The protocol describes simple and cost-effective solutions to real-life challenges affecting recruitment, compliance, and data quality in population studies employing wearable sensors. The steps described here allowed for the successful setup of a consumer wearable device for exposure and health monitoring in a large population study involving children with asthma and adults with atrial fibrillation. Figure 6 provides a graphical overview of the provided protocols and illustrates the key steps undertaken to address the main underlying issues identified.
Here, we present the representative results from a subset of 17 participants (asthmatic children aged 6-11 years old) who engaged in the LIFE MEDEA study in the spring of 202013. The 17 participants were equipped with a smartwatch that provided time-stamped data on physical activity (pedometer, accelerometer, heart rate) and GPS locations before and after the implementation of the protocol. These data were collected via the data collection application and were automatically synchronized with a cloud-based database when the smartwatch was in contact with the Wi-Fi network inside each participant's home, as described previously13. However, through the application of the described protocol, information on Wi-Fi connectivity, Wi-Fi signal strength, battery capacity, and whether the device was charging or not was also made available. The data on these additional variables were not automatically synchronized with the cloud-based database but had to be manually downloaded from each smartwatch via Bluetooth after the end of the study period. By comparing the data collected for a duration of 2 weeks before and 2 weeks after the protocol implementation, we evaluated the impact of these solutions in improving data completeness, defined as the percentage of time with collected data per day. Figure 7A presents the percentage of time with data before and after protocol implementation for each participant separately, while Figure 7B presents the corresponding distributions of the percentage of time with data for the whole group before and after the protocol implementation. Interestingly, the protocol implementation led to a statically significant increase in data completeness, with the percentage of time with data increasing from a median of 36.5% (min: 9.3%, max: 68.1%) to a median of 48.9% (IQR: 18.4%, 77.8%, p = 0.013).
Furthermore, in Figure 8, we present an extreme case of poor GPS data collected during 24 h from a single patient with AF participating in the study. Although the patient was wearing the watch as instructed, the actual raw GPS signal collected was scattered across the 24 h (Figure 8A), and the estimation of the duration of time indoors and the duration of time outdoors was difficult. The implementation of a GPS data filling algorithm (Supplementary Figure 1) allows for replacing missing data with estimated values (Figure 8B). Confirmation that the estimated time indoors and the estimated time outdoors were correct was provided by the logged smartwatch connectivity with the Wi-Fi network signal (Figure 8C). For the same patient, we also showcase another extreme case of a day with poor GPS data collected (Figure 9A). However, in this case, the implementation of the GPS data filling algorithm alone did not accurately estimate all the missing data. Characteristically, the algorithm correctly estimated that the participant was mostly out of their residence between approximately 09:00 to 21:00 that day and that they returned home for a brief period around 18:00, but it failed to capture that the participant also returned home for a period of about 90 min at approximately 13:30 (Figure 9B). Nevertheless, this event was not missed when the data on smartwatch connectivity with the Wi-Fi network signal were also considered (Figure 9C).
Finally, following successful piloting, the protocol was implemented across the full cohort of MEDEA participants during the spring of 2020 in both Cyprus and Greece (n = 108 asthmatic children). However, a few weeks after the smartwatches were distributed to the children and data collection began, the health authorities in Cyprus and Greece enforced a series of public health interventions of increasing intensity to control the COVID-19 pandemic in their respective countries. The public health interventions were initially characterized by social distancing measures and a ban on large public events but quickly escalated to strict national lockdowns during the months of March and April. Considering the unprecedented disturbances in the daily routine and behavior of the population, the decision was taken to continue tracking the location and activity of asthmatic children using the smartwatches during the duration of lockdowns to objectively quantify their compliance with the public health intervention measures and overall changes in physical activity. The data collected were used to calculate individual profiles of daily "fraction time spent at home" and "total steps/day" and were analyzed statistically to assess changes in these parameters over the escalating levels of the COVID-19 lockdown measures. The timeline and description of the escalating levels of the COVID-19 lockdown measures in the two countries are presented in Figure 10 and are described in detail by Kouis et al. in an earlier publication13. In summary, the results indicated a statistically significant mean increase in "fraction time spent at home" in both countries across the increasing intervention levels. The mean increase in "fraction time spent at home" was equal to 41.4% and 14.3% (at level 1), 48.7% and 23.1% (at level 2), and 45.2% and 32.0% (at level 3) for Cyprus and Greece, respectively. Physical activity in Cyprus and Greece demonstrated significant mean decreases of −2,531 and −1,191 steps/day (at level 1), −3,638 and −2,337 steps/day (at level 2), and −3,644 and −1,961 steps/day (at level 3)in Cyprus and Greece, respectively13. The weekly averages of "fraction time spent at home" and "total steps/day"in asthmatic children before COVID-19 and during the three levels of COVID-19 lockdown measures are displayed in Figure 1113.
