Search results
A total of 1,117 studies were identified from databases, including 204 in Chinese and 913 in English. After eliminating 392 duplicates, 725 studies remained. After reading the titles and abstracts, 31 studies remained. Eventually, 14 studies were included through reading the full texts. The search process and selection procedure are shown in Figure 1.
Study characteristics
The characteristics of the included studies are provided in Table 1. The 14 studies involved 1,283 patients with insomnia (644 treated with and 639 treated without Shugan Jieyu capsules), including 445 females (35%), 528 males (41%), and 310 patients of unknown gender. The patients ranged in age from 18 to 74 years, with an average of 46 years. There were no statistically significant baseline differences in patient gender, age, or basic disease between the experimental and control groups in the 14 studies. All the randomized controlled trials (RCTs) were conducted in China.
Methodological quality
The methodological quality assessment results of the 14 studies are shown in Figure 1 and Figure 2. Five trials reported specific randomization methods (random number table)48,49,50,51,52 and, thus, were assessed as low risk. One trial53 was judged as high risk, using the order of consultation, and other trials mentioned randomization but no specific methods. None of the trials reported minute details of allocation concealment and blinding of the outcome assessment. None of the studies used placebo, and blinding appeared unlikely to be implemented, so the risk of participant bias and lack of personnel blinding was considered high. In all the studies, the risk of incomplete outcome reporting was lower. For five25,50,53,54,55 studies, it was difficult to determine whether there was a risk of selective reporting. Two studies47,48 had unclear risks due to incomplete baseline measurements.
Primary outcomes
Nine studies24,49,50,51,52,54,56,57,58, including 866 patients, reported the total number of clinically effective cases. The total clinical effectiveness rate was 94% (406/433) in the experimental group compared to 73% (317/433) in the control group. Compared with the control group, the total clinical effectiveness was significantly higher in the experimental group (OR: 5.71, 95% CI: 3.56 to 9.15, I2 = 0%) (Figure 3). Eight studies stated that the experimental group showed reduced overall PSQI scores compared to the control group, and one study reported opposite results25. After pooling the data, the mean difference (MD) was −2.95 (95% CI: −4.97 to −0.93, I2= 97%) (Figure 4).
Secondary outcomes
Eight studies24,48,49,52,53,56,57,58, including 717 patients, reported a number of adverse events. The adverse reaction rate was 13% (45/358) in the experimental group compared to 21% (74/359) in the control group. The experimental group had significantly fewer adverse reactions (OR: 0.56, 95% CI: 0.32 to 0.97, I2 = 35%) (Figure 5). The experimental group did not show a significant reduction in sleep latency (MD: −0.26, 95% CI: −1.32 to 0.80, I2 = 96%) (Figure 6). Four studies49,50,52,55, including 392 patients, reported the sleep duration. Three studies showed that the experimental group showed statistically significant improvements in sleep duration, and one study reported that the experimental group did not differ significantly from the control group in terms of sleep duration52. After pooling the data, the MD was 1.06 (95% CI: 0.11 to 2.01, I2 = 91%) (Figure 7).
In comparison with the control group, the experimental group was associated with a significant decrease of −0.46 in night awakening (95% CI: −0.57 to −0.35, I2 = 0%), of −0.48 in nightmares with excessive dreaming (95% CI: −0.56 to −0.39, I2 = 0%), of −0.40 in daytime sleepiness (95% CI: −0.69 to −0.10, I2 = 87%), and of −0.41 in low energy (95% CI: −0.54 to −0.29, I2 = 0%) (Figure 8, Figure 9, Figure 10, Figure 11). Additionally, the experimental group showed significantly improved sleep quality (MD: −0.78, 95% CI: −1.54 to −0.02, I2 = 90%) (Figure 12).
Quality of evidence
The results of the GRADE46 evaluation on the studies examining the effectiveness and safety of Chinese medicine Shugan Jieyu capsules for insomnia treatment showed that the evidence qualities were medium, low, or very low. The details can be found in Supplementary Table 1.
