We present here a retrospective cross-sectional analysis (01/2018 to 05/2021) from 66 patients (37 males, 29 females) aged 9-68 years (mean 46.3y, SD ±13.4y), who underwent stapes surgery (48 standard surgeries, 18 revisions, Table 1 and Table 2). All patients were operated by the same surgeon (GM). The instruments were bent and black (Figure 3). The mean speculum size was 6.1 mm (range 5-8 mm, n = 51, Figure 2) which allowed an adequate visualization of the operating field. Only 1 out 66 cases needed a retroauricular incision (9 years old child with a canal diameter <5 mm). A posterior canaloplasty was necessary for 37 of 66 patients. Figure 2 illustrate how to hold the bent instruments with the first three fingertips while stabilizing the hand on the speculum or head of the patient with the remaining two fingers. A speculum holder consists of a mobile extension mounted on the operation table (Figure 4). Light exposure is limited and needs to be adjusted by the position of the microscope and the angled instruments (Figure 5). The ergonometric position of the sitting surgeon and optimized angle of the hands (Figure 6) allow a stable microsurgical performance. Fifty-eight patients received a Richards' piston prosthesis, one patient a Matrix Slim Line KURZ prosthesis, and five patients a malleo-vestibulo-pexy (MVP) prosthesis (ball joint prosthesis). The mean size of the prosthesis was 4.4 mm (range 4-5 mm, SD ± 0.2 mm), mean diameter was 0.46 mm (range 0.4-0.6 mm, SD ± 0.08 mm, Table 1). The prosthesis was additionally fixed with otologic cement in 33 of 66 cases. The Chorda tympani was preserved in 55 out of 65 cases.

Figure 1: Positioning of the patient. (A) The operation table at the lowest position tilted in the reverse Trendelenburg position. (B) The head/body rotation in a side-lying position towards the healthy ear. Please click here to view a larger version of this figure.
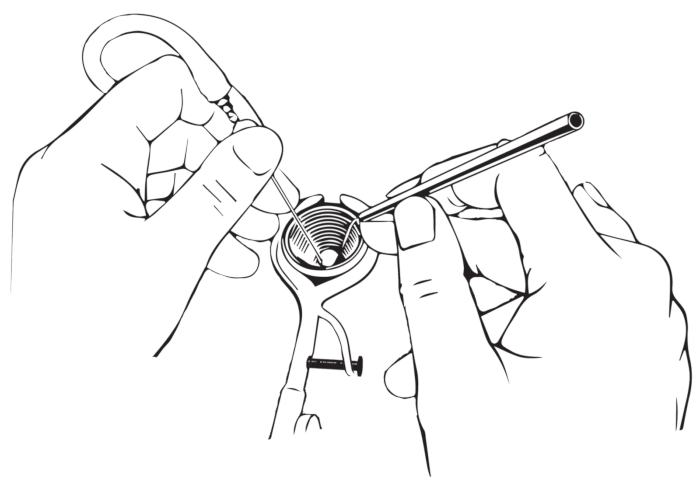
Figure 2: How to hold the instruments. The instruments must be held like a pencil; the ring finger should be supported at the edge of the speculum. Please click here to view a larger version of this figure.
