to initiate in the collagen-rich fibrosa layer from contributions of both VECs and VICs but expands and invades the other layers of the leaflet8. Thus, it is clear that both VECs and VICs respond to stimuli to upregulate the expression of osteogenic genes, however, the precise events driving the activation of osteogenic genes, as well as the complex interplay between the cells and the extracellular matrix of the leaflet, remain ill-defined. Murine models are not an ideal source to study non-genetic drivers of CAVD pathogenesis, as mice do not develop CAVD de novo26,27, hence the use of primary human tissues and the primary cell lines isolated from these tissues is necessary. In particular, obtaining these cells in high numbers and good quality is imperative, as the field of 3D cell cultures and organoid modeling is expanding and is likely to become an ex vivo human-based alternative to murine models.
The purpose of the present method is to share a workflow that has established the conditions to efficiently isolate and grow VECs and VICs obtained from surgically removed valves from human donors. Previous studies have shown successful isolation of VECs and VICs from porcine28 and murine valves29, to our knowledge this is the first to describe the isolation of these cells in human tissues. The protocol described here is applicable to human excised valves and greatly circumvents and improves the damage caused by the often-lengthy procurement time between tissue excision and laboratory processing by introducing the utilization of a cold storage solution, a buffered solution clinically utilized in organ transplants that greatly stabilizes cells of the excised tissue. The protocol described here also shows how to determine cell phenotype and guarantee high efficiency of cell survival with minimal cell cross-contamination.
Protocol
All patient samples are collected from individuals enrolled in studies approved by the institutional review board of the University of Pittsburgh in accordance with the Declaration of Helsinki. Cadaveric tissues obtained via the Center for Organ Recovery and Education (CORE) were approved by the University of Pittsburgh Committee for Oversight of Research and Clinical Training Involving Decedents (CORID).
1. Approval and safety
- Obtain Institutional Review Board (IRB) approval or an exempt memo for any collection of patient samples or cadaveric tissues in accordance with the Declaration of Helsinki.
- Take required institutional training to work with human tissues such as Bloodborne Pathogens Training, Biomedical Human Subjects Research, Privacy and Information Security, and Transportation and Shipping of Biological Materials.
2. Logistics and preparation
- Surgical Samples
- Ensure that a refrigerator is available and located near the operating room. Keep 50 mL conical tubes pre-labeled with de-identified nomenclature containing 40 mL of sterile aliquots of cold storage solution in this fridge for use by surgical staff. These tubes are stable at 4 °C until expiration date on the original package.
- Upon extraction, place valve tissue in these tubes. Place the tubes in a sealed secondary container such as a leak-proof plastic bag or a plastic container that is labeled with a biohazard label. Tissues are picked up and transported on ice according to institutional protocols for transporting biohazards.
- Cadaveric samples
- Submerge recovered organs in cold storage solution, place in a sealed secondary containment vessel, and transport on ice according to institutional protocols for transporting biohazards.
3. Reagents preparation
- Make collagen-coated plates at least the day before.
- In a 50 mL conical tube, mix 5 mL of isopropyl alcohol, 8.7 mL of acetic acid, and 0.5 µg of collagen I powder. Bring up to 50 mL with sterile water. Mix and filter through a 0.45 µm filter.
- Under a sterile cell culture hood, add enough collagen solution to 6 well plates and 10 cm dishes to just cover the entire bottom. Cover the plate and let sit for 4-6 h at room temperature. Remove the excess solution with a sterile pipette, place in a new sterile 50 mL conical tube, and save at 4 °C to make additional plates. Solution can be stored at 4 °C for several months.
- Dry the plates in a 37 °C incubator overnight, and subsequently store them in a resealable bag at 4 °C. Collagen-coated plates and dishes can be stored for several months.
- Autoclave the following items: tissue forceps, tissue scissors, cotton swabs and gauze pads.
- VEC growth media: Prepare and use endothelial cell growth medium according to manufacturer's protocols. Store in the dark at 4 °C. Warm to 37 °C just before use on cells, do not leave media in warming bath longer than necessary (10-15 min is sufficient). Use the media within one month of preparation.
- VIC growth media: Supplement DMEM base medium (4.5 g/L glucose, L-glutamine supplement, 110 mg/L sodium pyruvate)30 with 10% heat-inactivated FBS and 100 I.U./mL penicillin and 100 μg/mL streptomycin. Store in the dark at 4 °C for up to 3 months. Warm to 37 °C just before use on cells, do not leave media in warming bath longer than necessary (10-15 min is sufficient).
- Make sterile rinsing solution just before use. Supplement sterile PBS with 2.5 µg/mL fungicide, 0.05 mg/mL gentamicin and 5 µg/mL bactericide.
- Make sterile collagenase solution just before use. Add 5 mg of collagenase II to 5 mL of sterile fresh DMEM base medium. Mix well and sterilize the solution by passing through a 0.45 µm filter. Keep on ice until use.
4. Tissue preparation and processing
NOTE: Institutional approval for use of human tissues must be obtained prior to beginning work. While handling tissues, the following personal protective equipment (PPE) must be worn: a disposable liquid barrier wrap-around gown, or a dedicated button front lab coat with a liquid-barrier wrap around apron and disposable sleeve clovers; a full face shield, or safety glasses with a surgical mask; double gloves; close-toed shoes; and clothing to cover the legs. Comprehensive workflow diagrams of the tissue preparation for calcification assessment (Section 5) and cell isolation (Sections 6 and 7) are illustrated in Figure 1A,B respectively.
- Upon receipt of cadaveric organ specimen, excise the aortic root and submerge in a 50 mL conical tube of sterile rinsing solution. Upon receipt of surgical specimen, remove from transport vessels and submerge in a 50 mL conical tube of sterile rinsing solution. Place tube containing the tissue in ice bucket on rocker and mix for 10 min at room temperature (RT).
