All procedures were performed following the Canadian Council on Animal Care guidelines after approval by the Institutional Animal Care Committee of the CRCHUM. Eight-week-old female BALB/c mice, obtained from a commercial source (see Table of Materials), were used for the present study. The animals received dietary supplementation with 10% inulin wt/wt for 2 weeks. A control group received a similar diet lacking the inulin supplement. Mice had ad libitum access to the diet. An overview of the assay is shown in Figure 1.
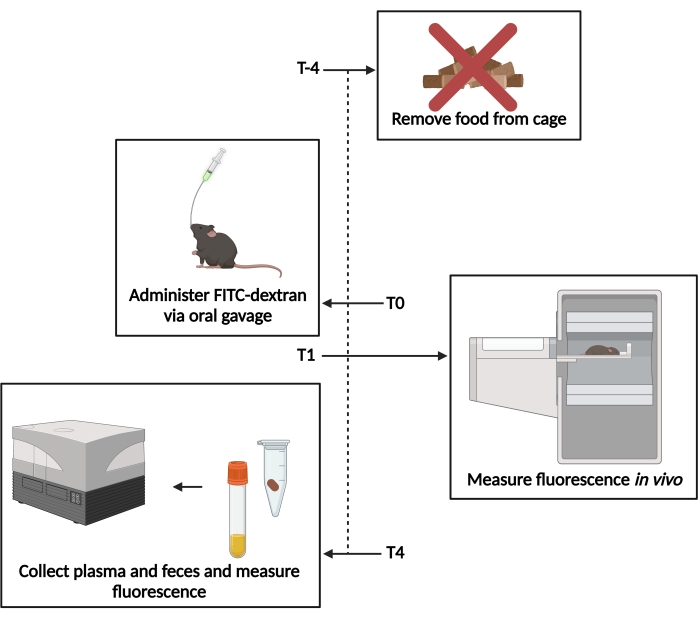
Figure 1: Schematic of the FITC-dextran assay. T−4– 4 h prior to gavage, food access was removed. T0– FITC-dextran was administered via oral gavage. T1 – 1 h post gavage, the in vivo fluorescence was evaluated. T4– 4 h post gavage, the fecal and plasma samples were collected, and the fluorescence was measured. Please click here to view a larger version of this figure.
1. Administration of FITC-dextran
- Prior to administering FITC-dextran, fast the mice for 4 h while maintaining ad libitum access to water.
NOTE: The fasting must preferably be initiated at the beginning of the light cycle (in the morning). The mice may be transferred to a new cage without bedding during fasting to limit coprophagy. - Prepare 200 µL of 80 mg·mL−1 4 kDa FITC-dextran (see Table of Materials) diluted in sterile 1x phosphate-buffered saline (PBS) (per mouse). Freshly prepare the samples immediately prior to administration, and keep them protected from light.
- Administer 200 µL of the FITC-dextran suspension via oral gavage to each mouse using a 38 mm 22 G sterilized, curved gavage needle with a ball- or pear-shaped tip (see Table of Materials). Start a timer after the first gavage, and wait for 5-10 min before gavaging the next mouse to allow for in vivo measurements (step 2), always maintaining 1 h post gavage. Keep the remaining FITC-dextran suspension for the standard curve.
NOTE: Immediately following the gavage, food may be replaced to ensure the formation of feces.
2. In vivo fluorescence measurement
- Anesthetize the mice 1 h after the gavage using 2.5% isoflurane or an alternative anesthetic. Confirm that the animal is appropriately anesthetized by pinching the toe or the tail and ensuring that the animal does not react.
- Remove the fur from the abdominal area using an electric shaver, and generously apply ophthalmic lubricating ointment to the eyes to prevent drying. Then, place the mice individually in the imaging chamber lying dorsally.
NOTE: One control mouse must be included that receives PBS or saline instead of FITC-dextran to account for background during in vivo imaging.
- Remove the fur from the abdominal area using an electric shaver, and generously apply ophthalmic lubricating ointment to the eyes to prevent drying. Then, place the mice individually in the imaging chamber lying dorsally.