DATA AVAILABILITY STATEMENT:
The anonymized dataset has been submitted to Figshare online open-access repository (https://doi.org/10.6084/m9.figshare.21601371.v3).
Table 1: Real-life challenges identified in relation to the use of smartwatch devices and the employed solutions. Please click here to download this Table.
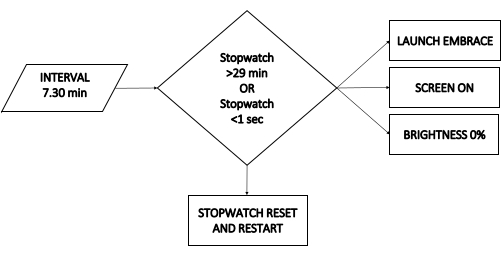
Figure 1: Activating the data collection application. Schematic diagram of the process to systematically activate the data collection application. The parallelogram denotes a trigger, the diamond denotes a condition, and the rectangle denotes an action. Please click here to view a larger version of this figure.

Figure 2: Enabling Wi-Fi connectivity. Schematic diagram of the process to systematically enable Wi-Fi connectivity. The parallelogram denotes a trigger, the diamond denotes a condition, and the rectangle denotes an action. Please click here to view a larger version of this figure.
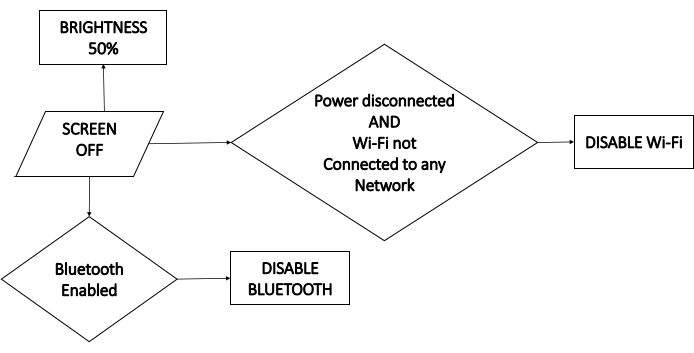
Figure 3: Optimizing battery consumption. Schematic diagram of the processes leading to actions that systematically optimize the battery consumption. The parallelogram denotes a trigger, the diamond denotes a condition, and the rectangle denotes an action. Please click here to view a larger version of this figure.
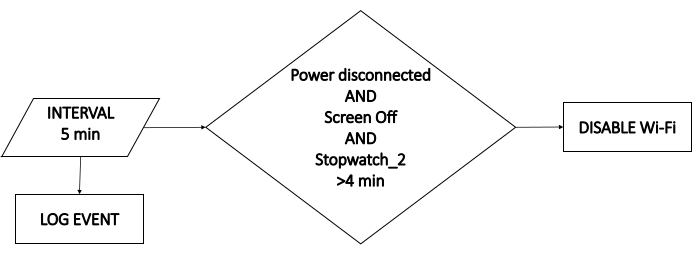
Figure 4: Logging event information. Schematic diagram of the processes that systematically log event information relevant to the project. The parallelogram denotes a trigger, the diamond denotes a condition, and the rectangle denotes an action. Please click here to view a larger version of this figure.
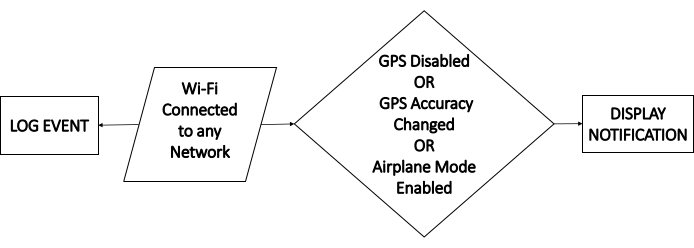
Figure 5: User notification if the GPS signal is disabled. Schematic diagram of the processes that systematically check the GPS signal status and provide notifications to alert users of problems. The parallelogram denotes a trigger, the diamond denotes a condition, and the rectangle denotes an action. Please click here to view a larger version of this figure.
