Robotic Taj Mahal Hepatectomy for Hilar Cholangiocarcinoma
Summary
Robotic resection of hepatic S4b, S5, and S1 using the Taj Mahal procedure is feasible and safe for selected patients with hilar cholangiocarcinoma. The step-by-step details for this surgery are presented here.
Abstract
Hilar cholangiocarcinoma is the most common malignant tumor of the biliary tract. Radical surgical resection is the only effective treatment option. In this study, a 32-year-old male patient with Bismuth Type IVa hilar cholangiocarcinoma underwent radical robotic resection of hepatic S4b, S5, and S1 (Taj Mahal hepatectomy) combined with regional lymphadenectomy, hilar bile duct reconstruction, and hepaticojejunostomy by the robotic surgical system. Postoperative pathological examination showed moderately-differentiated adenocarcinoma of the hilar bile duct. The surgical margins of the liver and bile ducts were negative. Recovery was smooth and the patient was discharged on the 17th postoperative day. The robotic surgical system and associated multiple instruments along with flexible and precise movements is suitable for the local hepatectomy around the porta hepatis, and delicate reconstruction of the hilar bile duct with a smaller diameter. This first clinical application study found that robotic Taj Mahal hepatectomy for hilar cholangiocarcinoma is safe and feasible and needs more experience for the evaluation of its long-term outcomes.
Introduction
Hilar cholangiocarcinoma is a type of malignant tumor that is typically resistant to radiotherapy and chemotherapy1. Most patients with hilar cholangiocarcinoma can only survive 1 year after the diagnosis. Surgical resection is the only effective treatment for hilar cholangiocarcinoma2. Recently, several approaches have been proposed for the treatment of hilar cholangiocarcinoma3.
The Taj Mahal procedure comprises complete resection of S4b, S5, and S1 combined with regional lymphadenectomy, extrahepatic bile duct resection, hilar bile duct reconstruction, and hepaticojejunostomy4. Different from conventional hilar cholangiocarcinoma radical resection, the Taj Mahal procedure does not require a large-scale liver resection such as hemihepatectomy, thus preserving the maximum residual liver volume for patients, which greatly improves patient's tolerance to the surgery and may reduce the incidence of postoperative complications. However, the Taj Mahal procedure is technically demanding and has not been widely applied. The robotic surgical system provides multiple instruments and has many advantages over laparoscopic surgery, which could make the dissection and suturing more precise. The protocol herein presents a robotic hepatic S4b, S5, and S1 resection using the Taj Mahal procedure for Bismuth type IVa hilar cholangiocarcinoma5.
Indications
Patients with Bismuth type II, III, and selected type IV hilar cholangiocarcinoma wherein the bilateral hepatic artery and portal vein are not widely invaded, especially those with liver function impairment require treatment via hemihepatectomy2,3,4,6.
Contraindication
Tumor massively invades the hepatic artery or portal vein and needs resection and reconstruction of vessels by preoperative imaging and intraoperativeassessment. The upper extent of the tumor far exceeds the U Point defined as the bend between the transverse portion and the umbilical portion of the left portal vein or P point defined as the bifurcation of the anterior branch and the posterior branch of the right portal vein7.
Case presentation
A 32-year-old Chinese man presented with jaundice and tea-colored urine. The patient had a 10-year history of heavy drinking and smoking. Laboratory examinations revealed elevated CA19-9 (31.48 U/mL) and total bilirubin (145.7 μmol/L). Severe obstruction with partial thickening of the hilar bile duct wall was observed in Magnetic Resonance Cholangiopancreatography (MRCP) (Figure 1) and 3D reconstruction of MRI (Figure 2). The patient was diagnosed with Bismuth IV4a hilar cholangiocarcinoma. Vascular invasion in the porta hepatis was not seen in the preoperative evaluation and intraoperative observation. A multidisciplinary team decided to perform radical resection using a robotic Taj Mahal procedure.
