Cells were cast into engineered muscle tissues in the 2-post consumable plate (Figure 1). Successful EMTs will appear uniform, and the matrix will be evenly distributed between the posts (Figure 2A). The matrix should also wrap around both posts, producing equivalent anchor points for the tissue. Failures in casting are rare with this method and are usually obvious with a visual inspection. Unsuccessful EMT production can range from catastrophic failures, such as tissue detachment from the posts (Figure 2B) to more subtle structural flaws, such as air bubbles and loose attachment to the posts (Figure 2C,D). Tissues with minor flaws may still be viable, but the data from these tissues should be examined carefully to ensure it is comparable to uncompromised EMTs. For example, air bubbles within an EMT may be squeezed out as the tissue compacts over time, rendering a fully functional construct without contractile deficiencies. These tissues must be evaluated on a case-by-case basis, however, as the location of the air bubbles may affect functional recovery. Air bubbles generated at the posts, for instance, may affect tissue attachment, which could impede long-term adherence to the post.
Tissues begin to compact within the first 24 h as cells remodel the matrix within the hydrogel (Figure 3). Compaction is a gradual process and usually proceeds over the first 2-4 weeks of culture. Overall, tissue compaction is consistent between technical and biological replicates (Figure 4). It is normal for some cell lines to compact the matrix more than others as tissues mature over time. The percentage of myogenic cells within a construct influences the rate and overall degree of EMT compaction. Total myogenic content for both cardiac and skeletal muscle cell lines should be above 80% to minimize variation between engineered tissues. This is particularly important when comparing contractile forces and kinetics across cell lines.
Within the first few days after casting, cardiomyocytes begin to spontaneously beat in culture, rhythmically bending the flexible post with each muscle contraction. Skeletal muscle constructs contract in response to electrical stimulation by day 7 after starting differentiation. Field stimulation was applied to skeletal muscle tissues via an external stimulator attached to a custom 24-well electrode lid. The lid, fabricated with a pair of carbon electrodes for each well, sits on top of the 24-well plate of tissues, simultaneously stimulating each EMT to induce muscle contractions. Tissues were paced using a 10 V stimulus for 10 ms pulse durations at 1 Hz during functional measurements. Contractile tissues indicate skeletal myoblasts that have fused, forming myotubes complete with functional sarcomeres and contractile machinery. Skeletal EMTs stain positive for myosin heavy chain (MyHC) and dystrophin is localized to the myotube membrane revealing a classic ring shape in cross-sectional immunohistochemical analysis (Figure 5). Once EMTs are functional, contractility can be measured daily in the magnetic sensing instrument, tracking force and kinetics as the constructs develop and mature over time. Both cardiac and skeletal muscle tissues remain contractile for weeks to months in 3D culture (Figure 6), and they can be used for a wide range of contractility studies.
The magnetic detection approach can be used to simultaneously measure acute and chronic effects of structural cardiotoxicants, such as doxorubicin (Figure 7) and BMS-986094 (Figure 8), as well as other drugs that affect muscle contractility. Optical tracking methods of contraction detection can also be used, but care must be taken when studying acute drug effects as measurements must be taken sequentially. The extended longevity of cardiac and skeletal EMTs in 3D culture enables long-term drug studies in these tissues. This permits users to explore the effects of repeat dosing, as well as continued, long-term exposure to compounds that may show cardiotoxic effects over time as occurs with doxorubicin. Doxorubicin (dox) is an anti-cancer chemotherapy drug17. The amount of drug administered to patients varies, depending on the type of cancer, age of the patient, height and weight of the patient, as well as other factors. For this reason, it is important to test the effect of dox across a wide range of concentrations and delivery schedules. Here, cardiac EMTs were treated over the course of 27 days with three separate concentrations (0.1 µM, 1 µM, and 10 µM) of dox (Figure 7). The groups were stratified further by treating EMTs at each concentration with either a bolus treatment or continuous administration with a medium change every 72 h. Wells given bolus treatments of dox were exposed to the drug at three separate time points, allowing for recovery between dosing. The two highest doses of bolus and continuous exposure showed an immediate and prolonged cessation of contractile force generation throughout the study. The middle and lowest concentrations had varying effects on the tissues, depending on the administration method. In the lowest concentration of the drug, the bolus group showed no difference from the controls. However, contractile force diminished after 2 weeks of continuous exposure. The mid-range concentration of the drug had an interesting effect. While continuous dosing reduced force over the first couple of days of treatment and lasted throughout the experiment, the bolus group showed a recovery of contractile force back to control levels when the drug was washed out after 3 days. However, the second bolus of the drug caused a full cessation of force, followed by no recovery (Figure 7), indicating that repeatedly dosing at this concentration may have a cardiotoxic effect in patients treated with this drug. The broad scope of this study, in both time and experimental conditions, highlights the utility of 3D engineered tissues in toxicity screening, as they remain contractile and responsive to chemical exposure over extended periods of time, allowing for long-term drug studies within a single set of muscle tissues. This facilitates not only identifying compounds that may have a cardiotoxic effect with chronic exposure but also detecting potential cardiotoxic timing of administration.
