What to do
Successful double resin injection is achieved when both the intrahepatic bile ducts and portal vein vasculature are well filled. As a quality control step, clearing one lobe (for example, the left lateral lobe) allows for verification of a successful injection, followed by imaging of lobes of interest. The optically cleared lobe can be scanned later using microCT; hence it is possible to optically clear the whole liver. In well-injected mouse liver, the portal vein vasculature should be filled with resin until the liver periphery and resin should be visible in side-branches (Figure 4), and this architecture is faithfully recapitulated in microCT scanned and segmented data. Further, well-injected intrahepatic bile ducts should be visible next to the main portal vein branches extending almost to the periphery, and resin should be visible in the major side branches. If the control lobe passes the quality control step, the lobes of interest (included the optically cleared one) can be scanned with microCT. The result of the segmented data from a well-injected liver is shown for a P15 mouse (Figure 4A,B) and an adult mouse (Figure 4C,D).
What not to do
Intact liver tissue is a prerequisite for successful injection. Take extra care when cutting the abdominal cavity and diaphragm not to accidentally nick the liver tissue. If there is physical damage to the liver during this procedure, the resin is very likely to leak out during portal vein injection (Figure 5A). It is not possible to achieve a good injection of the vascular system if the liver is physically damaged.
One of the common mistakes is underfilling the liver with resin that can lead to challenges for visualization or analysis. One of the causes for system underfilling is resin hardening prematurely in the needle or the tip of the tubing before the injection is completed (Figure 5B, blue arrowheads, brackets depict large bubbles). A good practice is to use one injection set per animal and work fast after the curing agent is added to the resin. If the resin hardens during the injection (which can be observed by a half-filled system, here exemplified with a half-filled portal vein vasculature) remove the tubing, cut the tip of the tubing (always diagonally to create a beveled tip), and push the plunger. If resin begins to drip again, carefully re-insert the tubing and secure it with the suture. If the resin has hardened in the needle, replace the tubing completely, fill it with resin (avoiding bubbles), carefully re-insert the tubing, and secure it with the suture. It can be challenging to replace the tubing, especially in young postnatal mice <P30, as the tissue is more fragile. Another cause of poor resin filling of portal vein vasculature can be insufficient transcardial perfusion (Figure 5C, blue arrowheads denote blood visible in terminal branches). This can be observed when the tips of the vessels are filled with blood instead of resin. To avoid this, ensure that the portal vein (outside the liver) does not contain any blood before the injection. The third cause of underfilled liver is when the tubing is inserted too deep into the liver and enters a branch towards one of the lobes. To prevent this, insert the tubing at a minimum of 0.5 cm from the entry to the liver.
Conversely, one, or both, of the systems become overfilled with resin (Figure 5D). It is necessary to visually monitor the liver throughout the injection. Biliary system casting with resin is more challenging than portal vein resin casting since resin-filled ducts are only faintly visible on the liver surface, and it is difficult to assess when the system is nearly full and when to stop. When small yellow resin dots appear on the liver surface (Figure 2Ci, blue arrowhead), this is a sign that the biliary system is completely filled, and the resin is starting to leak out of the ducts. Minor resin leakage can be manually corrected during microCT data segmentation (Figure 5D, right panels).
If the injection pressure is too high, this can cause vessels or ducts to rupture (Figure 5E), irreversibly damaging vessel or duct architecture. The liver will not be suitable for microCT scanning or analysis. To avoid resin overfilling, optimize the right volume and pressure used for injection in each mouse model. When working with mice that have been challenged with a toxic diet, genetic modification, or liver injury that affects the biliary or venous systems, or liver stiffness, the injection pressure and volume may need to be adjusted as volume and pressure tolerated may be different from the wild type mice. This protocol describes the manual injection of the two systems, but it is possible to connect the syringe to a pump to standardize the injection pressure. Bubbles are another very common injection artifact that leads to sparse filling of the tubular networks (Figure 5F–H, blue arrowheads). To avoid bubble formation, make sure that the syringe and tubing do not contain any bubbles, are completely filled with resin, and the resin is dripping from the tip of the tubing before injection. Small bubbles that appear as negative areas on the microCT data can be manually corrected during post-processing steps, although this is laborious.