NOTE: Processing tissues as close as possible to the time of extraction will yield the best cell recovery, however viable cells can be collected upwards of 61 h post excision, and data show that VICs are more robust than VECs as time increases. If tissue cannot be processed immediately, when possible, remove tissue, perform step 4.1, and then put the tissue back in fresh sterile cold storage solution and keep at 4 °C until ready to proceed. Valves collected during night or weekend surgeries can be stored in 40 mL cold storage solution at 4 °C and still are able to yield viable cells more than 2 days post extraction. - Spray down tubes with 70% ethanol and move to a sterile hood. Remove tissue and excise two valve leaflets (Figure 2A). Place one leaflet in a cryogenic vial (or 2-3 vials if several smaller pieces are needed for future analysis) and snap freeze by dropping in liquid nitrogen then store at -80 °C.
- If the valve is bicuspid, excise only one leaflet. Using scissors, cut the leaflet in half from the nodule to the hinge. Use one half of the leaflet for snap freezing and the other half for step 4.3.
- Process the second leaflet for paraffin embedding to assess calcification content by cutting it in half from nodule to hinge. Place both pieces in a cassette that is submerged in 4% paraformaldehyde (PFA), then place on a rocker at RT for a minimum of 2 h but no more than 4 h.
NOTE: Longer fixation times create more background with immunofluorescent staining. Once steps 4.2 and 4.3 are performed, move immediately to Section 6 and come back to step 4.4 after step 6.12. - After fixation, wash the tissues by submerging in fresh PBS for 1 h 3-4 times. After these washes, samples can stay in PBS at 4 °C for several months if needed. Proceed to next step just before embedding.
- Gradually change from PBS to 70% ethanol. Wash 30-60 min each step with 1:4 70% ethanol:PBS; 1:1 70% ethanol:PBS, 4:1 70% ethanol:PBS; 70% ethanol.
- Embed the tissue such that sections will reveal the three layers of the leaflet (Figure 1A) according to established protocols31. Alternatively, and if available, bring the tissue to a pathology core for embedding and cutting.
- After handling tissues, dispose or store PPE as appropriate and wash hands immediately. Decontaminate all equipment, surfaces, and solid and liquid wastes with a 1:10 dilution of bleach or detergent disinfectant. Allow 20 min for decontamination, then follow with a 70% ethanol rinse. Treat the cell culture hood with mycoplasma spray according to manufacturer's instructions.
5. Von Kossa staining for calcium content
NOTE: This can be done well after cell isolation and line establishment but be sure to link the calcification level of the tissue to documents pertaining to the primary cell line established.
- Cut 5 or 10 µm thick paraffin slices onto glass slides and bake slides at 65 °C for 1 h, then cool to RT.
- Using fresh solutions, deparaffinize slides by submerging as following: 100% xylene for 30 min, 2x; 100% ethanol for 3 min, 2x; 90% ethanol for 3 min; 80% ethanol for 3 min; 70% ethanol for 3 min; 50% ethanol for 3 min; ultrapure water for 3 min; keep in ultrapure water until next steps.
NOTE: Times above are minimum, each step may go longer. - Proceed with Von Kossa staining according to manufacturer's protocols.
- Assess full valve area microscopically and assign a control tissue (no sign of calcification) or CAVD (any evidence of calcification, Figure 2B).
6. Valve Endothelial Cell (VEC) isolation, expansion, and confirmation
- In a sterile cell culture hood, open the conical tube containing the remaining valve leaflet and place the leaflet in a new 50 mL conical tube filled with ice cold PBS. Cap tube and gently invert or place on a rocker for 2 min at RT.
- Remove tissue to a 60 mm dish filled with 5-7 mL of cold collagenase solution. Using forceps, dip both sides of the leaflet in the solution 3-4 times. Incubate the tissue for 5-10 min in the cell culture incubator at 37 °C, rocking the tissue gently every 2 min 3-4 times.
- Remove 2 mL of the solution from the dish and place in a sterile 15 mL conical tube. Place forceps at the nodule and use a dry sterile cotton swab to swipe from the forceps to the hinge, twirling the swab while moving it along the leaflet. Between each swipe, swish the swab in the solution in the 15 mL conical tube to remove the cells. Repeat to fully swab the surface of the tissue, then flip over and repeat on the other side.
- Holding the valve leaflet with forceps in one hand, and a 1 mL pipette in the other, rinse the surfaces of the leaflet with the solution in the dish. Once rinsed, transfer all the solution containing the VECs in the dish into the same 15 mL conical tube with the cells from the swab and proceed to Step 6.5. Place the remaining valve tissue in a new 15 mL conical tube with 7 mL of sterile collagenase solution and proceed to Step 7.1.
- Centrifuge the tube containing the VECs at 180 x g for 5 min to pellet the isolated VECs. Aspirate the supernatant and resuspend in 3 mL of VEC growth media. Centrifuge one more time and remove the supernatant. Resuspend the cells in 1 mL of growth media and determine the number of cells using a hemocytometer and trypan blue.
- Resuspend VEC pellet in 2 mL of VEC growth media and plate the cells in a collagen pre-coated well of a 6 well plate at approximately 5 x 105 cells/cm2. Let the cells grow at least 3-4 days, then remove media and replenish with fresh media. Repeat media changing every 4 days. VECs will grow in cobblestone shaped patches (Figure 3B, left panels).
- When VEC patches cover >80% of the plate, split cells at about 1.3 x 104 cells/cm2 depending on how fast they grow (if they reach 80% in less than 1 week split at a slightly lower number of cells/cm2).
