We determined the range of detection for RT-qPCR probes and primers for synthetic nucleic acid content for both SARS-CoV-2 (N1) and Hs_RPP30 (P1). A 10-fold serial dilution of known concentrations of combined synthetic SARS-CoV-2 RNA and synthetic Hs_RPP30 DNA in water was done. The following formula was used to convert molecular weight to gene copy number
Gene copy number = (ng * 6.0221 x 1023)/((length in base pairs*660 g/mole) *1 x 109 ng/g)
and RT-qPCR was performed. After carrying out RT-qPCR, linear curves for N1 detection (Figure 4A) and P1 detection (Figure 4B) showed good correlation coefficients across a wide range of gene copy concentrations (R2= 0.9975 and R2= 0.9884, respectively). This result indicates that the combination of primer and probe sets is not inhibitory and can accurately detect SARS-CoV-2 RNA at one gene copy/µL (Cq=33). One gene copy is roughly equivalent to one viral copy; however, we did not determine quantitative viral copy numbers in saliva due to the semi-quantitative nature of RT-qPCR. We attempted to simulate positive saliva samples by spiking synthetic SARS-CoV-2 RNA of known concentrations into virus-free saliva (both heat-treated and non-heat treated) but were unable to produce N1 amplification at low concentrations of RNA (Data not shown). This might be due to RNase degradation or other confounding factors.
The inter-and intra-assay variability between automated and manual sample loading methods was also assessed. To evaluate inter-assay variability, 20 unique positive samples were loaded using the manual (described in section 8.1-8.3) and automated (described in section 7.1-7.11) methods. N1 Ct values were compared to determine if liquid handling robots and manual sample loading produced equivalent results (Figure 5A). The linear relationship between manual and automated methods produced a high correlation coefficient (R2= 0.9088), indicating that both methods are functionally equivalent. As N1 Ct values increased, variability of Ct values also increased. This trend is likely due to the heterogeneous distribution of viral particles within the saliva, which is more pronounced when fewer particles are present. To evaluate intra-assay variability, a comparison between the N1 Ct values from replicate wells of unique saliva samples using both methods of sample loading was done (Figure 5B). The linear relationship between replicates of automated sample loading (R2= 0.9622) produced a slightly higher correlation coefficient than that of manual loading (R2= 0.9589), indicating high reproducibility of SARS-CoV-2 detection for both loading methods.
Finally, an evaluation of saliva viscosity reduction with respect to the heat treatment methods was done (Figure 6). Saliva was obtained from a single source to eliminate sample variability. Greater variability in P1 Ct values within one heat treatment method may be indicative of higher sample viscosity as viscous saliva cannot be aspirated and dispensed precisely. Both 30 min and 60 min heat treatment methods produced significantly decreased sample variability when compared to no treatment control (p = 0.0006 and p = 0.0429, respectively). There was no significant difference between 30 min and 60 min treatments (p = 0.2245); therefore, the 30-min heat treatment method was implemented to reduce processing time.
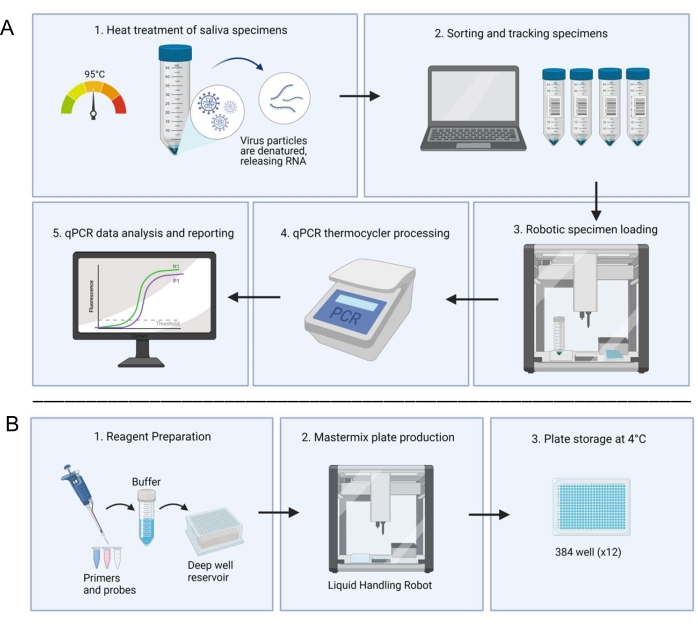
Figure 1: Laboratory workflow utilizing the saliva-based RT-qPCR diagnostic system. (A) Samples are collected and heat-treated at 95 °C for 30 min. Treated samples are sorted and tracked with patient information through an in-house spreadsheet system. A liquid handling robot loads samples into duplicate wells of prepared master mix plates. A technician manually loads the controls, seals the plate, and places the plate in a thermocycler for processing. Results are analyzed through an automated computer system and verified by a technician. (B) A technician prepares reagents for the master mix which are added to a deep well reservoir in a sterile biosafety cabinet. Filled deep well reservoirs are loaded into a dedicated liquid handling robot. Completed plates are sealed with foil, labeled, and stored at 4 °C. Please click here to view a larger version of this figure.