Fresh is the best
Using fresh yellow resin is a crucial factor, significantly affecting the contrast of the two resins and the microCT data segmentation. When the freshly opened resin is used (Figure 6A) there is a clear difference in contrast between the yellow resin-injected bile ducts (bright white) and the green resin-injected portal veins (bright grey). Liver that is injected with fresh resin is easily processed using automated global thresholding. With prolonged storage, the resin precipitates, and the contrast diminishes. After 3 months of storage, the contrast can still be sufficient to distinguish the portal vein from the bile duct (Figure 6B), but precipitation affects the mixing of the two resins, which is visible as a heterogeneous opacity in the filled portal vein (Fig 6B, blue arrowheads). Heterogeneous contrast negatively affects the automated thresholding and necessitates manual corrections, which increases the processing time. If the resin is older than six months, the contrast has degraded to a point at which it is not possible to distinguish the yellow-injected bile duct from the green-injected portal vein based on their contrast alone (Figure 6C). In this case, the bile duct and portal vein must be segmented manually based on their diameter and position in the hilar region and followed manually throughout the entire microCT data. This procedure is extremely time-consuming and best avoided.
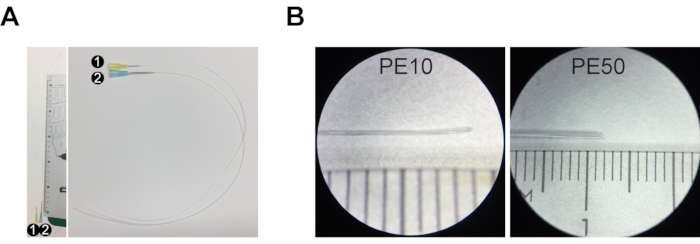
Figure 1: Injection set for resin casting. (A) Injection set #1 comprises a 30 G needle and PE10 tubing that is ~30 cm long. Injection set #2 is composed of a 23 G needle and PE50 tubing ~30 cm long. (B) The tip of the tubing is stretched and cut at an angle to create a beveled tip. The ruler in A and B is a centimeter ruler, with major increments of 1 cm, intermediate increments of 5 mm, and minor increments of 1 mm. Please click here to view a larger version of this figure.
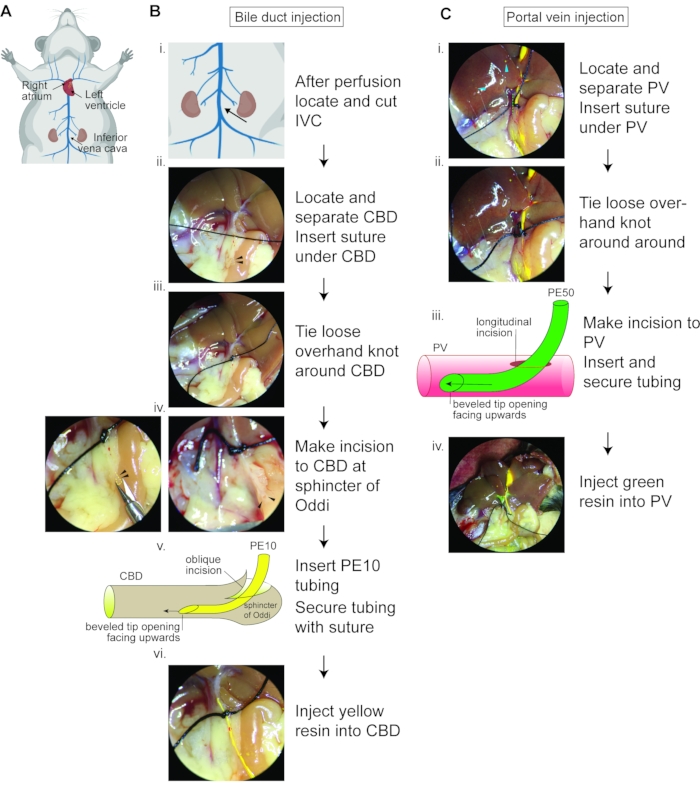
Figure 2: Double resin casting flow chart. (A) Schematic showing the murine venous circulatory system and the heart with highlighted right atrium, which should be cut away before perfusion, and the left ventricle into which the needle should be inserted for perfusion to wash away the blood from the circulatory system. The inferior vena cava should be severed under the kidneys to relieve vascular pressure. (B) Bile duct resin injection flow chart. (i) Zoom image of (A) depicting where to sever the IVC. (ii) Image depicting the common bile duct (yellow dotted line) from the liver hilar region to the sphincter of Oddi (black arrowheads), with suture thread under the cleared common bile duct. (iii) Suitable position for loose overhand knot around common bile duct. (iv) The yellow dotted line and black arrowheads label the sphincter of Oddi, demonstrating the oblique angle for incision and how the opening should appear after the oblique angle incision. (v) Schematic demonstrating the orientation of the PE10 tubing bevel opening (upwards) upon insertion. (vi) Appearance of yellow resin being injected; resin should easily pass the loosely tied knot. IVC, inferior vena cava; CBD, common bile duct. (C) Portal vein resin injection flow chart. (i) The green dotted line marks the portal vein from the hilar region. The blue arrowheads label the overfilled biliary system. (ii) Suitable location for loose overhand knot around portal vein. (iii) Schematic demonstrating the bevel opening (upward) upon insertion. (iv) Appearance of liver upon injection of green resin and yellow resin; note the resin-filled blood vessel in the liver periphery. PV, portal vein. Figure 2A was created with Biorender.com. Please click here to view a larger version of this figure.