Protocol
The patient provided written informed consent for the operation and use of medical data for scientific purposes. This research was performed in compliance with the Declarations of Helsinki and was approved by the local institution's human research ethics committee and institutional review board.
1. Operative setting and trocar placement
- After satisfactory anesthesia, place the patient in a supine, 30° reverse Trendelenburg position and spread the legs apart. Perform the sterilized exposition and check the instrument availability.
- Ensure that the first surgeon stays in front of the robot console and the table-side surgeon stands between the patient's legs. Ensure the availability of the robotic system and robotic instruments (Table of Materials).
- Establish pneumoperitoneum through a 1 cm incision above the umbilicus using a Veress needle connected to the insufflator (set the pressure to 14 mmHg). Remove the Veress needle, transfer the insufflation tube to a 12 mm trocar, and then insert the trocar as a temporary camera port.
- Insert the robotic endoscope through the camera port and perform a diagnostic laparoscopy (the robotic endoscope is held by the assistant surgeon) to confirm adhesion status, exclude peritoneum metastasis, and evaluate operative feasibility. Subsequently, insert the remaining four trocars as follows, under the visual guidance of the endoscope.
- Place 8 mm trocars in the right and left anterior axillary lines (AALs) under the costal margin, for the second (bipolar forceps) and third (Cadiere forceps) robotic arms, respectively.
- Place a 12 mm trocar 5 cm to the umbilicus in the right lateral position as the camera port.
- Place an 8 mm trocar 8 cm to the umbilicus at the superior left lateral position for the first (electrocoagulation hook) robotic arm.
- Place a 12 mm trocar right to the umbilicus in the right midclavicular line as the camera port. The assistant port is the original temporary camera port (step 1.3) (Figure 3).
NOTE: The location of the ports can be adjusted according to the lesion's location and the patient's body figure.
2. Abdominal inspection and assessment of resectability
- Perform a full abdominal inspection using robotic endoscopy to observe the shape and size of the liver, gallbladder, and hepatoduodenal ligament, assessing for tumor resectability. Advance the endoscope into the abdominal cavity to rule out tumor metastasis.
- Dissect the lesser omentum from right to left with an electrocoagulation hook to descend the pylorus and duodenum. Create a Kocher's incision, about 5 cm, at the lateral side of the second part of the duodenum using an electrocoagulation hook to expose the retroduodenal portion of the common bile duct.
- Clip the distal and proximal stump of the common bile duct with an absorbable ligating clip.
- Transect the common bile duct in the superior edge of the pancreas using curved shears. Sample the tissue from the largest margin of the distal stump of the common bile duct and send it for frozen section pathological examination.
- Dissect the common bile duct and hepatic duct from caudal to cephalad direction, toward the cystic triangle. Confirm the presence of the cystic duct and artery. Dissect the cystic triangle using an electrocoagulation hook and determine the relationship between tumor and hepatic artery as well as portal vein.
NOTE: The cystic triangle is constituted by the common hepatic duct, cystic duct, and cystic artery. - After ligation with an absorbable ligating clip, transect the cystic duct and artery using curved shears, and then remove them and the gallbladder from the gallbladder bed.
- Dissect the hepatic artery and portal vein using the intraglissonian approach8 with an electrocoagulation hook and bipolar forceps. Identify the position of the gastroduodenal artery, common hepatic artery, and portal vein, and fasten them with a rubber band.
NOTE: The intraglissonian approach is used to dissociate the whole bundle of the left, middle, and right Glissonean pedicles beyond the hilar plate, and based on this, dissect the Glissonean pedicles, hepatic artery, and portal vein, respectively. Thereafter, a regular and precise hepatectomy is performed according to the ischemia line after selective hepatic flow occlusion. - Skeletonize arteries and veins in the hilar region using an electrocoagulation hook and bipolar forceps.
- Dissect the hepatoduodenal ligament and transect the common bile duct from bottom to top. Dissect the bile duct, proper hepatic artery, and portal vein completely with an electrocoagulation hook and bipolar forceps. Transect their branches with an ultrasonic scalpel to expose arteries and veins one by one.
