The procedure presented here is performed in one- to three-month-old mice in the C57BL/6J background. Male mice weighed 16-28 g, and female mice weighed 14-24 g at the time of the procedure. This procedure has been optimized to be applicable for mice of many ages, from weaning through adulthood.
Surgical orchiectomy involves a single skin incision in the ventral scrotal sac, as depicted in Figure 1A. Both testes are removed one at a time and are severed through the vas deferens and spermatic blood vessels, resulting in the removal of the testis and attached epididymis (Figure 1B). The removed contents include the testis, epididymis, and inguinal fat pad, shown in Figure 1C. Successful removal of the testicles can be confirmed by visual observation of removed tissues and ensuring good hemostasis of the tissue stump prior to closing the body cavity. The success of orchiectomy can be measured by observation of well-recovered mice that demonstrate healed incision sites (Figure 1D). Mice that have undergone orchiectomy will also demonstrate a reduction in the level of testosterone measured in mouse serum as early as a week after the procedure (Figure 1E).
Surgical bilateral ovariectomy is done by incisions into the left and right dorsum of female mice (Figure 2A). The lateral incision approach can be used if only one ovary is to be removed. In this approach, the abdominal wall is incised, and the ovarian fat pad is located. The fat pad, ovary, ovarian duct, and distal uterine horn, as depicted in Figure 2B, is exteriorized, followed by severing the distal uterine horn. This technique results in the removal of the ovary and oviduct. The ovary and ovarian duct can be removed without including the distal uterine horn, but there is a risk that any remaining ovarian cells will continue to keep the mouse in estrous cycles. Including the distal uterine horn ensures that the full ovary and duct are removed, there will be a depletion of the sex hormones, and the mice will no longer cycle. Figure 2C depicts an example of the murine female reproductive organs dissected out of the body. It can be observed that the ovaries themselves are much smaller than the surrounding tissues. A dissection scope or loupes aids in the identification of these tissues. Figure 2D demonstrates the ovarian anatomy under a dissecting scope with tissue from the uterine fat pad removed, allowing for better visualization. The success of this procedure can be measured by the observation of well-recovered mice that demonstrate healed incision sites (Figure 2E).
Ovariectomy surgery is safe and efficient when performed rapidly and with minimal disturbance to surrounding tissues. Following the procedure outlined here accomplishes this by ensuring that the skin and abdominal wall incision are positioned correctly, allowing for quick location of the uterine tissues. Identifying the inferior border of the rib cage and the superior border of the leg bones ensures the incision is made near the tissue of interest. Making an incision that is about halfway between the inferior border of the ribs and superior border of the leg bones and is located about 1.5 cm lateral to the spine allows for good positioning of the surgical site when performing a lateral incision approach (Figure 2A).
Confirmation of surgical ovariectomy is shown by observation of uterine atrophy. Figure 2F shows a uterine horn dissected from a 6-month-old mouse, while Figure 2G shows a uterine horn from a 6-month-old mouse that underwent surgical ovariectomy at three months of age. The ovariectomized uterine horn appears thinner and lacks the attachment to the ovary on the distal end. This method of confirmation of the surgical technique effectively shows that the removal of the ovary resulted in atrophy of the uterine tissue.
Once tissues have been successfully identified and excised, the surgery can be completed by closure of the wounds and careful post-operative monitoring. Proper aseptic technique14 is important in ensuring good outcomes when performing survival surgery. As the mouse begins to heal from the incisions, monitoring is performed to look for signs of pain and surgical complications. A possible surgical complication is internal bleeding because of poking or nicking blood vessels while trying to incise or manipulate the tissue. This is denoted by a persistent red, flushed appearance underneath the skin around the surgical site. Avoiding complications such as these is achieved by proper localization of incision sites and aiding the surgeon's vision by use of a surgical microscope or loupes. Visual examination is recommended every 12 hours for the first three days post-surgery. Successful surgery will result in clean, healing wounds (Figure 1D, 2E).
