This paper demonstrates that the concurrent application of LIFU sonication and MB administration is an effective technique for localized BSCB disruption. The opening of the BSCB is indicated by the presence of EBD extravasation into the spinal parenchyma. The changes are apparent both visually and under fluorescence microscopy. The spinal cord vasculature is visible after laminectomy and shows the posterior spinal vein with multiple smaller vessels radiating laterally (Figure 4A). Intravenous injection of EBD through the tail vein catheter results in this vasculature being enriched with blue dye (Figure 4B). This is a good point in the procedure to verify that the laminectomy did not result in the rupture of any spinal vasculature, as this would result in blue blood pooling over the cord. After sonication, a spot of blue should become visible over the targeted location, indicating the extravasation of EBD into the white parenchyma due to BSCB disruption (Figure 4C). The size of this spot varies based on a number of factors, including the size of the focal region of the transducer and the amount of time after sonication. To increase the chances of seeing EBD extravasation, one should lengthen the amount of time between sonication and spinal cord extraction.
Although PFA perfusion is not a necessary step to perform prior to cord extraction and subsequent tissue analysis, it removes blood from the sample and increases the contrast between the white spinal parenchyma and the blue EBD-stained regions. All rats that received MB administration and LIFU sonication show apparent extravasation of EBD into the spinal cord, while negative controls that received MBs and EBD with no LIFU sonication do not. Representative images are shown in Figure 5. Sagittal cuts through the tissues reveal that the EBD extravasation is not only superficial, but extends well into the cord itself. This is expected, since the focal region of the transducer used in this study is greater than the diameter of the rat spinal cord. Sometimes, small amounts of hemorrhage may be seen in the sagittal cuts. This can be due to the laminectomy or the ultrasound sonication. If the hemorrhage is close to the dorsal periphery of the cord, it is more likely due to the laminectomy.
To further evaluate EBD extravasation, sagittal spinal cord sections were stained with DAPI (nuclear marker) and imaged using a fluorescent microscope. All cords that received LIFU sonication (n = 3) showed a significantly greater intensity of EBD autofluorescence (p = 0.016) than cords that did not receive sonication, with similar intensities of DAPI present in both (Figure 6). H&E analysis further revealed no neuronal damage, hemorrhage, or cavity lesions present in the sonicated locations, supporting the safety of this procedure. Examples of injured cords due to surgical mishandling and a high-powered sonication are shown as a comparison. Hemorrhage, tissue damage, cavity lesions, and possible vacuolization are labeled. Although the high-power sonication example does not show hemorrhage, this has also been reported as an effect of ultrasound disruption.
Furthermore, behavioral analysis was conducted on rats that received MBs, EBD, and LIFU sonication. Although this method does not completely exclude tissue damage, it does test if motor deficits occurred due to this procedure. Rats were recorded walking in a cage for 5 min every day over a period of 5 days, and locomotor function was graded based on the Basso Beattie Bresnahan locomotor scale (Supplemental Video File 1). All rats (n = 5) received the highest score before sonication, post-sonication, and every day of the survival period (Figure 7).
Finally, the thermal effects of the sonication parameters used in this study were measured using two ex vivo rat spinal cord samples and a digital thermometer probe with a fine tip inserted into the cord. The temperature of the spinal cord samples was tracked for 5 min before, during, and after sonication, for a total of 15 min. Minimal changes in temperature were seen. In fact, there was ≤1.3 °C change due to sonication in both samples, decreasing the likelihood of hyperthermic injury as a result of sonication (Figure 8).
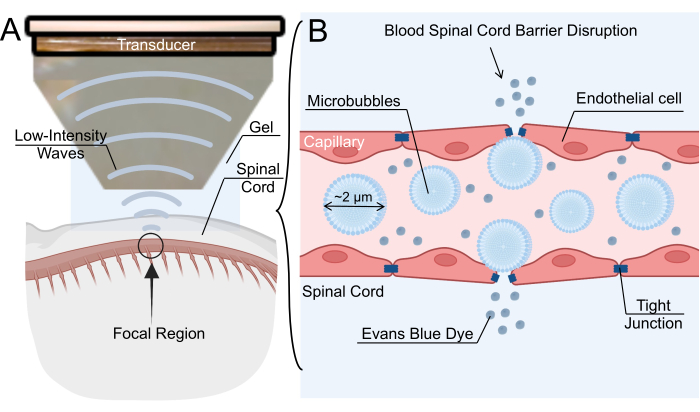
Figure 1: Low-intensity focused ultrasound-mediated blood-spinal cord barrier opening mechanism. (A) Schematic overview of low-intensity focused ultrasound (LIFU) sonication of rat spinal cord. (B) The mechanism for blood-spinal cord barrier (BSCB) opening via LIFU sonication of intravenous microbubbles (MBs). MBs oscillate in response to LIFU, causing the widening of tight junctions between endothelial cells. This disruption of the BSCB allows for the extravasation of nanoparticles, therapeutic drugs, or Evans blue dye. Please click here to view a larger version of this figure.