- Resect the 8a, 8p, and 12 lymph nodes, peripheral nerve connective tissue, and hepatic portal plate with the electrocoagulation hook. Finally, remove fibrous connective tissue and lymph nodes along the duct.
- Mobilize the left and right portal veins and tie a rubber band around the left portal vein. Transect the branches of the portal vein from the right caudate lobe using an ultrasonic scalpel.
3. Taj Mahal hepatectomy and regional lymphadenectomy
- Label the resection line of S4b, S5, and the caudate lobe on the liver's surface using an electrocoagulation hook. Transect the perihepatic ligaments and dissociate the bilateral halves of the liver with the electrocoagulation hook and bipolar forceps.
- Expand the Kocher's incision using an ultrasonic scalpel and an electrocoagulation hook. Resect lymph nodes 13a, 16a2, and part of the 7 and 9 groups using an ultrasonic scalpel and bipolar forceps. Remove these lymph nodes together with the previously dissected lymph nodes (8a, 8p, and 12) to achieve en bloc regional lymphadenectomy, which could also improve the exposure of the left caudate lobe.
- Transect the hepatic round ligament and its falciform ligaments using an electrocoagulation hook and bipolar forceps. Correct the resection line in order to expose intrahepatic bile ducts sufficiently, according to the actual situation during surgery.
- Occlude the left Glissonean pedicle with bulldog clamps and transect the left liver parenchyma (S4b) along the resection line with an ultrasonic scalpel. Similarly, occlude the right Glissonean pedicle and transect the right liver parenchyma (S5).
- Ligate the branches of the intrahepatic Glissonean system and hepatic veins using surgical clips and use an ultrasonic scalpel for parenchymal transection. Completely resect S4b and S5.
NOTE: To occlude the left and right Glissonean pedicles, use the intraglissonian approach before this process. - Transect the liver parenchyma of the caudate lobe and the Spiegel lobe. Finally, transect the ventral caudal portion of S1.
4. Reconstruction of the intrahepatic bile ducts and bilateral hepaticojejunostomy
- Examine the cut surface of the liver and close the bile duct orifice of the caudate lobe with 4-0 sutures. Use a electrocoagulation hook (spray coagulation model, effect 3, 80 W) to stop small bleeds and bile leakage, while using a 4-0 suture to stop larger bleeds and bile leakage.
- Insert silicon stents into the branches of the left and right hepatic ducts to confirm the location of the ducts. Remove the stents and suture the adjacent walls of the right hepatic duct branches (B5d/7/8+6) and the left hepatic duct branches (B2-4) with 4-0 sutures. When the adjacent branches are sufficiently close, reconstruct the adjacent hepatic duct branches into an arch with a septum using a CV-4 suture (Figure 4A). Close the remaining small bile duct orifice with 4-0 sutures. Cover the cut surface of the liver with a hemostatic sponge.
- Open the gastrocolic ligament with an electrocoagulation hook and ultrasonic scalpel. Open the avascular area on the left of vessels of the middle colic artery to expose the jejunum. Retract the proximal jejunum through the transverse mesocolon.
- Perform retrocolic hepaticojejunostomy about 20 cm away from the ligament of Treitz for the left hepatic duct (B2-4) using a CV-4 suture in the hypotonic position of the jejunum. Using the same method, perform the hepaticojejunostomy for the right hepatic duct (b5d/7/8+6) and jejunum, and finish the bilateral hepaticojejunostomy (Figure 4).
NOTE: Before the hepaticojejunostomy, suitably mobilize the bile duct stumps for anastomosis. The 5-0 absorbable suture is preferred for hepaticojejunostomy, while the non-absorbable suture, such as the size CV-4 ePTFE monofilament suture is preferred for a wider anastomosis site. - Transect the jejunum and jejunal mesentery using a cutting stapler away from the proximal stump of the biliary-enteric anastomosis. Perform a side-to-side jejuno-jejunostomy with the cutting stapler about 45 cm away from the distal stump of the biliary-enteric anastomosis.