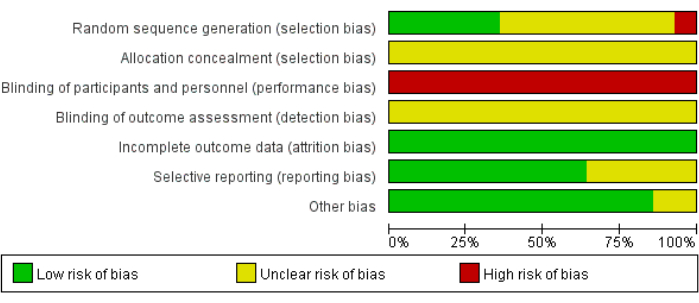
Figure 1: Assessment of the risk of bias according to the authors' judgment. This graph represents the percentages of respective bias across all the included literature. Please click here to view a larger version of this figure.
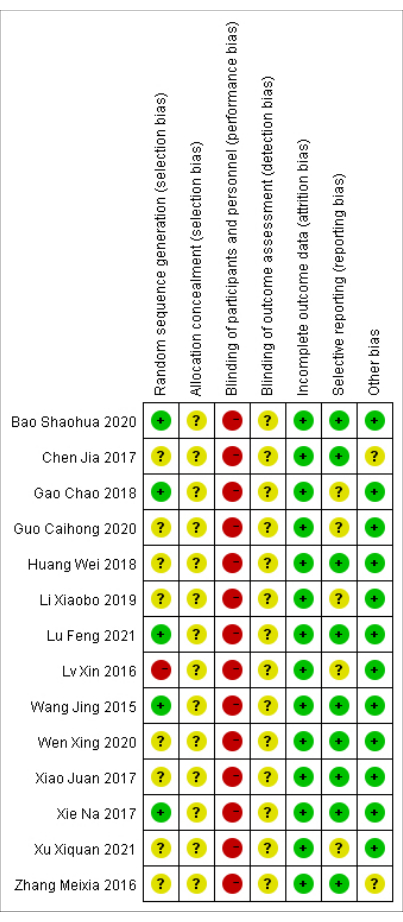
Figure 2: Risk of bias summary. The specific biases identified for each study included in the analysis. The red, yellow, and green circles represent high, unclear, and low risk of bias, respectively. For further details, please see Table 1. Please click here to view a larger version of this figure.
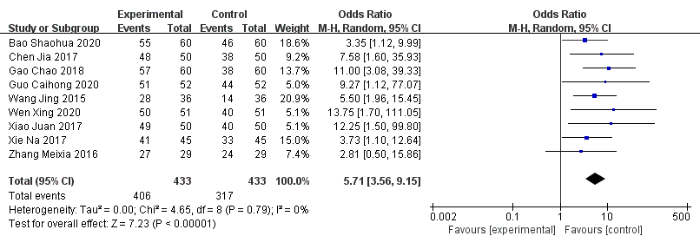
Figure 3: Forest plot for the pooled analysis of the total clinical effectiveness. Please click here to view a larger version of this figure.
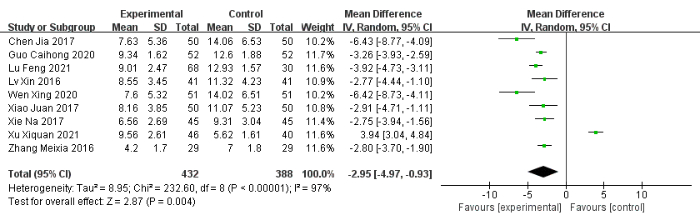
Figure 4: Forest plot for the pooled analysis of the PSQI total score. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.
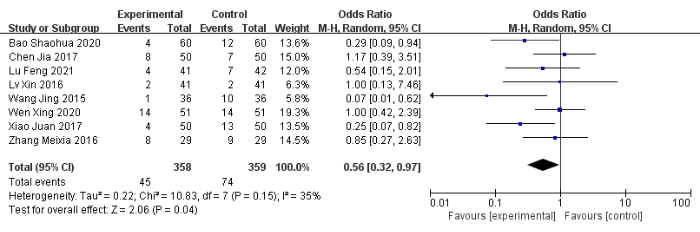
Figure 5: Forest plot for the pooled analysis of the improvement of adverse reactions. Please click here to view a larger version of this figure.

Figure 6: Forest plot for the pooled analysis of sleep latency improvement. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.