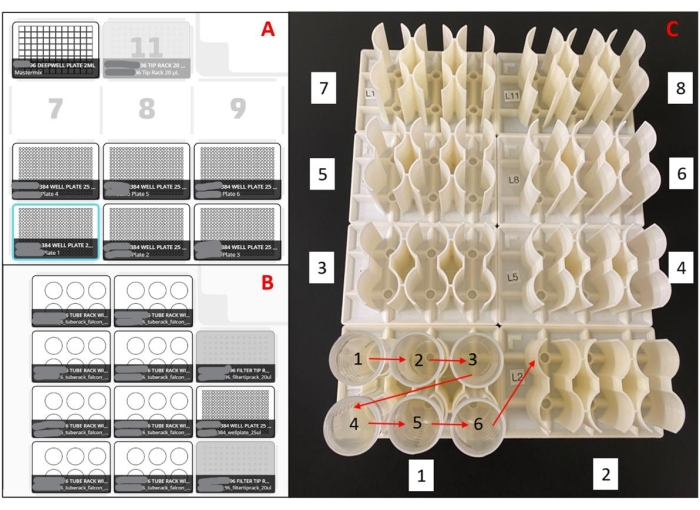
Figure 2: Layouts used for the liquid handling robot. (A) Deck layout for master mix plate preparation robot(s). With an eight-channel pipette, the robot is programmed to pick up pipette tips, aspirate master mix from a 96-well deep well reservoir, dispense master mix into empty 384-well plates, and eject the pipette tips into a waste bin. This is repeated for six plates per run. (B) Deck setup for sample loading robot(s). With a single-channel pipette, the robot is programmed to pick up a pipette tip, aspirate a saliva sample, dispense a saliva sample into duplicate wells of a 384-well master mix plate, and eject the pipette tip into a waste bin. This is repeated for 48 samples per run. (C) Sample tube loading order for 3D printed racks. Red arrows indicate loading order within a rack, and the white boxed numbers indicate the loading order of the entire set of racks. The entire setup will load 188 samples in duplicate into a 384-well plate. Please click here to view a larger version of this figure.
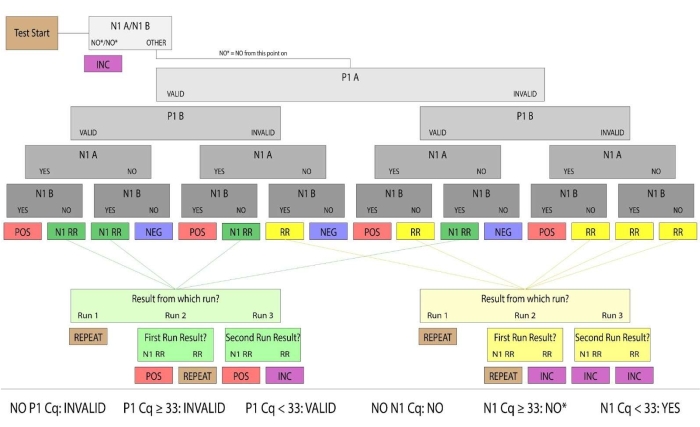
Figure 3: Sample resulting flowchart. Samples with valid P1 and positive N1 were determined to be human saliva samples positive for SARS-CoV-2. Valid and positive/negative sample results were considered conclusive. Samples that did not produce conclusive results in the first run were categorized as Rerun (denoted RR) or N1 Rerun (denoted N1 RR). Rerun samples had no valid P1 amplification, and N1 Rerun samples had positive N1 amplification in a single replicate. If no valid P1 amplification could be produced by a subsequent manual run, or both replicates had N1 Ct values above the positive threshold (Ct >33), the sample results were considered inconclusive. For clinical purposes, patient samples that did not arrive at the lab, had an insufficient quantity of saliva to pipette or were damaged were considered invalid. Please click here to view a larger version of this figure.