NOTE: To reduce the tension of hepaticojejunostomy, the key is the preparation of a tension-free jejunum loop. Transect 1-2 branches of jejunal artery, if necessary. Put two suspension sutures at both sides of the hepaticojejunostomy to further reduce the tension caused by gravity and intestinal motility.
5. Drain placement
- Examine the cut surface of the liver and anastomosis sites. Eliminate bleeding and bile leakage as described in step 4.1.
- Place two drainage tubes at the anterior and posterior areas of the biliary-enteric anastomosis, respectively.
6. Postoperative care
- Remove the nasogastric tube the day after the operation. Start an abrosia and expand to a normal diet in 3 days.
- Assess serum total bilirubin on postoperative day 1, day 3, day 7, and day 12. Perform a CT of the abdomen if total bilirubin on day four is elevated compared to day three.
- Assess drain bilirubin on postoperative day 1 to day 3. Remove the drain when drain bilirubin levels are less than three times the upper limit of normal serum amylase.
- Perform abdominal CT, blood routine examination, and blood biochemistry examination to assess postoperative recovery before discharge.
Representative Results
The operation was eventually completed with trimming of the hepatic ducts (Figure 4A) and the anastomosis of the bilateral hepaticojejunostomy (Figure 4B). The total operative time was 340 min with an estimated blood loss of 100 mL (Table 1). The enhanced recovery after surgery (ERAS) pathway of the People's Liberation Army (PLA) General Hospital was used during the postoperative recovery period in the surgical ward. Total bilirubin was measured on postoperative days (PODs) 1 (157.5 μmol/L), 3 (162.3 μmol/L), 7 (127.6 μmol/L), and 12 (45.9 μmol/L) to assess recovery. The drain was removed, and the patient was discharged on POD 17.
A pathological analysis of the specimen revealed a moderately-differentiated cholangiocarcinoma (IVa, T3N2M0, AJCC 8th edition)5. The surgical margins of the liver and bile ducts were negative. Immunohistochemical staining was positive for CA19-9, CD10, CDX-2, CEA, CK19, CK7, E-cadherin, EMA, muc-1, MUC-5AC, P53, MLH1, MSH2, MSH6, PMS2, and HER-2, and was negative for CD34, CK20, Syn, muc-2, and muc-5AC. The patient had no laboratory and radiological evidence of recurrence or metastasis 3 months postoperatively (Figure 5).
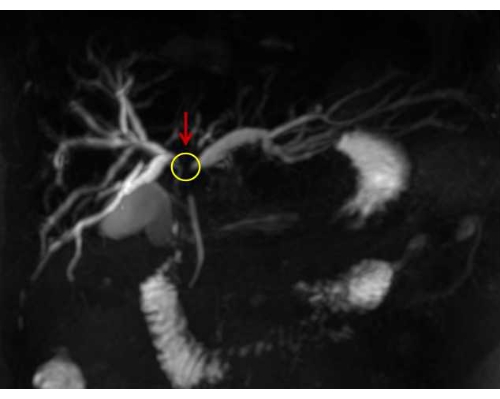
Figure 1: MRCP scan showing the obstruction in the hilar bile duct. The yellow circle indicates the site of cholangiocarcinoma. Please click here to view a larger version of this figure.