- To split, wash cells two times with 2 mL DPBS then add enough dissociation reagent to just cover the surface of the cells. Incubate for 2-3 min at 37 °C, checking to make sure cells are not over incubated. Stop digestion by adding equal volume of VEC growth media and transfer liquid to a 15 mL tube. Centrifuge at 180 x g for 5 min, remove supernatant, and resuspend in appropriate volume of media for number of wells/plates needed.
NOTE: Once expanded into a 10 cm plate VECs may sometimes lose their morphology and change phenotype as they proliferate. This tends occurs when VECs are seeded at a low confluency during the establishment and expansion of the cell line. - To guarantee a pure culture consider utilizing CD31+ superparamagnetic beads with every splitting.
- For 1 x 108 or fewer cells (one 10 cm dish or less), prepare 25 µL of superparamagnetic beads by washing according to manufacturer's protocols.
NOTE: Step 6.10 is recommended to be performed before trypsinization of VECs. - Detach cells as in step 6.8 but resuspend in 500 µL of PBS with 0.1% BSA, pH 7.4, and place in a 2 mL centrifuge tube. Add 500 µL of washed and resuspended beads to the 2 mL tube of cells and incubate on a rotator for 20 min at 4 °C.
- Place tubes on the magnet for 2 min. While tube is still in the magnet, carefully remove supernatant. Remove tube from magnet, add 1 mL fresh PBS with 0.1% BSA, pipette gently 2-3 times, then place back on magnet for 2 min. Repeat 2 more times. After final removal of buffer, resuspend cells in growth media in volume needed for replating.
NOTE: Cells will still have beads, but these will not affect growth and will be removed in subsequent passages. - Once cells have been expanded, in addition to morphology, confirm VEC phenotype by positive staining for immunofluorescent markers such as von Willebrand factor (vWF), cadherin 5 (CDH5), or PECAM-1/CD31, and negative staining for VIC markers such as calponin 1 (CNN) or alpha-2 smooth muscle actin (αSMA, Figure 4, left panels).
7. Valve Interstitial Cell (VIC) isolation, expansion, and storage
- As stated in step 6.4, after removing VECs from the valve tissue, the leaflet is placed in a 15 mL conical tube with 7 mL collagenase solution. Incubate for 12 h in the cell culture incubator with the cap slightly open to allow gas exchange. Successful isolation of VICs can still occur with up to 18 h in collagenase solution.
- After incubation, in a sterile cell culture hood, mix the tissue gently by pipetting with a serological pipette to ensure the release of VICs from the leaflet tissue.
- Remove cell suspension and pass through a 0.70 μm filter into a 50 mL conical tube.
- Add 7 mL of VIC growth medium to the 50 mL tube and centrifuge at 180 x g for 5 min. Aspirate supernatant and resuspend cell pellet in 1 mL of VIC growth media and determine the cell number. Plate the VICs in a 60 mm tissue-culture treated dish at 1.3 x 104 cells/cm2.
- Let the cells grow at least 1-2 days before replacing media. Remove media and wash twice DPBS to remove residual debris and replace with fresh growth medium. Replenish medium every 2-3 days. VICs will grow in fibroblast shape (Figure 3B, right panels).
- When VICs reach a confluency of >90%, wash twice with DPBS to remove the excess media and detach the cells by adding appropriate volume of pre-warmed dissociation reagent to cover the plate (i.e., 2-3 mL per 10 cm dish). Incubate the dish in a 37 °C incubator. VICs will detach from the dish after 2-3 min of incubation. Add 4-6 mL of pre-warmed media.
NOTE: If cells take longer than 3 min to lift off the plate, the dissociation reagent may have lost potency. If needed, a cell scraper may be used to gently lift the cells. - Transfer the cell suspension to a tube and gently centrifuge at 180 x g for 5 min. After removing the supernatant, gently resuspend the cell pellet in pre-warmed VIC growth media and determine the number of viable cells by using a hemocytometer and trypan blue. Seed the viable cells at a 1:2 density of the original dish (i.e., ~ 1 × 106 cells per 10 cm dish or 1.3 x 104 cells/cm2).
- Assess VIC phenotype by positive staining for immunofluorescent markers such as αSMA, CNN, or SM22α and negative staining for VEC markers such as CD31, CDH5, or vWF (Figure 4, right panels).
NOTE: The protocol workflow presented here unbiasedly selects one leaflet for VECs and VICs isolation, while the remaining leaflets are utilized for Von Kossa staining (Section 5) and snap freezing.
8. Long-term cell storage
- Once expanded, freeze cells down for long-term storage. Wash cells twice with 2-5 mL DPBS then add enough dissociation reagent to detach cells as in steps 6.8 and 7.6. Stop digestion by adding equal volume of VEC or VIC growth media and transfer cell suspension to a 15 mL tube.
- Determine the number of viable cells by using a hemocytometer and trypan blue.
- Centrifuge at 180 x g for 5 min.
- Resuspend cells in chilled conditioned growth media to a cell density of ~ 3 × 106 cells/mL.
- Gently with swirling, add an equal volume of chilled 2x cryopreservation medium. This will bring cell concentration to ~ 1.5 × 106 cells/mL.
- Aliquot 1 mL into cryopreservation vials. Place vials in a cell freezing container, close, and invert 5-6 times to ensure cells remain suspended. Place container at -80 °C for 6-72 h or according to freezing container protocol. Remove vials from -80 °C and transfer to liquid nitrogen for long term storage.