In vitro toxicity testing in engineered human muscle tissues is one way to help keep human patients safe in clinical trials. BMS-986094 is a nucleotide polymerase (NS5B) inhibitor used to treat hepatitis C. The drug was in Phase II clinical development when Bristol-Myers Squibb discontinued development due to several cases of unexpected heart failure in patients18,19. Here, BMS-986094 was applied to cardiac EMTs to test whether 3D engineered muscle tissues would develop a cardiotoxic reaction to the drug (Figure 8). Three different concentrations of the drug were applied, and tissues were monitored over 13 days. Contractile force dropped with the addition of the drug in a dose-dependent manner (Figure 8A). Twitch frequency was also significantly affected as the beat rate slowed and eventually stopped as expected with continued exposure to the cardiotoxic compound (p < 0.05, Figure 8B). These results demonstrate how 3D-engineered human muscle tissues can be used to facilitate bringing new drugs to the market and flag compounds that eventually fail due to cardiotoxicity. Moreover, this technology could potentially save lives by exposing dangerous drugs before they are put into patients in clinical trials.
The ability to measure the effect of acute and chronically applied drugs on human contractile tissue is a vital first step when investigating therapeutics for safety and efficacy. It is important to know, however, that the concentration of drugs applied are physiologically relevant and appropriate for in vitro testing. Skeletal muscle tissues were used to establish an IC50 value for 2,3-Butanedione monoxime (BDM) in a full dose-response curve. This drug is a well-characterized ATPase inhibitor of skeletal muscle myosin-II20. BDM inhibits muscle contractions by preventing myosin cross-bridge formation with the actin filament in sarcomeres21. Results shown here reveal a dose-dependent decrease in absolute force when the drug is applied and complete recovery of contractile force when the drug is washed out, indicating the transient effect is preventing muscle contractions and not merely killing cells within the tissue (Figure 9A). Furthermore, a full dose-response curve was measured across the seven concentrations examined, establishing an IC50 of 3.2 mM in these human microtissues (Figure 9B).
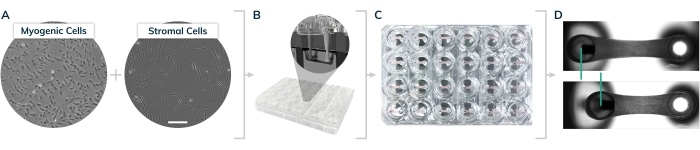
Figure 1: EMT casting in the 2-post Mantarray consumable 24-well plate. (A) Myogenic and stromal cells were cultured on 2D surfaces prior to tissue casting. (B) Cells are lifted from 2D surfaces and mixed together with extracellular matrix proteins to form hydrogels in the individual plate casting wells shown in the inset. (C) 24-well plate containing engineered tissues in every well. (D) Representative tissues showing relaxed and contracted engineered muscle, comparing displacement of the magnetic post (green bars). Please click here to view a larger version of this figure.
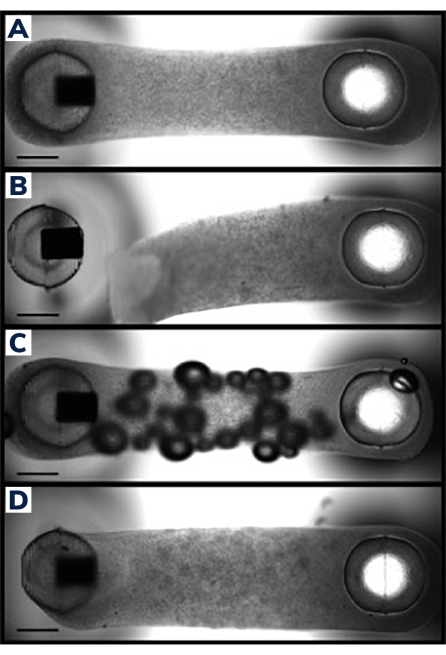
Figure 2: Successful and unsuccessful EMT casting. (A) Ideal engineered muscle tissue 24 h post-casting uniformly compacted around the posts with homogenous cell/matrix composition throughout the tissue. (B) Failed EMT showing detachment of the hydrogel from the flexible post. (C) EMT containing air bubbles throughout the tissue. (D) Unequal tissue deposition around both posts. Tissue is loosely anchored to the flexible post on one side. Scale bars are 1 mm. Please click here to view a larger version of this figure.