- Image the mice using a fluorescence imaging chamber (see Table of Materials). Acquire images of the abdominal region, setting the laser length at 470 nm and the resolution at 2.0 mm.
- Start the machine and software by clicking and holding the start button. Allow the system to warm up.
NOTE: The system may need 20 min or more to warm up, so the machine must be started early so as not to interfere with imaging the mice at 1 h after gavage. - Click on Device status and ensure all the configured devices show "OK" before proceeding.
- If needed, warm up the appropriate laser by clicking on Laser control and then clicking on the Laser name button of the desired laser.
- Start a new study by clicking on New study. Save under the appropriate file with the desired name.
- Click on Study options, then enter the Specimen ID, and choose the correct laser and experiment.
- Open the imaging chamber and place the animal dorsally on the scanning plate. Secure the limbs and tail with tape, and ensure that the nose and mouth fit snugly in the anesthesia tube, maintaining 2.5% isoflurane.
- Adjust the height of the scanning plate so that the scanning region is slightly ventral from the animal's midline. Adjust the plate by turning the adjustment knob inside the imaging chamber. Close and lock the imaging chamber door.
- Select the area to be scanned by using the Draw tool. Include the whole width of the abdomen from just above the liver to the rectum. Click on the Modify tool to adjust the area once drawn.
- Set the scan resolution to 2.0 mm, and then click on Next. Once power automation is completed, ensure that the settings are correct, and make any adjustments needed. Click on Start to begin the scan.
- Once the scan is complete, remove the animal from the imaging chamber, and place it in an incubator to maintain body temperature while recovering from anesthesia.
- Click on Continue study to maintain the settings, and then repeat steps 2.2.5-2.2.10 until all the mice have been scanned.
- Click on the power button and hold it for 3 s to power down the imaging chamber.
- Start the machine and software by clicking and holding the start button. Allow the system to warm up.
- Evaluate the fluorescence by comparing the abdominal fluorescence of each animal and the control mouse on uniformly scaled images using a software associated with the imaging system used (see Table of Materials).
- Open the image files by finding them under the chosen file name. Open all the files that have synchronized settings at the same time.
- Using the image settings toolbar, use the Sync image and Sync scale buttons to sync the settings for the images, allowing for an accurate comparison.
- Save the images with their adjusted scales.
3. Fluorescence measurement in fecal samples and plasma
- Collect a fecal pellet from each mouse in a sterile tube 4 h after gavage. Keep the tubes in the dark on ice.
- Anesthetize the mice via intraperitoneal injection of 240 mg/mL pentobarbital sodium (dilution, 1:100; see Table of Materials). Administer at a dose of 0.03 mL/g body weight.
- Collect blood samples of at least 700 µL in a tube made for plasma collection containing heparin or EDTA to prevent clotting (see Table of Materials) by inserting a glass capillary tube into the retro-orbital plexus14.
NOTE: Alternative methods for blood collection include cardiac puncture or withdrawal from the tail vein. As this is a terminal procedure, the mice need to be euthanized via cervical dislocation or an alternative humane method. Follow local animal ethics committee recommendations for euthanasia.
- Collect blood samples of at least 700 µL in a tube made for plasma collection containing heparin or EDTA to prevent clotting (see Table of Materials) by inserting a glass capillary tube into the retro-orbital plexus14.
- Centrifuge the blood samples at 9,390 x g for 10 min at room temperature. Transfer the plasma to a new sterile tube, and keep it in the dark on ice.
- Dilute 50 mg of fecal samples in 200 µL of 1x PBS and dilute the plasma 1:2 with 1x PBS. The dilution ratio can be modified based on the intensity of the fluorescence signal.
- Generate a standard curve using serial dilutions of FITC-dextran in 1x PBS. Starting with the highest concentration of 20 mg·mL−1 FITC dextran, dilute by a factor of 1:1 serially 7-10 times.