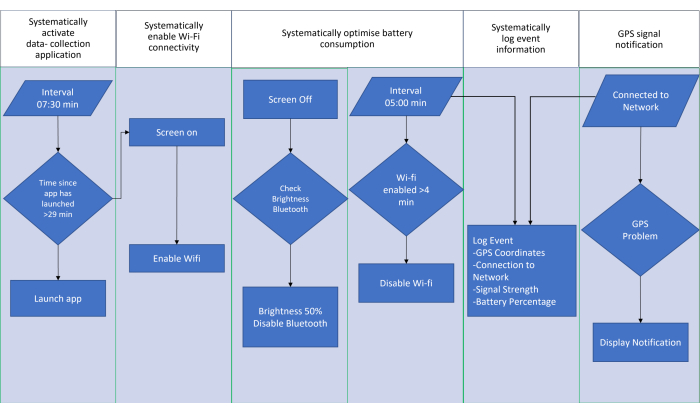
Figure 6: Schematic overview of the protocols. Schematic overview of the underlying challenges identified and the provided protocols with an illustration of the key steps in the processes. Please click here to view a larger version of this figure.
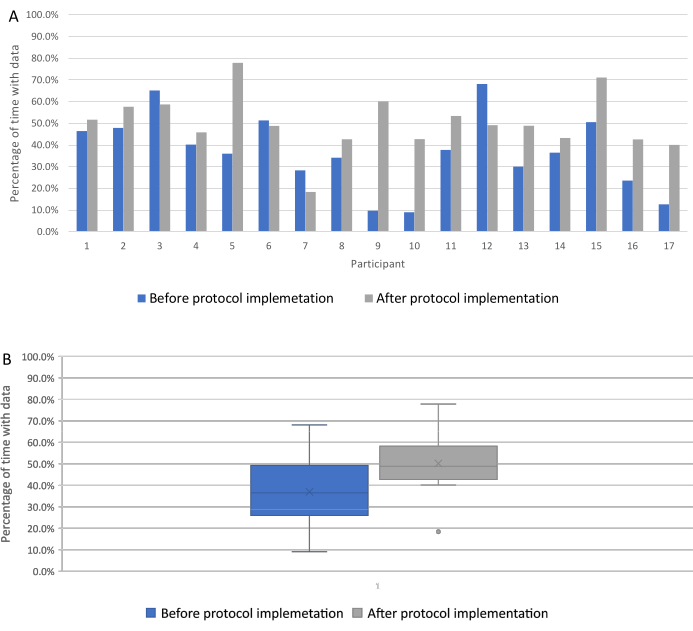
Figure 7: Data completeness before and after the implementation of the protocol. Data completeness for a representative group of participants (n = 17) for a period of 2 weeks before and after implementation of the protocol. (A) The percentage of time with data before and after the protocol implementation for each participant separately. (B) The corresponding distributions for the whole group. Please click here to view a larger version of this figure.
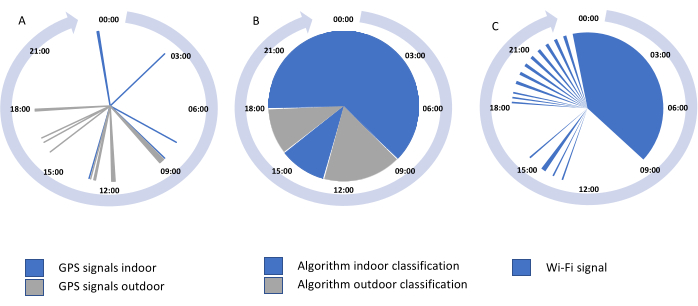
Figure 8: Implementation of the GPS data filling algorithm (extreme case 1). (A) Example case of a day with poor raw GPS signal data and (B) the implementation of the GPS data filling algorithm to replace the missing data with estimated values. (C) The confirmation of indoor and outdoor classifications based on the Wi-Fi received signal indicator. Please click here to view a larger version of this figure.