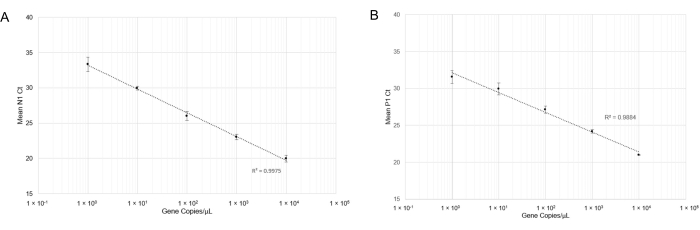
Figure 4: RT-qPCR detection of N1 (SARS-CoV-2) synthetic RNA and P1 (Hs_RPP30) synthetic DNA. Standard curves were plotted with standard deviations to determine the range of accurate detection using this probe/primer combination. (A) The mean Ct values (n =4) obtained in respective dilutions were plotted against the estimated quantity of synthetic RNA (1×100 to 1×104 RNA copies in 10 µL of RT-qPCR reaction). (B) The mean Ct values (n =3) obtained in respective dilutions were plotted against the estimated quantity of synthetic DNA (1 x 100 to 1 x 104 gene copies in 10 µL of RT-qPCR reaction). Please click here to view a larger version of this figure.
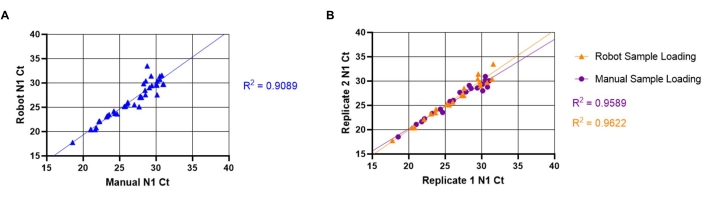
Figure 5: Comparison between manual and automated saliva transfer SARS-CoV-2 (N1) Ct values. The known SARS-CoV-2 positive saliva samples (n =20) were loaded in duplicate into an RT-qPCR master mix plate by a liquid handling robot. The samples have a Ct value ranging from 18-32 for N1. The same samples were then manually loaded into duplicate wells in a different plate location. (A) N1 Ct values obtained from unique samples using both the robot and manual sample loading were transposed to determine inter-assay variability between manual and robot loading. (B) Intra-assay variability was also determined by using transposed replicate of N1 Ct values obtained from both robot and manual sample loading. Please click here to view a larger version of this figure.
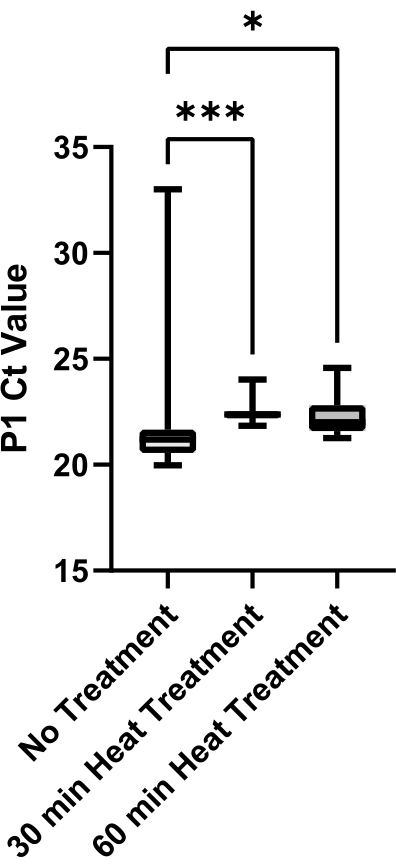
Figure 6: Evaluation of heat treatment methods for viscosity reduction in saliva. SARS-CoV-2 negative saliva was collected from a single source and aliquots were heat-treated for either 0 min, 30 min, or 60 min at 95 °C. P1 Ct values from technical replicates (n =12) of each condition were plotted to determine variability between treatment methods. Pairwise comparisons between groups were evaluated with an unpaired t-test (*** indicates p <0.001, * indicates p <0.05). Please click here to view a larger version of this figure.
Supplemental Figure 1: Comparison of N1 Ct in low P1 Ct saliva samples. The positive samples with low P1 Ct were selected and compared with the N1 Ct (n =106). The N1 Ct values ranged from 14-33, indicating the assay has a dynamic range in saliva samples that is comparable to the standard curve. Please click here to download this File.