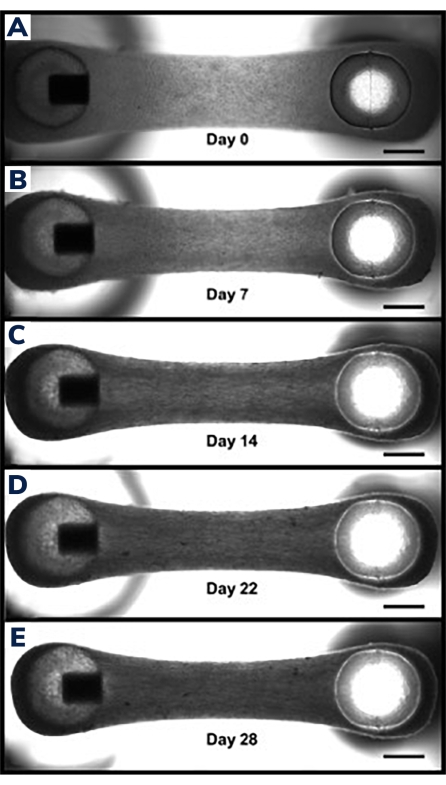
Figure 3: Compaction in engineered muscle tissue over time. (A) EMT construct shown 1 day after casting. Tissues are transferred into differentiation medium, beginning day 0 of cell fusion and hydrogel compaction. (B–E) The same EMT at day 7 through day 21 showing a slightly shorter overall length between the two posts over time and smaller width when measured through the middle section of the EMT. Scale bars are 1 mm. Please click here to view a larger version of this figure.
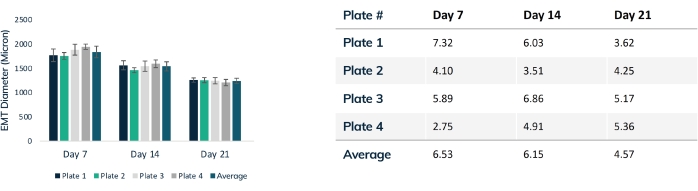
Figure 4: EMT diameter over time. Four plates of tissues were tracked over 21 days, comparing EMT diameter throughout compaction. Each tissue was measured through the mid-section every week using optical microscopy. Time points show consistent EMT size between plates. Maximal compaction is reached at day 21 as matrix remodeling is stabilized. The table shows the standard deviation (% of total) of compaction within each plate of tissues and the average deviation for all plates. Colored bars are individual plates. Error bars are SD of EMTs within plates. Please click here to view a larger version of this figure.
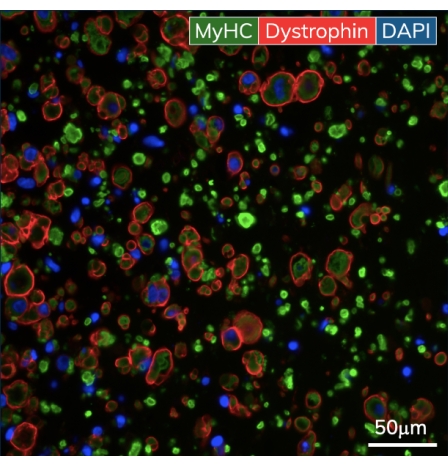
Figure 5: Immunohistochemistry of the engineered skeletal muscle tissues. EMTs were fixed on day 10 of culture and embedded in paraffin. Thin cross-sections (7 μm) were stained with antibodies against myosin heavy chain and dystrophin prior to imaging. Green = MyHC, red = Dystrophin, blue = DAPI. Objective magnification is 40X; scale bar is 50 µm. Please click here to view a larger version of this figure.
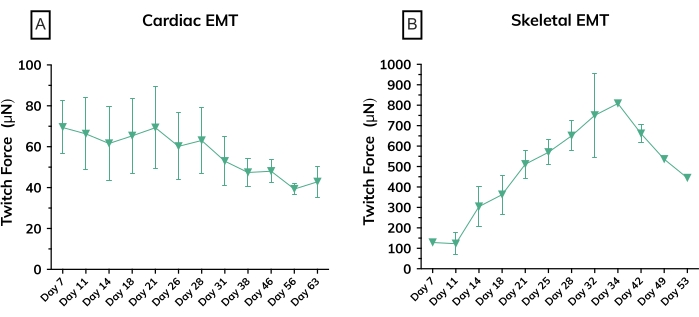
Figure 6: Contractile force in engineered muscle tissues over time. (A) Average absolute twitch force measured from cardiac EMTs from day 7 through day 63 in culture; n = 3 per group. (B) Average absolute twitch force in skeletal EMTs derived from a primary cell line on day 7 through day 53 in culture; n = 3. Error bars are SD for both graphs. Please click here to view a larger version of this figure.