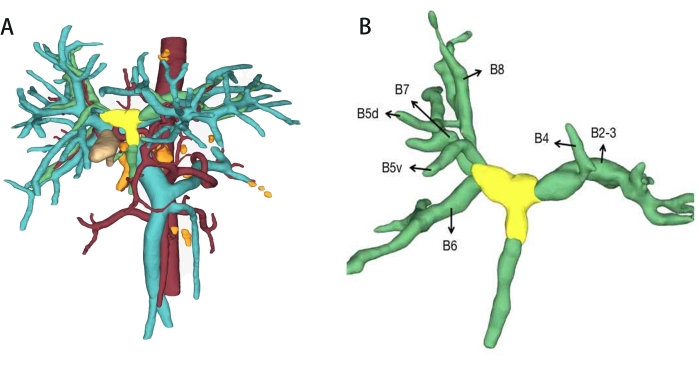
Figure 2: 3D reconstruction of MRI. (A) 3D reconstruction model of the lesion, hilar bile duct, and vessels.Red tubes are arteries, blue tubes are portal veins, green tubes are bile ducts, yellow regions are hilar cholangiocarcinoma, and orange regions are swollen lymph nodes. (B) 3D reconstruction model of the hilar bile duct. B2-B8: Each branch of the intrahepatic bile duct. Please click here to view a larger version of this figure.
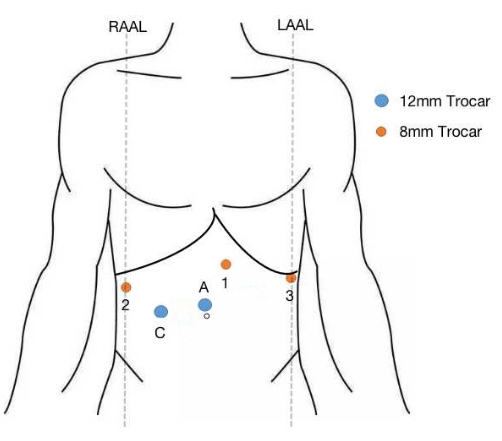
Figure 3: Trocar placement. Five trocars were used. 1: port for the first robotic arm; 2: port for the second robotic arm; 3: port for the third robotic arm; C: camera port; A: assistant port; red circle: 8 mm trocar; blue circle: 12 mm trocar; RAAL: right middle axillary line; LAAL: left anterior axillary line. Please click here to view a larger version of this figure.
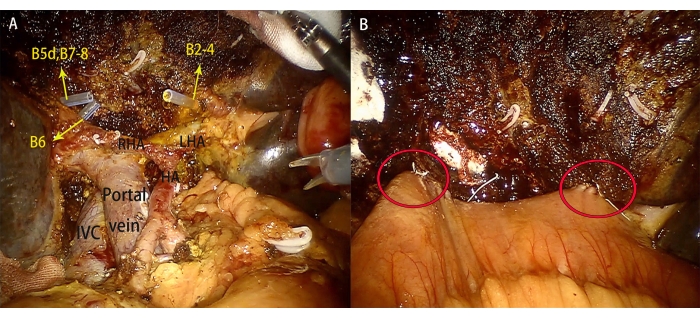
Figure 4: Taj Mahal hepatectomy and bilateral hepaticojejunostomy. (A) Identification of the stumps of the intrahepatic bile duct. B: bile, RHA: right hepatic artery, LHA: left hepatic artery, HA: hepatic artery IVC: inferior vena cava (B) The red circles indicate the sites of the hepaticojejunostomy of the right and left intrahepatic bile ducts. Please click here to view a larger version of this figure.
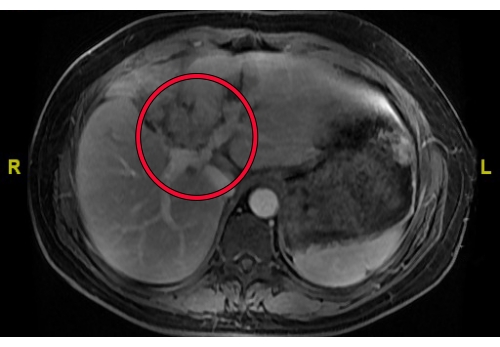
Figure 5: MRI of the patient obtained 3 months postoperatively. The red circle indicates the area of the operative region; changes after Taj Mahal hepatectomy for hilar cholangiocarcinoma; mild dilatation of intrahepatic bile duct; liver regeneration without tumor recurrence. Please click here to view a larger version of this figure.