| Component | Sequence (5’→3’) | Stock Concentration | Volume | ||
| 2019-nCoV-N1 Probe | /5FAM/ACCCCGCAT/ZEN/TACGTTTGGTGGACC/3IABkFQ | 50 µM | 500 µL | ||
| 2019-nCoV-N1-For | GACCCCAAAATCAGCGAAAT | 100 µM | 2000 µL | ||
| 2019-nCoV-N1-Rev | TCTGGTTACTGCCAGTTGAATCTG | 100 µM | 2000 µL | ||
| Hs RPP30 Cy5 Probe | /5Cy5/TTCTGACCT/ZEN/GAAGGCTCTGCGCG/3IABkFQ | 50 µM | 500 µL | ||
| Hs-RPP30-For | AGATTTGGACCTGCGAGCG | 100 µM | 2000 µL | ||
| Hs-RPP30-Rev | GAGCGGCTGTCTCCACAAGT | 100 µM | 2000 µL | ||
| Water | – | – | 11000 µL | ||
Table 1: Components of N1+P1 probe/primer mix.
| Component | Stock Concentration | Volume per reaction | Final Concentration | Batch Volume | ||
| Luna WarmStart RT Enzyme Mix | 20X | 0.5 μL | 1X | 3 mL | ||
| Luna Buffer Reaction Mix | 2X | 5.0 μL | 1X | 30 mL | ||
| N1+P1 Primer/Probe Mix | nCoV N1 F: 10 μM | 0.5 μL | 500 nM | 3 mL | ||
| nCoV N1 R: 10 μM | 500 nM | |||||
| Probe nCoV N1: 2.5 μM | 125 nM | |||||
| RPP_30 P1 F: 10 μM | 500 nM | |||||
| RPP_30 P1 R: 10 μM | 500 nM | |||||
| Probe RPP_30 P1: 2.5 μM | 125 nM | |||||
| Nuclease Free Water | — | 2 μL | — | 12 mL | ||
| Subtotal | — | 8 μL | — | 48 mL | ||
| Template | 2 μL | |||||
Table 2: Components of multiplex SARS-CoV-2 master mix.
| Stage | Temperature (°C) | Duration | Number of Cycles |
| Reverse Transcription | 55 | 10 min | 1 |
| Initial Denaturation | 95 | 1 min | 1 |
| Touchdown | 95 | 10 sec | 3 |
| 72 | 30 sec | ||
| 95 | 10 sec | 3 | |
| 69 | 30 sec | ||
| 95 | 10 sec | 3 | |
| 66 | 30 sec | ||
| Main Amplification | 95 | 10 sec | 40 |
| 65 | 30 sec |
Table 3: Touchdown RT-qPCR protocol. Thermocycling conditions for one-step RT-qPCR SARS-CoV-2 diagnostic assay.
| Touchdown Step | No Touchdown Step | |||
| Mean N1 Ct | Mean P1 Ct | Mean N1 Ct | Mean P1 Ct | |
| Sample 1 | 19.65 | 22.7 | 27.8 | 28.3 |
| Sample 2 | 22.24 | 24.9 | 28.77 | 30.5 |
| Sample 3 | 18.85 | 19.2 | 24.65 | 25.9 |
| Sample 4 | 25.56 | 22.8 | 31.93 | 29.2 |
| Sample 5 | 22.34 | 24.8 | 38.48 | 40.0 (Failed detection) |
Table 4: Comparison of touchdown Ct values for five positive samples against no touchdown Ct values.
| Sample | TigerSaliva | Commercially available saliva-based SARS-CoV-2 assay | ||
| N1 Ct | P1 Ct | Covid-19 Value | RNaseP Value | |
| D11 | 16.4 | 18.1 | 20.86 | 23.4 |
| E11 | 18.9 | 19.1 | 25.6 | 21.2 |
| F11 | 19.5 | 18.4 | 22.8 | 22.2 |
| G11 | 22.2 | 19.1 | 23.7 | 22.9 |
| H11 | 26.4 | 21.3 | 32.2 | 26.7 |
| A12 | 14.8 | 16.5 | 29.15 | 19 |
| B12 | 24 | 19.6 | 31.05 | 21.35 |
| C12 | 14.9 | 17.5 | 20.84 | 18.9 |
Table 5: Comparison of TigerSaliva Ct results and commercially available saliva-based SARS-CoV-2 assay results. Both assays were performed on the same saliva samples (n =8).
Supplemental File 1: Custom script for robot master mix plate creation. Please click here to download this File.
Supplemental File 2: Custom script for saliva processing on sample loading robots. Please click here to download this File.
Supplemental File 3: Instructions for self-collection of high-quality saliva samples from participants. Further details can be found in the short video description of the testing process available at https://www.clemson.edu/centers-institutes/reddilab/index.html. Please click here to download this File.
Supplemental File 4: Sample intake spreadsheet. Please click here to download this File.
Supplemental File 5: Sample loading spreadsheet. Please click here to download this File.
Supplemental File 6: Sample 384-well plate layout diagram. Please click here to download this File.