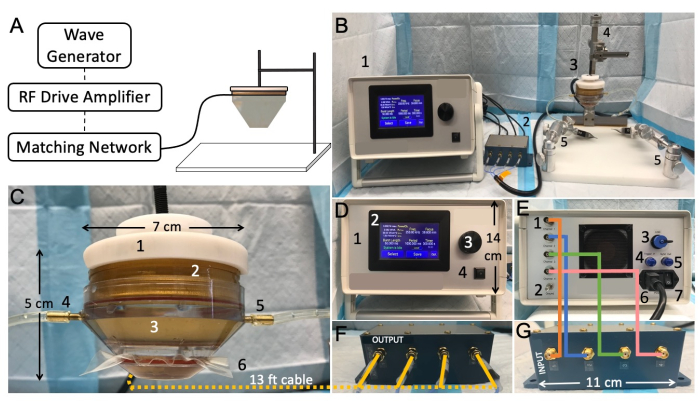
Figure 2: Low-intensity focused ultrasound benchtop setup and connectivity. (A) Schematic representation showing typical focused ultrasound components. (B) Overview picture of the focused ultrasound setup, including: 1. transducer power output (TPO), 2. matching network, 3. LIFU transducer, 4. the stereotaxic instrument, 5. mobile clamps. (C) Transducer, including: 1. probe holder, 2. ring transducer, 3. water cone, 4. water-Inlet tube, 5. water-outlet tube, 6. membrane secured with a rubber band. (D) Front of the TPO, including: 1. RF shielded enclosure, 2. touch-sensitive front display panel with adjustable menu, 3. rotating knob for parameter adjustment, 4. start/stop output switch. (E) Back of the TPO, including: 1. channel output connectors, 2. ground, 3. USB input port for software control, 4. internal trigger, 5. sync output connector, 6. power input jack and supply, 7. on/off power switch. (F) Matching network output, with wires matching channel numbers. (G) Matching network XDR input, with wires matching channel numbers Please click here to view a larger version of this figure.
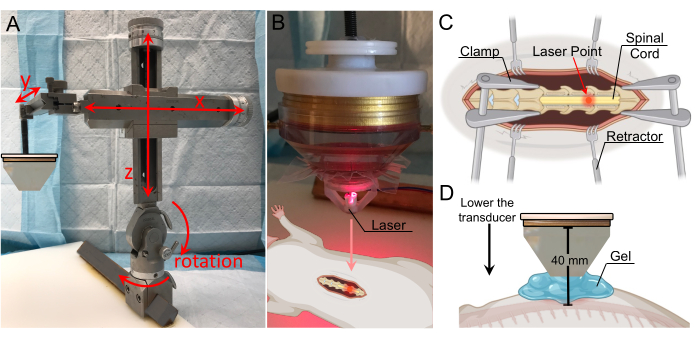
Figure 3: Target localization with laser guidance. (A) Stereotactic arm with range-of-motion in all three axes and rotation capabilities. It is affixed to the fixation plate below. (B) Laser apparatus for identification of the focal zone. The laser is positioned on the tip of the transducer and is in line with the focal region. (C) Illustration showing the laser on the exposed spinal cord, indicating the transducer's focal region is now directed to this location. (D) The transducer is lowered until the tip of the cone is located 1 cm above the cord, and the gap is filled with gel to ensure maximal coupling. The distance from the transducer to the spinal cord is 40 mm (focal distance). Please click here to view a larger version of this figure.