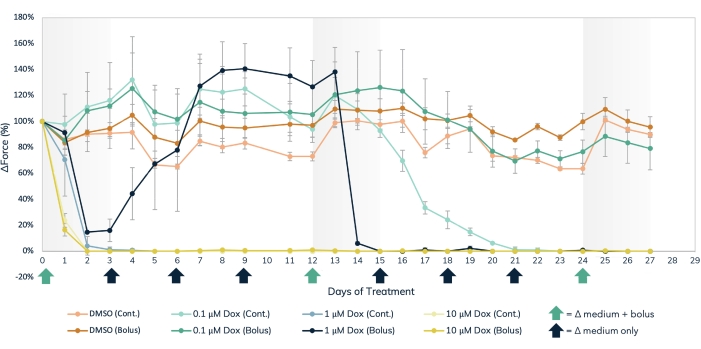
Figure 7: Acute and chronic doxorubicin treatment in the engineered muscle tissue. Three separate dose concentrations of dox, 0.1 µM, 1 µM, and 10 µM, were delivered either in bolus or administered continuously to engineered muscle tissues over the course of 27 days. Bolus doses of the drug were added at media changes on days 0, 12, and 24, noted by the green arrows on the X-axis. The drug was added to the media at every media change for continuous dosing, noted by the black and green arrows on the X-axis. The percent change in force from baseline values (pre-drug treatment) is on the Y-axis, and the time in days of treatment is on the X-axis. Light orange = DMSO continuous control, dark orange = DMSO bolus control, light green = 0.1 µM dox continuous, dark green = 0.1 µM dox bolus, light blue = 1 µM dox continuous, dark blue = 1 µM Dox bolus, light yellow = 10 µM dox continuous, dark yellow = 10 µM dox bolus. Error bars are SD; n = 3 per condition. Please click here to view a larger version of this figure.
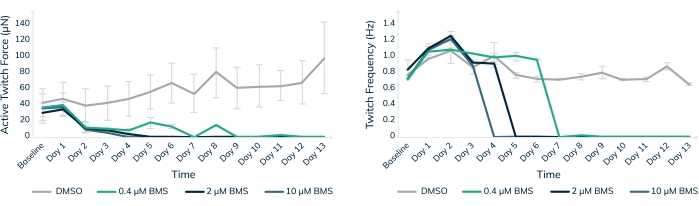
Figure 8: Chronic treatment with BMS-986094 in engineered muscle tissue. EMTs were treated with 0.4 µM (green), 2 µM (dark blue), and 10 µM (light blue) BMS-986094 over 13 days. (A) Contractile twitch force (Y-axis) decreases at all drug concentrations in the first 2 days, whereas the control tissues in DMSO continue to get stronger over time (X-axis). (B) The cardiac beat rate, or twitch frequency, ceases in a dose-dependent like manner in tandem with a cessation of contractile force shown in graph A. Control tissues in DMSO (gray) maintain a regular beat rate throughout the experiment. Error bars are SD; n = 3 per condition. Please click here to view a larger version of this figure.
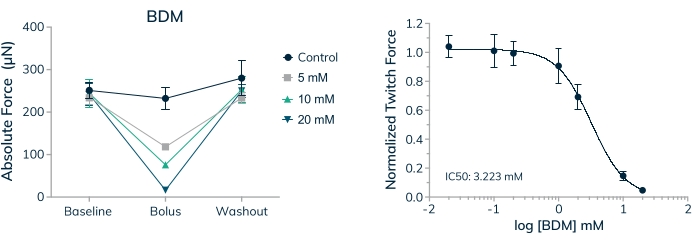
Figure 9: Dose-response to BDM in engineered skeletal muscle tissues. (A) Absolute twitch force decreases in a dose-dependent manner when primary cell-derived EMTs are exposed to 2,3-Butanedione monoxime (BDM) on day 16 in 3D culture. Absolute twitch force returns to near baseline values when the drug is washed out. (B) Absolute twitch force normalized to baseline values decreases in a dose-dependent manner when exposed to BDM yielding a full dose-response curve and IC50 value; n = 4 per dose. Error bars are SD. Please click here to view a larger version of this figure.