NOTE: The concentrations, thus, must read 20 mg·mL−1, 10 mg·mL−1, 5 mg·mL−1, 2.5 mg·mL−1, 1.25 mg·mL−1, 0.625 mg·mL−1, 0.3125 mg·mL−1, etc. - Plate 100 µL samples and standards in an opaque black 96-well plate. Include a PBS blank. Read the fluorescence on a fluorescent plate reader (see Table of Materials) with the absorption at 530 nm and the excitation at 485 nm.
NOTE: The samples and standards can be plated in duplicate or triplicate, and then their fluorescence values are averaged. - Determine the concentration of FITC-dextran per sample by comparing the fluorescence to the known concentrations of the standard curve. In the samples, multiply the concentration by the dilution factor (step 3.5).
The analysis of the in vivo fluorescence showed that mice who received only the control diet had a higher hepatic intake of FITC-dextran and higher levels of residual fluorescence in the abdominal cavity compared to the mice who received the inulin-supplemented diet (Figure 2A). Some fluorescence was visible in the caecum of the mice that received the inulin diet, but there was little to no hepatic intake, indicating that these diets protected against increased intestinal permeability.
The fluorescence levels in plasma and fecal samples work to reinforce and quantify their in vivo counterparts. The mice that received the inulin-supplemented diet had significantly lower levels of FITC-dextran in their plasma compared to the mice that received only the control diet (Figure 2B). This indicates that they had improved gut barrier function because less FITC-dextran could permeate the intestinal barrier into the circulation. Concordantly, the mice that received the inulin diet had significantly higher levels of FITC-dextran in their feces than the mice that received only the control diet (Figure 2C). This reinforces that they had intact gut barrier function as the FITC-dextran remained in the colon until excretion, as is considered normal. The lower levels of FITC-dextran in the feces of the control mice indicate that it permeated through the intestinal barrier into the circulation rather than being appropriately excreted. The high levels of FITC-dextran in the plasma reinforce this finding.
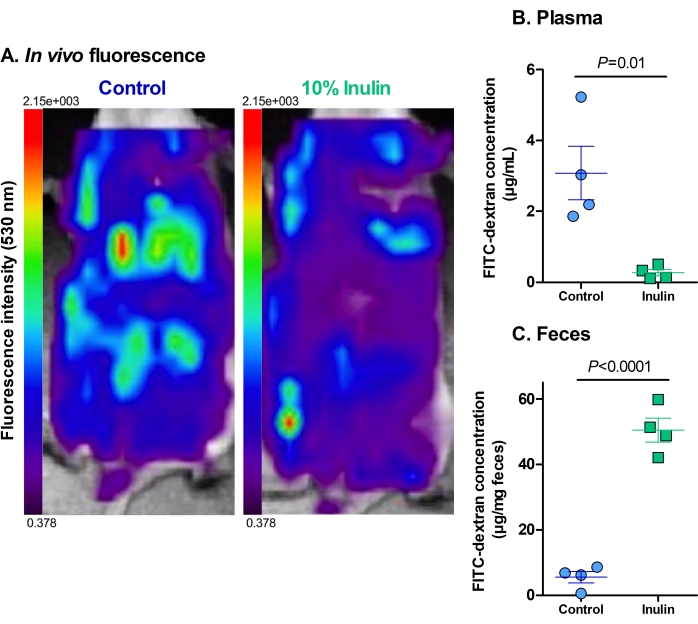
Figure 2: Dietary supplementation with inulin decreases the translocation of FITC-dextran through the gut barrier. (A) The residual fluorescence and hepatic uptake of FITC-dextran. Red = highest intensity; dark purple = lowest intensity. Maximum fluorescence of 2.15 x 103, minimum fluorescence of 0.378. (B) The plasmatic concentration of FITC-dextran. P = 0.010. (C) The fecal concentration of FITC-dextran. P = 0.00003. N = 4 per group. Data are represented as mean ± SEM. Each dot represents one mouse. Unpaired Student's t-test. Please click here to view a larger version of this figure.