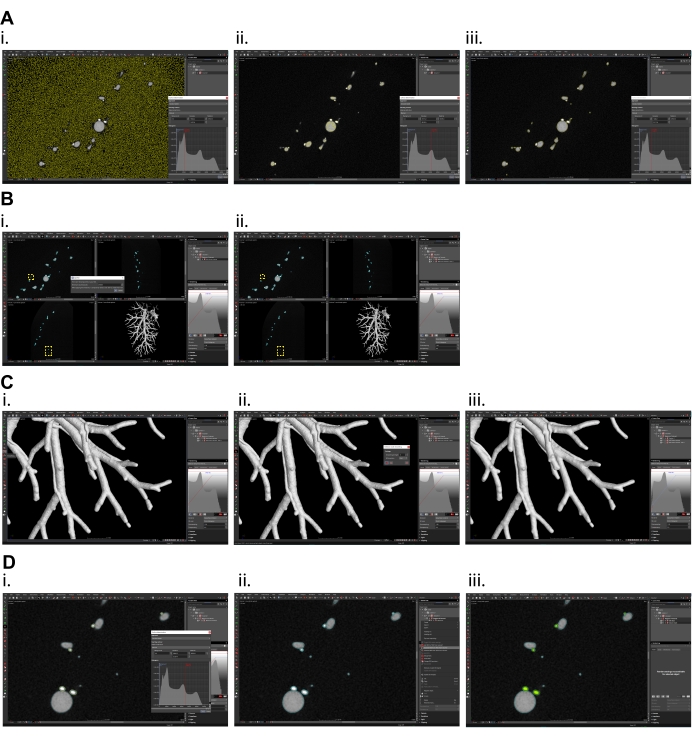
Figure 3: Micro CT data processing in volume graphics software. (A) Surface determination, (i) overestimated isovalue (current preview of selection is shown in yellow color), (ii) underestimated isovalue, (iii) optimal selection of isovalue for proper surface determination of portal vein and bile ducts. (B) Splitting region of interest (ROI) created by surface determination, (i) set the value in dialog window high enough that only one segment (the largest one) will remain, (ii) in yellow frames the smaller (excluded) particles are shown. (C) Surface smoothing of the data, (i) smoothing function is on the left panel, (ii) set the smoothing strength to 1 (max. 2) and create new smoothed ROI, (iii) smoothed data. (D) Separation of individual tubular systems, (i) in surface determination function set the isovalue so that only the biliary system is included in selection (current preview of selection is shown in yellow color), (ii) mark the ROI of both systems and ROI of only the biliary system and subtract biliary system ROI from ROI of both systems, (iii) Portal vein shown in grey, the biliary system shown in green. Please click here to view a larger version of this figure.