Representative Results
The above protocol outlines the steps necessary for the handling of human valve tissues and the isolation and establishment of viable cell lines from these tissues. Leaflets of the aortic valve are processed for paraffin embedding, snap frozen for long term storage for biochemical or genetic analysis and digested for the isolation of VECs and VICs (Figure 1). While surgical specimens will likely have a clinical diagnosis of aortic stenosis and may exhibit heavy nodules of calcification that can be visible with the naked eye, aortic valve calcification is present in a significant number of elderly (>65 years old) individuals32, and because of this prevalence all tissues – surgical and cadaveric – are subjected to Von Kossa staining or similar procedure to assess whether calcification is present (Figure 2).
It was found that use of cold storage solution greatly stabilized the cells of the excised valve tissue. Cold storage solution is used in live organ transplants. It is flushed through organs either before or after removal from the donor and left in the vasculature of that organ during transportation on ice. It was observed that VEC lines were more readily established from donor specimens than surgical tissues, and the donor lines were more likely to retain their endothelial cell morphology for more passages. This was perplexing, as donor tissues would often not reach the lab for 12-24 hours postmortem while surgical tissue was obtained between 2 and 4 hours. Upon packing the surgical specimen tubes with cold storage solution instead of PBS, cell recovery greatly increased. As seen in Figure 3, both viable VECs and VICs can be obtained upwards of 61 hours post valve extraction. While a slightly higher percentage of live VICs are obtained than VECs when cells are isolated up to a day after valve excision, cells remain viable after 48 hours post excision. Up to 40% of the total recovered cells correspond to alive cells and we have observed consistent figures between biological replicates. Further, morphology inspection also confirms cell identity; while VECs appear as packed, cobblestone-like and growth contact-inhibited cells, VIC morphology is similar to myofibroblasts with a spindle shape. Immunostaining of the specimens confirmed that 91.8% ± 1.8 (n = 3) of expanded VECs were positive for the endothelial marker vWF whereas 92.0% ± 5.0 (n = 3) of expanded VICs were positive for the interstitial cell marker αSMA (Figure 4). These figures are in line with results reported previously33.
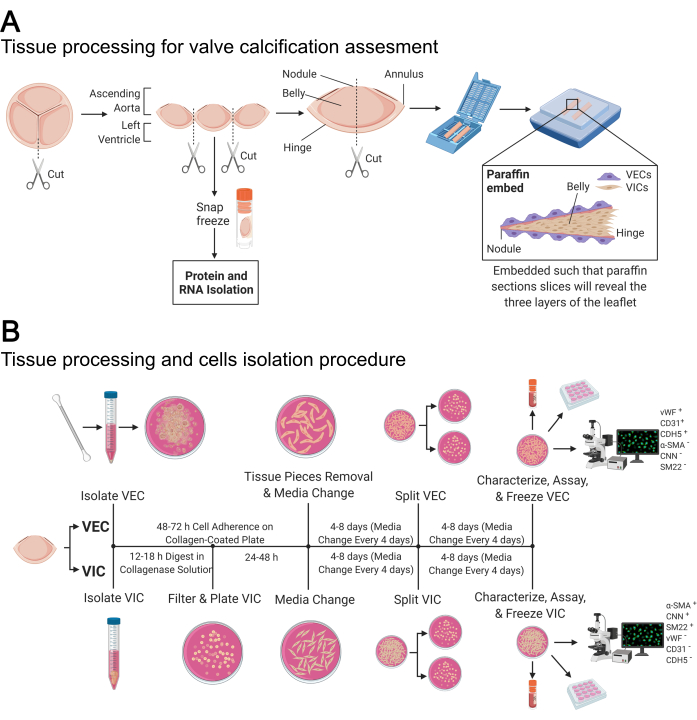
Figure 1: Valve tissue processing and cell isolation from human control and CAVD valves. (A) Schematic representation of tissue processing for assessment of calcification levels of the valves. (B) Schematic representation of the time course and steps for the isolation and characterization of human valve endothelial cells (VECs) and valve interstitial cells (VICs) from control and CAVD tissues. Please click here to view a larger version of this figure.
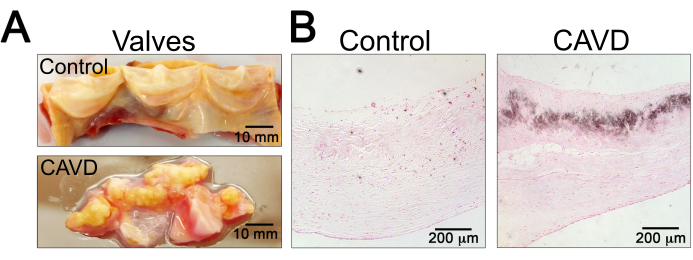
Figure 2: Assessment of Calcification. (A) Representative image of control (top) and calcified (bottom) valve tissues from human donors. Note the calcification nodules of the CAVD tissue can severely alter morphology and the ability to cleanly excise the leaflets. (B) Representative Von Kossa staining of control (left) and CAVD (right) valve tissue after fixation and further processing of the human valve tissue. Note calcification is revealed by the presence of dark precipitation in the leaflet tissue. Valve images were capture with a lab camera. Von Kossa stained valves were captured with a 10x objective, scale bar 200 µm. Please click here to view a larger version of this figure.