| Variable | Outcome |
| Intraoperative | |
| Operative time, minutes | 340 |
| Intraoperative blood loss, mL | 100 |
| Postoperative | |
| Drain removal, days | 17 |
| Postoperative hospital stay, days | 17 |
| Pathological diagnosis | moderately-differentiated cholangiocarcinoma, 2.0cm |
| Positive markers | CA19-9, CD10, CDX-2, CEA, CK19, CK7, E-cadherin, EMA, muc-1, MUC-5AC, P53, MLH1, MSH2, MSH6, PMS2, HER-2 |
| Negative markers | CD34, CK20, Syn, muc-2, muc-5AC |
Table 1: Representative results of surgery.
Discussion
Because the left hepatic duct is longer and less prone to anatomic variation than the right, the residual left hepatic duct after right hepatectomy has a decreased risk of a positive margin9. For hilar cholangiocarcinoma, a right hepatectomy is typically performed due to its anatomical advantages over a left hepatectomy However, increased complications and mortality rate of large-scale hepatectomy restrict the application of hemihepatectomy in hilar cholangiocarcinoma patients with poor liver function.
To preserve maximum liver parenchyma in patients with hilar cholangiocarcinoma, resection of the S4b, S5, and S1 (Taj Mahal hepatectomy) could be applied. Compared to the conventional operation, the Taj Mahal procedure significantly reduces the damage to normal liver tissue, preserves more normal liver tissue, and reduces the occurrence of serious postoperative complications, such as acute liver failure. More importantly, it follows the principle of radical tumor resection and can obtain a higher resection margin within P point or U point, thus ensuring the negative rate of longitudinal resection margin and transverse resection margin for hilar cholangiocarcinoma. Peripheral tissue of the bile duct can also completely be resected in Taj Mahal hepatectomy, which improves the negative rate of transverse incision margin as well. In the Taj Mahal hepatectomy, the liver must be transected along two planes to remove these liver segments, and four or more intrahepatic bile ducts will require anastomoses10. In the Taj Mahal hepatectomy, there are three technically difficult steps: the resection of the ventral part of the caudate lobule under non-hemihepatectomy,the safe dissection of vessels of the short hepatic veins and two or more hepaticojejunostomies. Because of the complex operative techniques, the Taj Mahal hepatectomy is seldom reported. The Taj Mahal procedure for the radical resection of hilar cholangiocarcinoma was first described in 19994. It was an open approach, and no serious perioperative complications were observed. Since then, few centers have reported the procedure due to its technical difficulty and a lack of surgical experience.
The robotic surgical system offers an optimal surgical view, which improves the exposure of the hilar structure and facilitates the skeletonization of the hilar duct with a thorough dissection of lymph nodes11. In addition, multiple hepaticojejunostomies are more precise and stable to perform. This parenchyma-preserving technique improves surgical tolerance and patient prognosis12. Several studies have reported the success of the radical robotic resection procedure in patients with hilar cholangiocarcinoma13,14,15. Xu et al16 reported 32 cases of robotic hemihepatectomy and caudate lobectomy in patients with hilar cholangiocarcinoma and proposed that the procedure only be conducted in strictly selected patients. A subsequent study further demonstrated acceptable long-term efficacy for robotic resection in patients with hilar cholangiocarcinoma17. These previous reports demonstrated an increasing trend for robotic radical resection in patients with hilar cholangiocarcinoma. A systematic review suggested that the feasibility and safety of radical surgery for hilar cholangiocarcinoma will be improved with technological innovations and the gradual accumulation of surgical experience, whether laparoscopic or robot-assisted systems18.