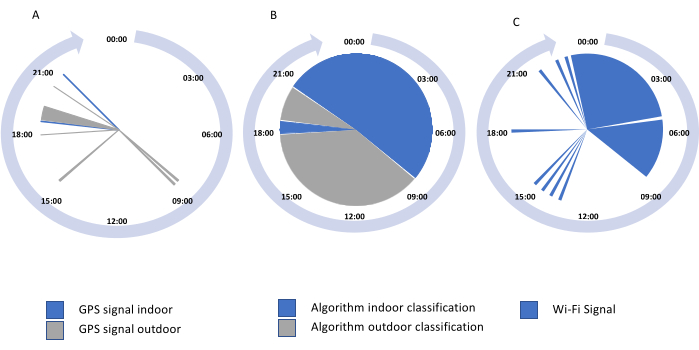
Figure 9: Implementation of GPS data filling algorithm (extreme case 2). (A) Example case of a day with poor raw GPS signal data and (B) the implementation of the GPS data filling algorithm to replace the missing data with estimated values. (C) The GPS data filling algorithm led to some indoor and outdoor misclassification, which was resolved using the Wi-Fi received signal indicator. Please click here to view a larger version of this figure.
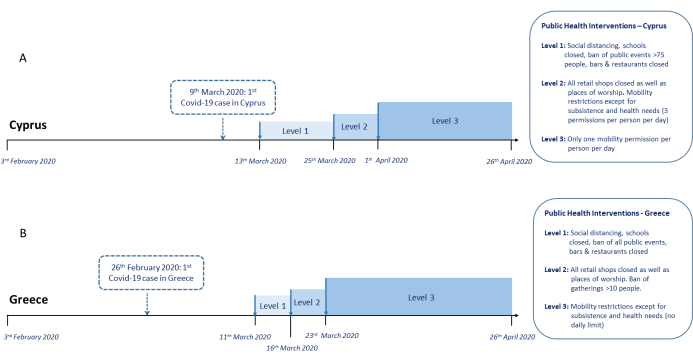
Figure 10: Timeline of public health interventions in Cyprus and Greece. Timeline of the study recordings in relation to the introduction of public health interventions in (A) Cyprus and (B) Greece during March and April 2020.The image is reproduced under license CC BY 4.0, without any changes, from the original study by Kouis et al., first published in Scientific Reports Journal13. Please click here to view a larger version of this figure.
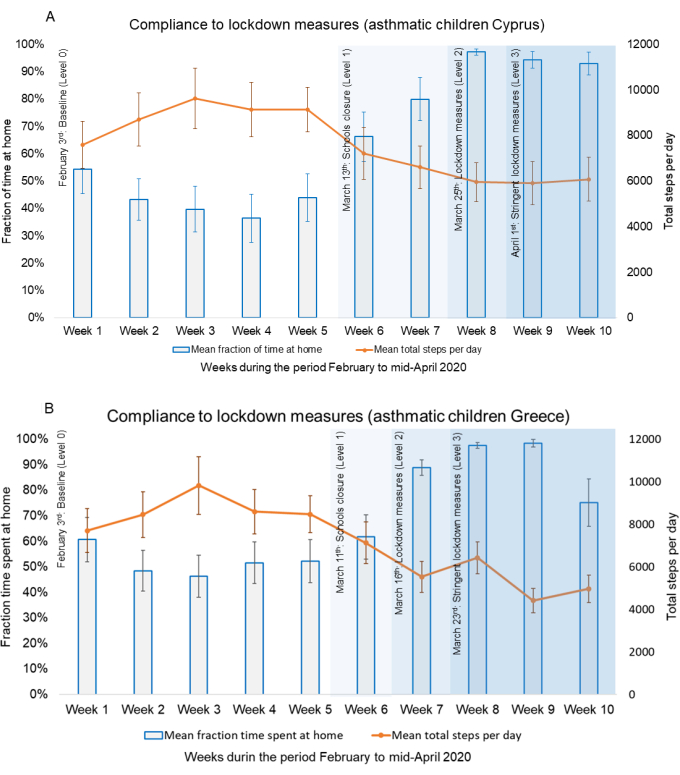
Figure 11: Changes in mobility in response to public health interventions among asthmatic children. Weekly averages of the fraction time spent at home and steps/day of asthmatic children before and during the three levels of public health interventions in (A) Cyprus and (B) Greece. The image is reproduced under license CC BY 4.0, without any changes, from the original study by Kouis et al., first published in Scientific Reports Journal13. Please click here to view a larger version of this figure.
Supplementary Figure 1: The implementation of a GPS data filling algorithm. Please click here to download this File.
Supplementary File 1: The macros described in this protocol. Please click here to download this File.