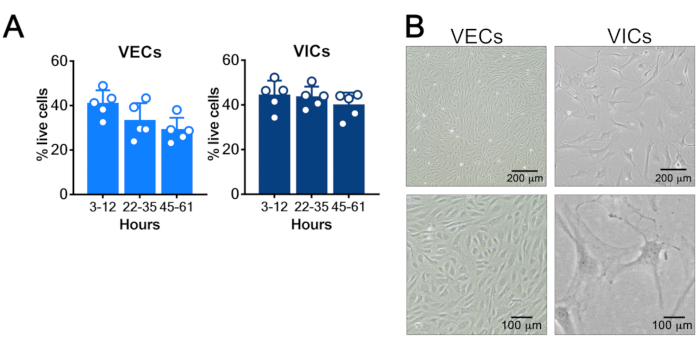
Figure 3: Assessment of Cell Survival (A) VECs and VICs survival curves. Three leaflets were obtained from five valve specimens. The first leaflet from each valve was processed immediately (3-12 h post extraction), the second leaflet was processed approximately 24 h later (22-35 h), and the third leaflet was processed approximately 48 h after obtaining the tissue (45-61 h). Valves leaflets were kept in cold storage solution at 4 °C until they were processed. The y-axis represents the percentage of live cells. (B) Morphology of healthy cultures of VECs (left panels) and VICs (right panels). Graphs show mean ± SD live cell proportion of cells isolated from n = 5 valve tissues. Images were captured with a 4x and 10x objective, scale bars 200 µm and 100 µm, respectively. Please click here to view a larger version of this figure.
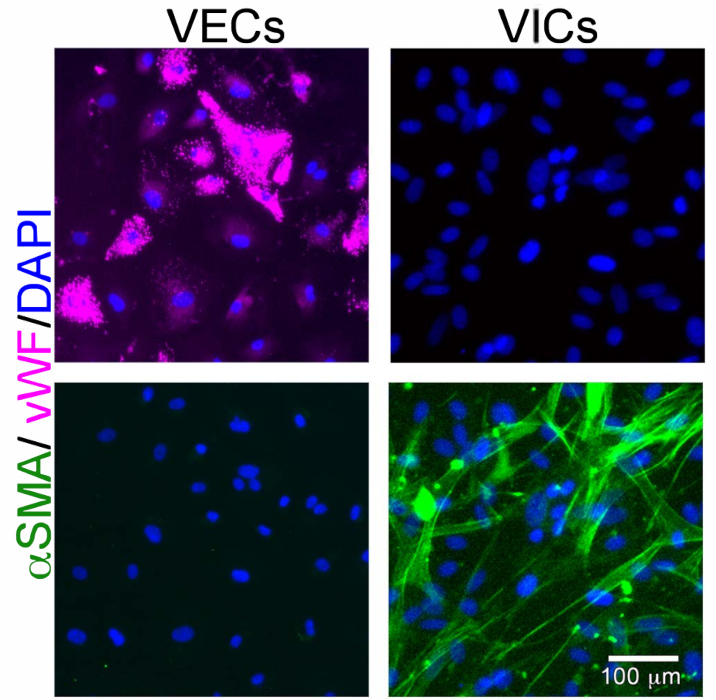
Figure 4: Representative immunofluorescent staining on VECs and VICs. VECs are positive for the endothelial marker von Willebrand Factor (vWF, left panels) whereas VICs are positive for the interstitial marker αSMA. Note our isolation protocol guarantees a high isolation efficiency; no cross-contamination between VECs and VICs is detected. Images were captured with a 10x objective, scale bar 100 µm. Please click here to view a larger version of this figure.
Discussion
Obtaining control and disease tissues from humans is critical for in vitro and ex vivo disease modeling; however, while one often speaks about the challenges of bridging the gap between bench to bedside, the reverse order – going from the surgical suite to the bench – is often just as daunting a gap. Essential for a basic scientist to obtain primary human tissue specimens is a collaboration with an invested surgeon scientist who has a team of nurses, surgical technicians, physician assistants, medical students and residents, and clinical protocol managers who can enroll and consent patients, participate and assist in the proper handling of excised tissues, and coordinate the logistics required for tissue pickup. Without the utmost effort from everyone involved to reduce the time from excision to cell isolation, vital cellular material and the information it contains will be irreparably altered or lost.
Critical to maintaining viability of the tissue specimens is the use of cold storage solution. This is the same solution used by the organ transplant teams at UPMC and other transplant medical centers. Better cell yield was obtained from cadaveric tissues that had been excised from the donor many hours beforehand than from tissues obtained more quickly from the operating room but kept in cold PBS. This accidental discovery has been essential for cell procurement from human tissues. Procurement time from tissue excision to delivery in the laboratory ranges from 1-5 hours for surgical tissue and upwards of 24 hours for cadaveric tissue. In comparison, procurement and processing of animal tissues can often be done within minutes of euthanasia, which is ideal for cell viability. In the absence of cold storage solution, it is likely that a medium suitable for the culturing of cells could also perform better than PBS, however this medium was not tested herein due to the success of the cold storage solution in live organ transplantation and to the receipt of cadaveric tissues in this solution. The solution is shelf-stable which is ideal for storage in operating rooms, and specific ingredients such as adenosine are known to promote beneficial responses to cellular stresses such as ischemia/hypoxia21,34.
Another essential step to obtaining viable cells is washing the tissues with fungicide, gentamicin, and bactericide. This short rinse helps to ensure that cells remain uncontaminated by bacteria and fungus. Equally critical are the steps to digest VECs out of the valve tissue, where in the span of just a few minutes, the VECs are detached and then swabbed off the surface of the valve leaflets. The subsequent digestion of the VICs that reside on the dense extracellular matrix of the leaflet has much more wiggle room for duration and strength. The unbiased tissue treatment described in this protocol allows the isolation of the main two cell populations present in the valve leaflet, VECs and VICs. Although a recent single cell transcriptome analysis has shown the co-existence of at least fourteen different cell subtypes residing in the human valve, including six non-valve derived stromal cells in CAVD tissue35, this diversity may represent variations due to effects from processing and digesting these hardened tissues, or it may be due to different microenvironments to which the leaflet cells are exposed: VECs are exposed to two different blood flows while VICs are embedded in three different extracellular matrix stratums8,9. The large-scale isolation protocol and analysis described herein ensure that over 90% of VECs and VICs correspond to their main phenotype. Although a degree of heterogenicity may be found, it does not affect the general outcomes of the study of VEC and VIC homeostasis8,9,13,14,15,16.