A margin-negative resection is a key factor affecting long-term survival in patients undergoing radical resection for hilar cholangiocarcinoma. The median survival (27-58 months) and 5-year survival (27%-47%) of patients with a negative margin are significantly longer compared to the median survival (12-21 months) and 5-year survival (0%-23%) of patients with a positive margin2,19,20,21,22,23. For hilar cholangiocarcinoma invading the bilateral 2nd-orderbile tract, a radical resection results in multiple stumps of the hepatic duct on the cutting surface. Performing hepatic duct reconstruction and hepaticojejunostomy safely and effectively is key to postoperative recovery and long-term outcomes. The authors' experience indicated that a maximum of eight intrahepatic bile ducts could be formed into one orifice by hepatic ductoplasty.
According to a lateset systematic review, the average hospital stay for laparoscopic surgery and robotic surgery for hilar cholangiocarcinoma was 14 days18. However, the presented data showed that the level of total bilirubin returned to normal level on POD 12, which had already reached the standard of discharge. This patient was discharged on POD 17 because of some other complications.
This article shows that the robotic Taj Mahal hepatectomy is safe and feasible for minimally invasive, radical resection in patients with hilar cholangiocarcinoma. Robotic surgery seems to have advantages over laparoscopic and open approaches in the dissection and anastomosis of the hilar bile duct. As the radical resection of hilar cholangiocarcinoma varies based on the location and extent of the lesion, thorough preoperative medical imaging examination and multidisciplinary cooperation are essential.
Disclosures
The authors have nothing to disclose.
Acknowledgements
The authors have no acknowledgment.
Materials
| 4-0 Non-Absorbable Suture | Ethicon, USA | W8761 | Synthetic non-absorbable Suture |
| 5-0 Non-Absorbable Suture | Ethicon, USA | W8556 | Synthetic non-absorbable Suture |
| Collagen Sponge | Beidi, CHINA | 20143642302 | Used for hemostasis |
| Da Vinci Robotic Surgical System | Intuitive Surgical, USA | Si | Surgical Robot Instrument |
| Disposable Ligation Clip(Medium) | KANG JI ,CHINA | KJ-JZJ06ML | Used for ligature |
| Endo GIA 60 mm Articulating Stapler with Tri-Stapler Technology | Covidien (Dublin, Ireland) | EGIA60AMT | Laparoscopic Surgical Stapler |
| EndoWrist Cadiere Forceps | Intuitive Surgical, USA | 420049 | Surgical Robot Instrument |
| ENDOWRIST Fenestrated Bipolar Forceps | Intuitive Surgical, USA | 470205 | Surgical Robot Instrument |
| EndoWrist Large Needle Driver | Intuitive Surgical, USA | 420006 | Surgical Robot Instrument |
| EndoWrist Permanent Cautery Hook | Intuitive Surgical, USA | 420183 | Surgical Robot Instrument |
| Gore-Tex Suture | Gore, USA | 4N04 | Synthetic non-absorbable Suture |
| Harmonic Ace Curved Shears | Ethicon, USA | 420275 | Used for cutting and coagulation |
| High Frequency Electrotome | COVIDIEN, USA | FORCE FX-8C | Used for electrocoagulation hemostasis |
| Silicone Catheter | Kang Wei, CHINA | Fr8 | Used for define the bile duct |
| Specimen Fetch Bag | GZTK, CHINA | HSD-130 | Used for removeing the specimen |
References
- Høgdall, D., Lewinska, M., Andersen, J. B. Desmoplastic tumor microenvironment and immunotherapy in cholangiocarcinoma. Trends in Cancer. 4 (3), 239-255 (2018).
- Mansour, J. C., et al. Hilar cholangiocarcinoma: expert consensus statement. The Official Journal of the International Hepato Pancreato Biliary Association (Oxford). 17 (8), 691-699 (2015).
- Li, H., et al. Interventional treatment for cholangiocarcinoma). Frontiers in Oncology. 11, 671327 (2021).
- Kawarada, Y., et al. S4a + $5 with caudate lobe (S 1) resection using the Taj Mahal liver parenchymal resection for carcinoma of the biliary tract. Journal of Gastxointesdnal Surgery. 3 (4), 369-373 (1999).