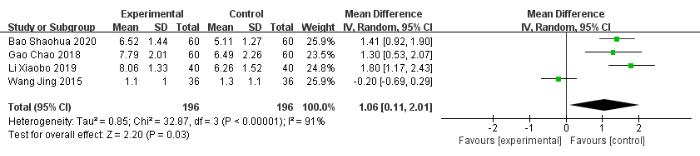
Figure 7: Forest plot for the pooled analysis of sleep duration improvement. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.
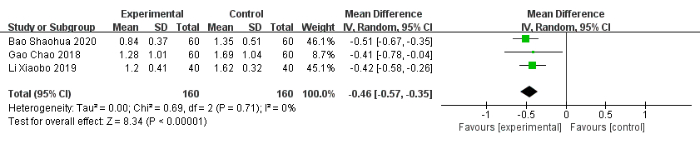
Figure 8: Forest plot for the pooled analysis of night awakening. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.
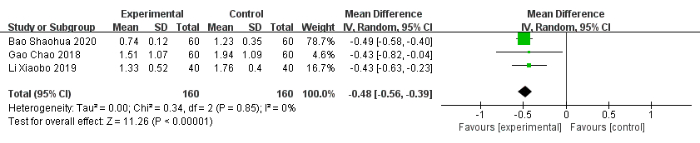
Figure 9: Forest plot for the pooled analysis of nightmares with excessive dreaming. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.
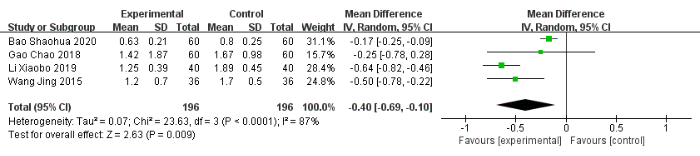
Figure 10: Forest plot for the pooled analysis of daytime sleepiness. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.

Figure 11: Forest plot for the pooled analysis of low energy. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.

Figure 12: Forest plot for the pooled analysis of sleep quality. Abbreviation: SD = standard deviation. Please click here to view a larger version of this figure.
Table 1: Basic information of the included studies. *: (1) Total clinical efficiency; (2) PSQI overall score; (3) Adverse reactions; (4) Sleep latency; (5) Sleep duration; (6) Night awakening; (7) Nightmares with excessive dreaming; (8) Daytime sleepiness; (9) Low energy; (10) Sleep quality. Abbreviations: T = experimental group; C = control group; "-" = not mentioned. Please click here to download this Table.
Supplementary Figure 1: Handling the PubMed database. (A) The main window of the literature search in Pubmed. (B) The main window for downloading all the retrieved literature in Pubmed. Please click here to download this File.
Supplementary Figure 2: Working in Endnote. (A) The main window for importing the retrieved literature in Endnote. (B) The main window for creating the inclusion and exclusion groups in Endnote. (C) The main window for removing duplicates in Endnote. Please click here to download this File.
Supplementary Figure 3: Adding research to RevMan. (A) The main window for creating a new file in RevMan. (B) The main window for adding the included literature in RevMan. (C) The main window for entering the quality evaluation results in RevMan. Please click here to download this File.
Supplementary Figure 4: Literature quality evaluation in RevMan. (A) The main window for creating a graph of RoB in RevMan. (B) The main window for adding the outcome indicators in RevMan. Please click here to download this File.
Supplementary Figure 5: Meta-analysis. (A) The main window for adding the study data in RevMan. (B) The main window for creating forest plots in RevMan. Please click here to download this File.
Supplementary Table 1: GRADE evidence profile. 1, downgrade one level: the quality of included literature is low; 2, downgrade one level: heterogeneity in the data synthesis results, I2 > 50%; 3, downgrade one level: the confidence interval is too wide; 4, downgrade one level: the sample size is too small. Abbreviations: MD = mean difference; OR = odds ratio; CI = confidence interval. *: the overall quality of the evidence. Please click here to download this File.
Supplementary File 1: The details of the retrieval strategy for this study. Please click here to download this File.
Supplementary File 2: PRISMA checklist. Overall, 1,117 articles were identified initially through the literature search, and 14 full-text articles were reviewed and entered into the final analysis. Please click here to download this File.