It is also important to note that patients and their valve tissues, and thus the cell lines procured from them, are not identical. Genetics, co-morbidities, handling during surgery and processing, and freshness of digestion solution ingredients may affect the growth rate and even perhaps the behavior or phenotype of the cells isolated. While the present study demonstrates the ability to yield a sufficient number of viable cells with this procedure, there may be innate or induced differences in these cell lines that may impact downstream experimentation. It is often difficult to know precisely the time since the tissue has been removed from the patient or donor, and particularly in the case of the latter, the time since circulation has stopped. Further, there is inherent variability among tissues regarding the number of viable valve cells obtained, the proliferative capacity of the cells, and the retention of cell phenotype. Cell lines may harbor genetic mutations – either congenital or somatic – of which the physician and research team are unaware, and the remodeling and subsequent handling of the tissues may also modify the cell phenotype or even epigenetics. As such, for all experiments in which these primary human cells are used, it is absolutely essential that biological replicates – i.e., cell lines obtained from different patients – be used, despite the substantial time and cost they incur. This helps ensure that any results are not due to confounding effects from the procurement and processing of the tissue. The variable proliferation rate of different cell lines can be adjusted for by either collecting cells in experiments at different times or seeding cells for experiments at different densities; no one answer is best for all experimental designs. While the complications are not insignificant, the use of primary human control and CAVD tissue-derived cell lines for in vitro and ex vivo experimental models is essential for defining the initiating factors and propagating processes that drive CAVD pathogenesis.
Disclosures
The authors have nothing to disclose.
Acknowledgements
We would like to thank Jason Dobbins for insightful discussion and critical reading of this manuscript. We would like to acknowledge the Center for Organ Recovery and Education for their help and support and thank tissue donors and their families for making this study possible. All patient samples are collected from individuals enrolled in studies approved by the institutional review board of the University of Pittsburgh in accordance with the Declaration of Helsinki. Cadaveric tissues obtained via the Center for Organ Recovery and Education (CORE) were approved by the University of Pittsburgh Committee for Oversight of Research and Clinical Training Involving Decedents (CORID).
Some figures created with Biorender.com.
CSH is supported by the National Heart, Lung, and Blood Institute K22 HL117917 and R01 HL142932, the American Heart Association 20IPA35260111.
Materials
| 0.45 μm filter | Thermo Scientific | 7211345 | Preparing plate with collagen coating |
| 10 cm cell culture plate | Greiner Bio-One | 664160 | Cell culture/cell line expansion |
| 10 mL serological pipet | Fisher | 14955234 | VEC/VIC isolation, cell culture, cell line expansion |
| 1000 μL filter tips | VWR | 76322-154 | Cell culture/cell line expansion |
| 10XL filter tips | VWR | 76322-132 | Cell culture/cell line expansion |
| 15 mL conical tubes | Thermo Scientific | 339650 | Tissue storage, VIC/VEC isolation |
| 16% paraformaldehyde aqueous solution | Electron Microscopy Sciences | 15710S | Tissue and cell fixative |
| 190 proof ethanol | Decon | 2801 | Disinfection |
| 1x DPBS: no calcium, no magnesium | Gibco | 14190250 | Saline solution. VIC/VEC isolation |
| 1x PBS | Fisher | BP2944100 | Saline solution. Tissue preparation, VIC/VEC isolation |
| 20 μL filter tips | VWR | 76322-134 | Cell culture/cell line expansion |
| 200 proof ethanol | Decon | 2701 | Deparaffinizing tissue samples |
| 2-propanol | Fisher | A416P 4 | Making collagen coated plates |
| 5 mL serological pipet | Fisher | 14955233 | VEC/VIC isolation, cell culture, cell line expansion |
| 50 mL conical tubes | Thermo Scientific | 339652 | Tissue storage, VIC/VEC isolation |
| 60 mm dish | GenClone | 25-260 | VEC isolation |
| 6-well cell culture plate | Corning | 3516 | Cell culture/cell line expansion |
| Acetic acid, glacial | Fisher | BP2401 500 | Making collagen coated plates |
| AlexaFluor 488 phalloidin | Invitrogen | A12379 | Fluorescent f-actin counterstain |
| Belzer UW Cold Storage Transplant Solution | Bridge to Life | BUW0011L | Tissue storage solution |
| Bovine Serum Albumin, Fraction V – Fatty Acid Free 25g | Bioworld | 220700233 | VEC confirmation with CD31+ Dynabeads |
| Calponin 1 antibody | Abcam | ab46794 | Primary antibody (VIC positive stain) |
| CD31 (PECAM-1) (89C2) | Cell Signaling | 3528 | Primary antibody (VEC positive stain) |
| CD31+ Dynabeads | Invitrogen | 11155D | VEC confirmation with CD31+ Dynabeads |
| CDH5 | Cell Signaling | 2500 | Primary antibody (VEC positive stain) |
| Cell strainer with 0.70 μm pores | Corning | 431751 | VIC isolation |
| Collagen 1, rat tail protein | Gibco | A1048301 | Making collagen coated plates |