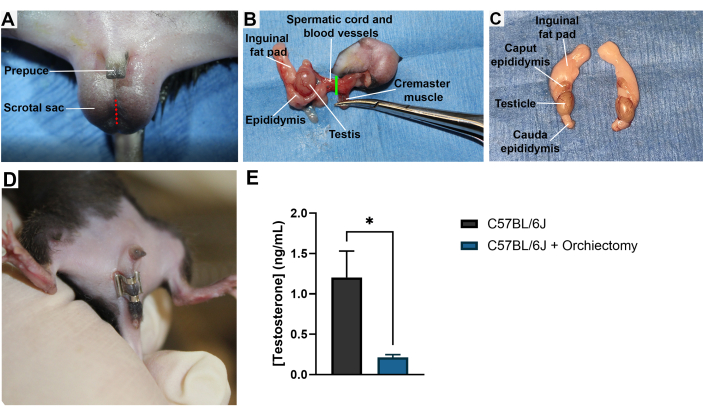
Figure 1: Male murine orchiectomy. (A) A male mouse is shown in the supine position with the location of a surgical incision into the scrotal sac for the removal of the testis, which is shown in red. (B) Image taken during the orchiectomy surgical procedure depicting the point of detachment in green. (C) Dissected-out testis, fat pads, and epididymis from a male mouse. (D) A male mouse with a well-healed wound clip over the scrotal incision following orchiectomy. (E) Mouse serum testosterone concentration in ng/mL as determined by ELISA interpolation. Both groups represent 9-week-old mice. Surgical orchiectomies were performed at 8 weeks of age. N = 3 mice per group. Samples were run in triplicate. Serum samples were collected by cardiac puncture and frozen until the time of analysis. *, p < 0.05. Error bars = SEM. Please click here to view a larger version of this figure.
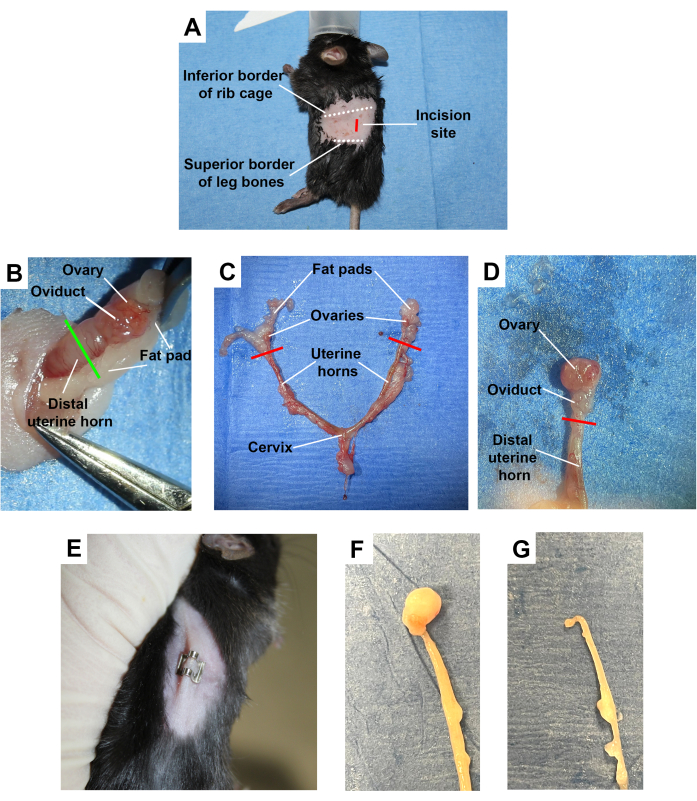
Figure 2: Female murine ovariectomy. (A) A female mouse shown in the lateral position with the surgical incision site for the removal of a single ovary from the dorsal lateral side, shown in red. Other important anatomical landmarks are highlighted. (B) Image taken during surgery depicting the exteriorized ovary, oviduct, and distal uterine horn with the point of detachment shown in green. (C) Dissected uterine horns, ovaries, and fat pads from a female mouse. (D) A close-up view of the dissected ovary, ovarian duct, and distal portion of the uterine horn with fat from the fat pad removed, allowing for better visualization of the ovary. (E) A female mouse with a well-healed wound clip over the incision following ovariectomy. (F) Dissected mouse uterine horn. (G) Dissected mouse uterine horn 3 months post-ovariectomy procedure, showing uterine atrophy. Please click here to view a larger version of this figure.
Figure 3: Graphical abstract for murine ovariectomy and orchiectomy. A pictorial representation of the orchiectomy procedure for male mice involving the removal of the testis and ovariectomy procedure involving the removal of the ovaries, both of which result in a sex hormone depleted mouse model. Please click here to view a larger version of this figure.