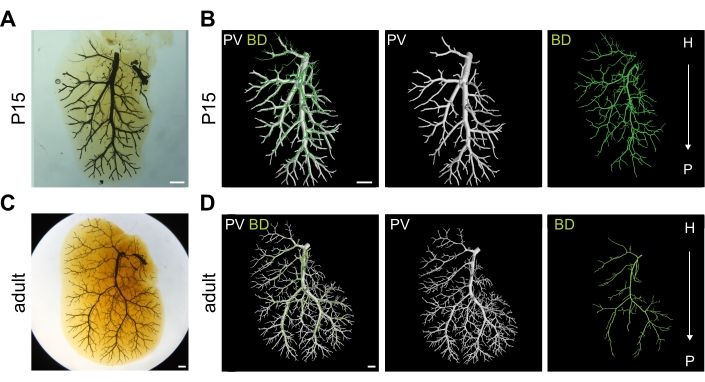
Figure 4: Well-injected bile duct (BD) and portal vein (PV) systems. (A) Optically cleared right medial lobe (RML) of postnatal day 15 (P15) liver injected with two resins into the two systems. Scale bar 1 mm. (B) 3D rendering of P15 RML shown in (A) depicting portal vein vasculature in white and biliary system in green. Scale bar 1 mm. (C) Optically cleared RML of adult liver injected with two resins into the two systems. Scale bar 1 mm. (D) 3D rendering of adult RML shown in (C) depicting portal vein vasculature in white and biliary system in green. H = hilar, P = peripheral. Scale bar 1 mm. Panels A, B, D are adapted with permission from Hankeova et al.9. Please click here to view a larger version of this figure.
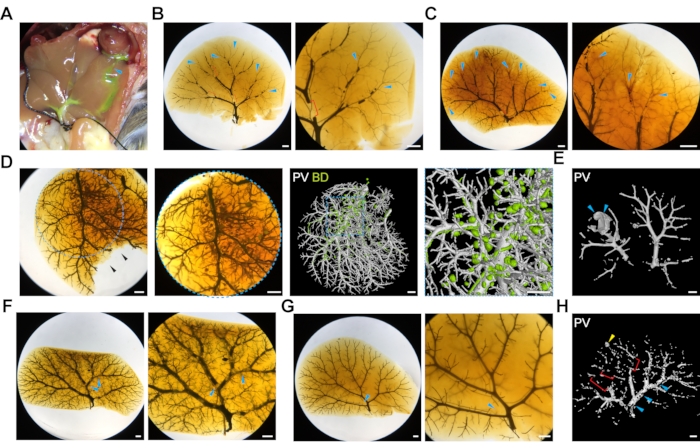
Figure 5: Common challenges of double resin liver injections. (A) The image depicts a liver that was accidentally nicked during the initial opening of the abdominal cavity, and the resin is leaking through the cut (blue arrowhead). (B) Poorly injected portal vein system due to resin hardening. Blue arrowheads label empty terminal branches, and red brackets label large bubbles. Scale bar 1 mm. (C) Poorly injected portal vein system due to poor transcardial perfusion. Blue arrowheads label blood visible in the terminal branches. Scale bar 1 mm. (D) Overfilled biliary system manifested by isolated balls of resin. The left panels show the optically cleared liver, and the right panels show the 3D microCT rendered image. The blue dotted outlines depict zoom-in regions. The black arrowheads label a part of the liver that was damaged during the optical clearing after microCT scanning. Scale bar 1 mm. (E) High pressure during resin injection can cause rupture of the portal vein (the animal in this panel carries a Jag1H268Q mutation), marked by blue arrowheads. Scale bar 1 mm. (F) Bubbles in the resin during portal vein injection (blue arrowheads) and (G) biliary system injection (blue arrowhead), scale bar 1 mm. (H) MicroCT scan of bubbles (blue arrowhead), poorly filled terminal branches (red brackets) and resin leakage (yellow arrowhead), scale bar 1 mm. Please click here to view a larger version of this figure.
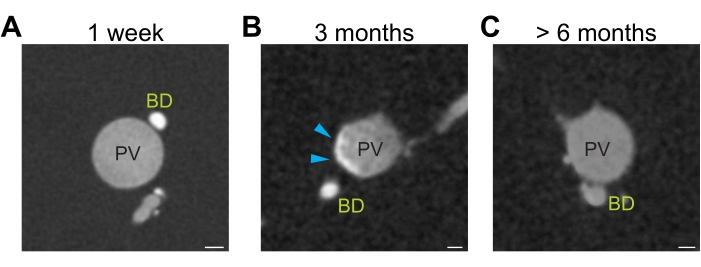
Figure 6: Differential resin contrast. (A) Freshly opened yellow resin generates sufficient contrast to distinguish resin injected portal vein (grey) and bile ducts (white). (B) Three months storage of yellow resin lead to precipitation of the resin resulting in heterogeneous opacity (grey-white portal vein, blue arrowhead). (C) Prolonged storage (>6 months) of yellow resin diminishes the contrast between the portal vein (grey) and bile ducts (grey). Scale bar 100 µm. Please click here to view a larger version of this figure.