| Collagenase II | Worthington Biochemical Corporation | LS004176 | Tissue digestion. Tissue preparation, VIC/VEC isolation |
| Conflikt Ready-to-use Disinfectant Spray | Decon | 4101 | Disinfection |
| Countess II Automated Cell Counter | Invitrogen | A27977 | Automated cell counter |
| Countess II reusable slide coverslips | Invitrogen | 2026h | Automated cell counter required slide cover |
| Coverslips | Fisher | 125485E | Mounting valve samples |
| Cryogenic vials | Olympus Plastics | 24-202 | Freezing cells/tissue samples |
| Disinfecting Bleach with CLOROMAX – Concentrated Formula | Clorox | N/A | Disinfection |
| DMEM | Gibco | 10569044 | Growth media. VIC expansion |
| EBM – Endothelial Cell Medium, Basal Medium, Phenol Red free 500 | Lonza Walkersville | CC3129 | Growth media. VEC expansion |
| EGM-2 Endothelial Cell Medium-2 – 1 kit SingleQuot Kit | Lonza Walkersville | CC4176 | Growth media supplement. VEC expansion |
| EVOS FL Microscope | Life Technologies | Model Number: AME3300 | Fluorescent imaging |
| EVOS XL Microscope | Life Technologies | AMEX1000 | Visualizing cells during cell line expansion |
| Fetal Bovine Serum – Premium Select | R&D Systems | S11550 | VIC expansion |
| Fine scissors | Fine Science Tools | 14088-10 | Tissue preparation, VIC/VEC isolation |
| Fisherbrand Cell Scrapers | Fisher | 08-100-241 | VIC expansion |
| Fungizone | Gibco | 15290-026 | Antifungal: Tissue preparation, VIC/VEC isolation |
| Gentamicin | Gibco | 15710-064 | Antibiotic: Tissue preparation, VIC/VEC isolation |
| Glass slides | Globe Scientific Inc | 1358L | mounting valve samples |
| Goat anti-Mouse 488 | Invitrogen | A11001 | Fluorescent secondary Antibody |
| Goat anti-Mouse 594 | Invitrogen | A11005 | Fluorescent secondary Antibody |
| Goat anti-Rabbit 488 | Invitrogen | A11008 | Fluorescent secondary Antibody |
| Goat anti-Rabbit 594 | Invitrogen | A11012 | Fluorescent secondary Antibody |
| Invitrogen Countess II FL Reusable Slide | Invitrogen | A25750 | Automated cell counter required slide |
| Invitrogen NucBlue Fixed Cell ReadyProbes Reagent (DAPI) | Invitrogen | R37606 | Fluorescent nucleus counterstain |
| LM-HyCryo-STEM – 2X Cryopreservation media for stem cells | HyClone Laboratories, Inc. | SR30002 | Frozen cell storage |
| Mounting Medium | Fisher Chemical Permount | SP15-100 | Mounting valve samples |
| Mr. Frosty freezing container | Nalgene | 51000001 | Container for controlled sample freezing |
| Mycoplasma-ExS Spray | PromoCell | PK-CC91-5051 | Disinfection |
| Penicillin-Streptomycin | Gibco | 15140163 | Antibiotic. VIC expansion |
| Plasmocin | Invivogen | ANTMPT | Anti-mycoplasma. VIC/VEC isolation and expansion |
| SM22a antibody | Abcam | ab14106 | Primary antibody (VIC positive stain) |
| Sstandard pattern scissors | Fine Science Tools | 14001-14 | Tissue preparation, VIC/VEC isolation |
| Sterile cotton swab | Puritan | 25806 10WC | VEC isolation |
| Swingsette human tissue cassette | Simport Scientific | M515-2 | Tissue embedding container |
| Taylor Forceps (17cm) | Fine Science Tools | 11016-17 | Tissue preparation, VIC/VEC isolation |
| Trypan Blue Solution, 0.4% | Gibco | 15250061 | cell counting solution |
| TrypLE Express Enzyme | Gibco | 12604021 | Splitting VIC/VECs |
| Von Kossa kit | Polysciences | 246331 | Staining paraffin sections of tissues for calcification |
| von Willebrand factor antibody | Abcam | ab68545 | Primary antibody (VEC positive stain) |
| Xylenes | Fisher Chemical | X3S-4 | Deparaffinizing tissue samples |
| αSMA antibody | Abcam | ab7817 | Primary antibody (VIC positive stain) |
References
- Lamprea-Montealegre, J. A., Otto, C. M. Health behaviors and calcific aortic valve disease. Journal of Amercan Heart Association. 7, (2018).
- Nishimura, R. A., et al. AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. 129, 2440-2492 (2014).
- Clark, M. A., et al. Clinical and economic outcomes after surgical aortic valve replacement in Medicare patients. Risk Manag Healthc Policy. 5, 117-126 (2012).
- Misfeld, M., Sievers, H. H. Heart valve macro- and microstructure. Philosophical Transactions of Royal Society of London B Biological Sciences. 362, 1421-1436 (2007).
- Anstine, L. J., Bobba, C., Ghadiali, S., Lincoln, J. Growth and maturation of heart valves leads to changes in endothelial cell distribution, impaired function, decreased metabolism and reduced cell proliferation. Journal of Molecular and Cell Cardiology. 100, 72-82 (2016).
- Mahler, G. J., Butcher, J. T. Inflammatory regulation of valvular remodeling: the good(?), the bad, and the ugly. Internation Journal of Inflammation. 2011, 721419 (2011).
- Gould, S. T., Matherly, E. E., Smith, J. N., Heistad, D. D., Anseth, K. S. The role of valvular endothelial cell paracrine signaling and matrix elasticity on valvular interstitial cell activation. Biomaterials. 35, 3596-3606 (2014).
- Leopold, J. A. Cellular mechanisms of aortic valve calcification. Circulation: Cardiovascular Intervention. 5, 605-614 (2012).
- Chen, J. H., Simmons, C. A. Cell-matrix interactions in the pathobiology of calcific aortic valve disease: Critical roles for matricellular, matricrine, and matrix mechanics cues. Circulation Research. 108, 1510-1524 (2011).