- Bismuth, H., Corlette, M. B. Intrahepatic cholangioenteric anastomosis in carcinoma of the hilus of the liver. Surgery Gynecology and Obstetrics. 140 (2), 170-178 (1975).
- Amin, M. B., et al. . AJCC Cancer Staging Manual. 8th ed. , (2017).
- Hirano, S., et al. Treatment strategy for hilar cholangiocarcinoma, with special reference to the limits of ductal resection in right-sided hepatectomies. Journal of Hepato-Biliary-Pancreatic Surgery. 14 (5), 429-433 (2007).
- Machada, M. A., et al. Laparoscopic resection of left liver segments using the intrahepatic Glissonian approach. Surg Endosc. 11 (11), 2615-2619 (2009).
- Marino, M. V., Pellino, G., Ahmad, A. The robotic-assisted approach for left-side predominance hilar cholangiocarcinoma: a video technique. Updates in Surgery. 72 (3), 911-912 (2020).
- Vauthey, J. N., Blumgart, L. H. Recent advances in the management of cholangiocarcinomas. Seminars in Liver Disease. 14 (2), 109-114 (1994).
- Özgüner, O., et al. Camera-robot calibration for the da Vinci robotic surgery system. IEEE Transaction on Automation Science and Engineering. 17 (4), 2154-2161 (2020).
- Araujo, R. L. C., Sanctis, M. A., Barroti, L. C., Coelho, T. R. V. Robotic approach as a valid strategy to improve the access to posterosuperior hepatic segments-Case series and review of literature. Journal of Surgical Oncology. 121 (5), 873-880 (2020).
- Cillo, U., D’Amico, F. E., Furlanetto, A., Perin, L., Gringeri, E. Robotic hepatectomy and biliary reconstruction for perihilar cholangiocarcinoma: a pioneer western case series. Updates in Surgery. 73 (3), 999-1006 (2021).
- Sucandy, I., Ross, S., Rosemurgy, A. robotic resection of a Type IIIB Klatskin tumor. Journal of Gastrointestestinal Surgery. 25 (7), 1939-1940 (2021).
- Troisi, R. I., et al. Robotic approach to the liver: Open surgery in a closed abdomen or laparoscopic surgery with technical constraints. Surgical Oncology-Oxford. 33, 239-248 (2020).
- Xu, Y., et al. Robotic radical resection for hilar cholangiocarcinoma: perioperative and long-term outcomes of an initial series. Surgical Endoscopy and Other Interventional Techniques. 30 (7), 3060-3070 (2016).
- Chou, S., et al. Robotic hilar cholangiocarcinoma radical resection compared with laparotomy in prognosis. Zhonghua Wai Ke Za Zhi. 58 (3), 230-234 (2020).
- Wang, W., et al. Laparoscopic surgery and robotic surgery for hilar cholangiocarcinoma: an updated systematic review. ANZ Journal of Surgery. 91 (1-2), 42-48 (2021).
- Stremitzer, S., et al. Prognosis and circumferential margin in patients with resected hilar cholangiocarcinoma. Annals of Surgical Oncology. 28 (3), 1493-1498 (2021).
- Gomez, D., et al. Impact of specialized multi-disciplinary approach and an integrated pathway on outcomes in hilar cholangiocarcinoma. European Journal of Surgical Oncology. 40 (1), 77-84 (2014).
- Nagino, M., et al. Evolution of surgical treatment for perihilar cholangiocarcinoma: a single-center 34-year review of 574 consecutive resections. Annals of Surgery. 258 (1), 129-140 (2013).
- Matsuo, K., et al. The Blumgart preoperative staging system for hilar cholangiocarcinoma: analysis of resectability and outcomes in 380 patients. Journal of the American College of Surgeons. 215 (3), 343-355 (2012).
- Jarnagin, W., Winston, C. Hilar cholangiocarcinoma: diagnosis and staging. The Official Journal of the International Hepato Pancreato Biliary Association (Oxford). 7 (4), 244-251 (2005).