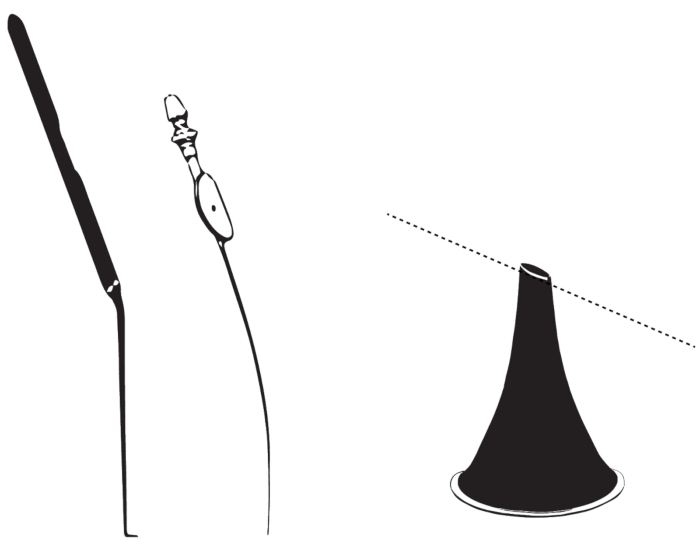
Figure 3: Bent instruments for transcanal microscopic approach. The figure illustrates bent instruments such as a hook, a suction, or an ear speculum (from left to right). Please click here to view a larger version of this figure.

Figure 4: Ear speculum holder. The figure illustrates the design of the speculum holder. Please click here to view a larger version of this figure.
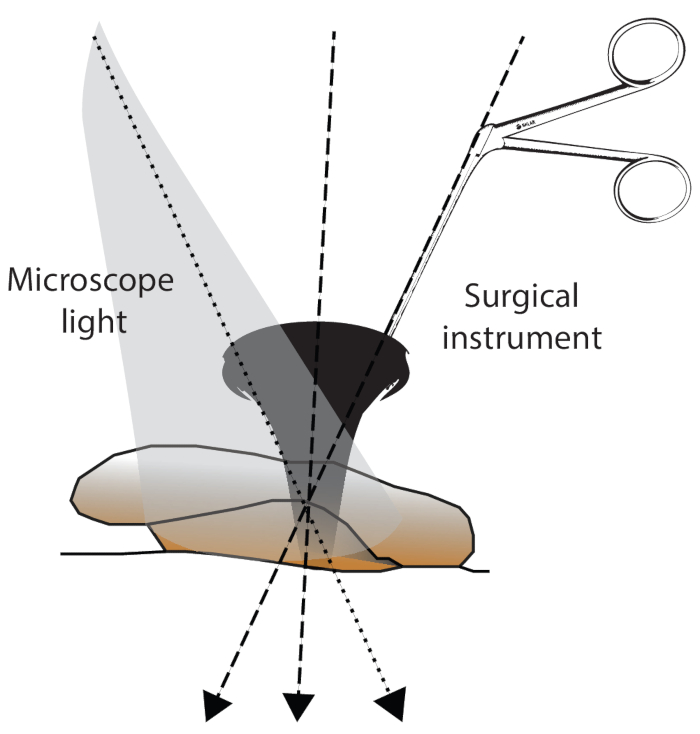
Figure 5: Surgical field exposure. The exposure of the surgical field can be influenced by 1) the angle of the microscope light, 2) the angle of the introduced instrument, and 3) the angle of the ear canal/head position. Please click here to view a larger version of this figure.
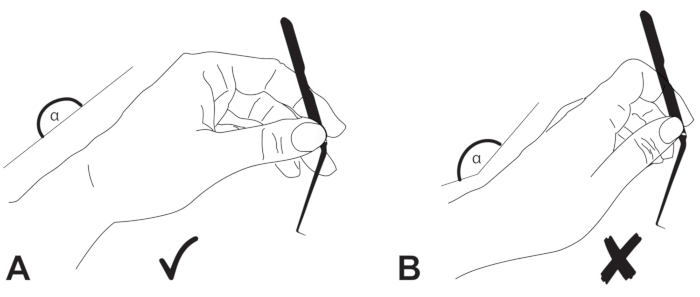
Figure 6: Positioning of the hands. The wrist of the surgeon should be in (A) neutral position and (B) not extended. Please click here to view a larger version of this figure.
Table 1: Summary of the study. The table summarizes the patient and operation characteristics Please click here to download this Table.
Table 2: Patient and operation characteristics. The table shows individual patient details and operation characteristics. Please click here to download this Table.