- Sacks, M. S., Schoen, F. J., Mayer, J. E. Bioengineering challenges for heart valve tissue engineering. Annual Review of Biomedical Engineering. 11, 289-313 (2009).
- Taylor, P. M., Batten, P., Brand, N. J., Thomas, P. S., Yacoub, M. H. The cardiac valve interstitial cell. Internation Journal of Biochemistry and Cell Biology. 35, 113-118 (2003).
- Taylor, P. M., Allen, S. P., Yacoub, M. H. Phenotypic and functional characterization of interstitial cells from human heart valves, pericardium and skin. Journal of Heart Valve Disease. 9, 150-158 (2000).
- Rajamannan, N. M., et al. Calcific aortic valve disease: not simply a degenerative process: A review and agenda for research from the National Heart and Lung and Blood Institute Aortic Stenosis Working Group. Executive summary: Calcific aortic valve disease-2011 update. Circulation. 124, 1783-1791 (2011).
- Wang, H., Leinwand, L. A., Anseth, K. S. Cardiac valve cells and their microenvironment–insights from in vitro studies. Nature Reviews Cardiology. 11, 715-727 (2014).
- Yutzey, K. E., et al. Calcific aortic valve disease: a consensus summary from the Alliance of Investigators on Calcific Aortic Valve Disease. Arteriosclerosis, Thrombosis, and Vascular Biology. 34, 2387-2393 (2014).
- Raddatz, M. A., Madhur, M. S., Merryman, W. D. Adaptive immune cells in calcific aortic valve disease. American Journal of Physiology-Heart and Circulation Physiology. 317, 141-155 (2019).
- Liu, A. C., Joag, V. R., Gotlieb, A. I. The emerging role of valve interstitial cell phenotypes in regulating heart valve pathobiology. American Journal of Pathology. 171, 1407-1418 (2007).
- Liu, A. C., Gotlieb, A. I. Characterization of cell motility in single heart valve interstitial cells in vitro. Histology and Histopathology. 22, 873-882 (2007).
- Yip, C. Y., Chen, J. H., Zhao, R., Simmons, C. A. Calcification by valve interstitial cells is regulated by the stiffness of the extracellular matrix. Arteriosclerosis, Thrombosis, and Vascular Biology. 29, 936-942 (2009).
- Song, R., Fullerton, D. A., Ao, L., Zhao, K. S., Meng, X. An epigenetic regulatory loop controls pro-osteogenic activation by TGF-beta1 or bone morphogenetic protein 2 in human aortic valve interstitial cells. Journal of Biological Chemistry. 292, 8657-8666 (2017).
- Xu, M. H., et al. Absence of the adenosine A2A receptor confers pulmonary arterial hypertension and increased pulmonary vascular remodeling in mice. Journal of Vascular Research. 48, 171-183 (2011).
- Jian, B., Narula, N., Li, Q. Y., Mohler, E. R., Levy, R. J. Progression of aortic valve stenosis: TGF-beta1 is present in calcified aortic valve cusps and promotes aortic valve interstitial cell calcification via apoptosis. Annals of Thoracic Surgery. 75, 465 (2003).
- Bogdanova, M., et al. Interstitial cells in calcified aortic valves have reduced differentiation potential and stem cell-like properties. Science Reports. 9, 12934 (2019).
- Gendron, N., et al. Human aortic valve interstitial cells display proangiogenic properties during calcific aortic valve disease. Arteriosclerosis, Thrombosis, and Vascular Biology. 41 (1), 415-429 (2021).
- Wirrig, E. E., Yutzey, K. E. Conserved transcriptional regulatory mechanisms in aortic valve development and disease. Arteriosclerosis, Thrombosis and Vascular Biology. 34, 737-741 (2014).
- Honda, S., et al. A novel mouse model of aortic valve stenosis induced by direct wire injury. Arteriosclerosis, Thrombosis and Vascular Biology. 34, 270-278 (2014).
- Sider, K. L., Blaser, M. C., Simmons, C. A. Animal models of calcific aortic valve disease. International Journal of Inflammation. 2011, 364310 (2011).
- Gould, R. A., Butcher, J. T. Isolation of valvular endothelial cells. Journal of Visualized Experiments. (46), e2158 (2010).
- Miller, L. J., Lincoln, J. Isolation of murine valve endothelial cells. Journal of Visualized Experiments. (90), e51860 (2014).
- Selig, J. I., et al. Impact of hyperinsulinemia and hyperglycemia on valvular interstitial cells – A link between aortic heart valve degeneration and type 2 diabetes. Biochimica Biophysica Acta Molecular Basis of Disease. 1865, 2526-2537 (2019).
- Fischer, A. H., Jacobson, K. A., Rose, J., Zeller, R. Paraffin embedding tissue samples for sectioning. CSH Protocols. 2008, (2008).
- Martinsson, A., et al. Temporal trends in the incidence and prognosis of aortic stenosis: A nationwide study of the Swedish population. Circulation. 131, 988-994 (2015).
- Rabkin-Aikawa, E., Farber, M., Aikawa, M., Schoen, F. J. Dynamic and reversible changes of interstitial cell phenotype during remodeling of cardiac valves. Journal of Heart Valve Diseases. 13, 841-847 (2004).
- St Hilaire, C., Carroll, S. H., Chen, H., Ravid, K. Mechanisms of induction of adenosine receptor genes and its functional significance. Journal of Cell Physiology. 218, 35-44 (2009).
- Xu, K., et al. Cell-type transcriptome atlas of human aortic valves reveal cell heterogeneity and endothelial to mesenchymal transition involved in calcific aortic valve disease. Arteriosclerosis, Thrombosis and Vascular Biology. 40, 2910-2921 (2020).
