LNMCP was performed successfully in 16 patients during the past year. The calculated mean age was 58.5 years (SD 8.0). All women consented to visit the hospital for follow-up after a mean duration of 6.6 months (SD 3.8). The mean estimated blood loss was 73.1 mL (SD 51.1). The mean operation time was 67.8 min (SD 15.5). There were no complication. Only one patient complained of minor lower abdominal pain occasionally. The results revealed an objective success rate of 100% until the last follow-up, while the subjective success rate was 93.8% (Table 1).
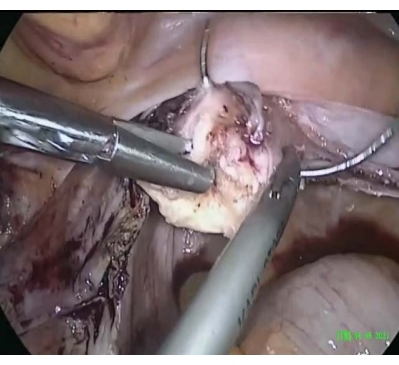
Figure 1: Cervical cerclage. Peripheral stitches were made around the cervix. Please click here to view a larger version of this figure.
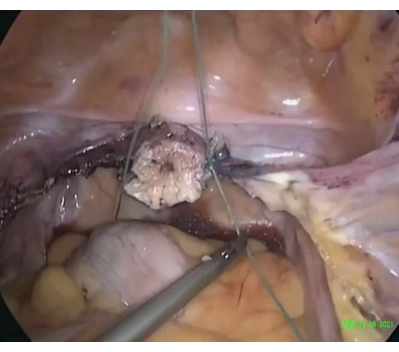
Figure 2: Completion of the cervical cerclage. The stitch was tightened and secured around the cervix, similar to the cerclage. Please click here to view a larger version of this figure.

Figure 3: Suture embedded in the round ligament. The suture was passed through and embedded in the round ligament until the iliopectineal ligament. Please click here to view a larger version of this figure.
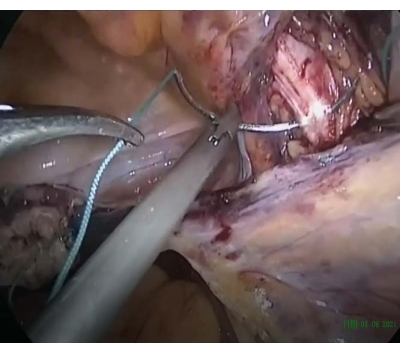
Figure 4: Suture passed through the iliopectineal ligament. The suture was passed through the iliopectineal ligament to keep a tension-free suture anchoring. Please click here to view a larger version of this figure.

Figure 5: Postoperative pelvis. The cervix was raised to POP-Q stage 0 to avoid overcorrection and ensure tension-free anchoring. Please click here to view a larger version of this figure.
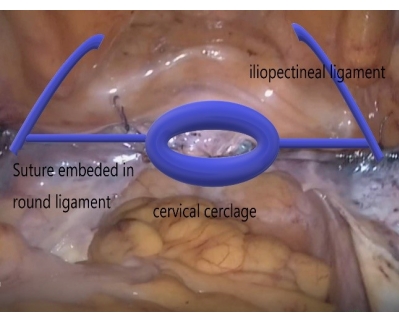
Figure 6: Schematic diagram describing the LNMCP technique. With cervical cerclage, embedding the suture in the round ligament, and fixing the suture on the iliopectineal ligament, LNMCP used only suture to treat apical prolapse and eliminated mesh-erosion complications. Please click here to view a larger version of this figure.
| Baseline demographic features of participants and the outcomes of LNMCP involving 16 cases | |
| Age | 58.5±8.0 years |
| BMI | 24.0±3.3 |
| Parity | 2.1±0.9 |
| POP-Q stage, range | 2–4 |
| Ba | 2.0±2.1 cm |
| Bp | -1.5±1.3 cm |
| C | 2.1±1.8 cm |
| Operation time | 67.8±15.5 min |
| Estimated blood loss | 73.1±51.1 ml |
| Duration of follow-up | 6.6±3.8 months |
| complications | None |
| Objective success rate | 100% |
| Subjective success rate (PGI≤ 2) | 93.80% |
Table 1: Baseline demographic features of the participants and the outcomes of LNMCP involving 16 cases. Parameters include operation time, estimated blood loss, duration of follow-up, complications, and objective and subjective success rates. BMI = body mass index. POP-Q, Ba, Bp, and C refer to scores associated with pelvic organ prolapse measurement. PGI = Patient Global Impression.