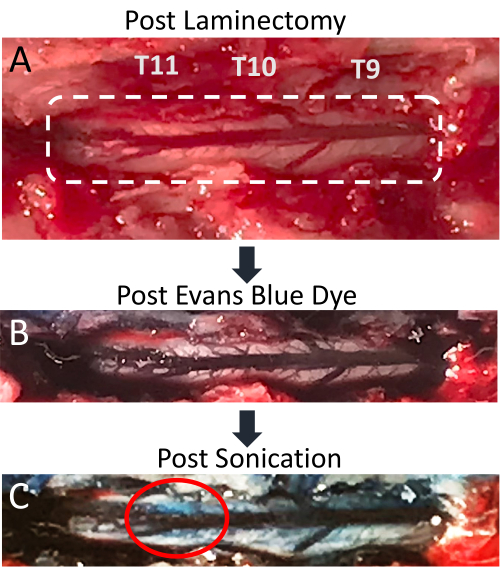
Figure 4: Evans blue dye extravasation in spinal cord post-sonication. (A) Picture of T9-T11 rat laminectomy incision, with the exposed spinal cord and posterior dorsal vein clearly visible. (B) The surrounding tissue and spinal cord vasculature become blue after intravenous injection of Evans blue dye (EBD). (C) EBD extravasation into spinal cord parenchyma at the site of sonication, indicating BSCB disruption has occurred. Please click here to view a larger version of this figure.
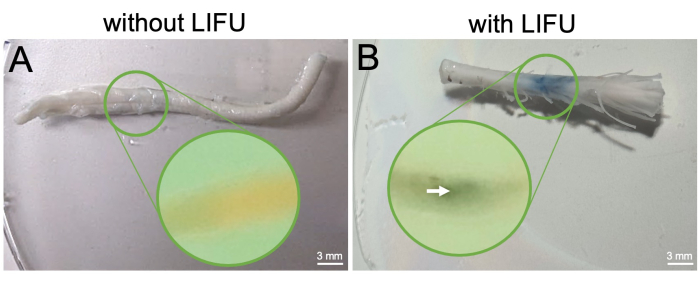
Figure 5: Spinal cord extraction and visualization of BSCB opening post-perfusion. (A) Excised spinal cord from control rat without LIFU treatment. This rat only received MBs and EBD. Mid-sagittal slice of the cord embedded in paraffin is shown in the inset, and no EBD extravasation is visible. (B) Excised spinal cord from rat with LIFU treatment. This rat also received MBs and EBD. The column of EBD extravasation is visible and localized to the sonicated region. Mid-sagittal slice of the cord embedded in paraffin is shown in the inset, with an arrow pointing to the EBD concentration visible inside the sonicated location. Please click here to view a larger version of this figure.
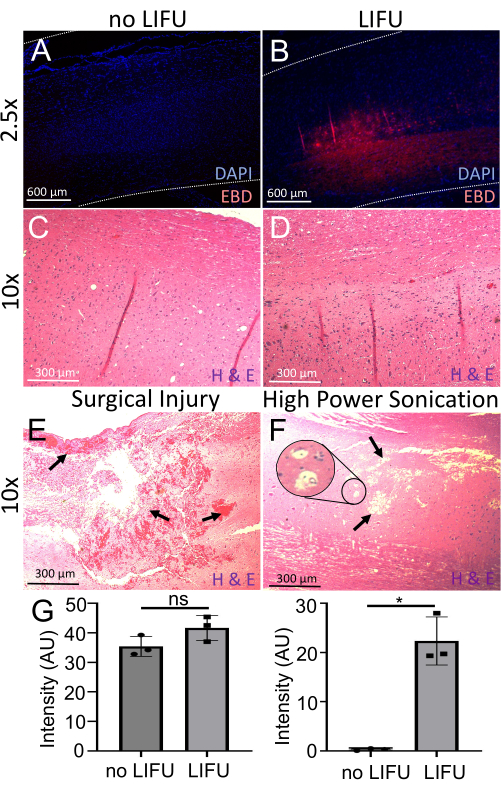
Figure 6: Detection and evaluation of BSCB opening. (A) Spinal cord stained with DAPI (nuclear marker, blue). Minimal EBD autofluorescence (red) is visible. This rat did not receive LIFU. (B) Spinal cord stained with DAPI (nuclear marker, blue). Localized EBD autofluorescence (red) at the sonicated target location is visible. This rat received LIFU and MBs. (C) The spinal cord of a rat without LIFU stained with hematoxylin (nucleic acid stain) and eosin (nonspecific protein stain) (H&E). No neuronal damage, hemorrhage, or cavity lesions are visible. (D) The spinal cord of a rat with LIFU stained with H&E. No neuronal damage, hemorrhage, or cavity lesions are visible. (E) Spinal cord of a rat with surgical injury stained with H&E. Arrows point to ample hemorrhage and tissue damage. (F) The spinal cord of a rat with damage due to high power sonication stained with H&E. Arrows point to cavity lesions, and the inset shows possible vacuolization. (G) Bar graphs showing the intensity of DAPI and EBD in spinal cords of rats with and without LIFU sonication. There is significantly more EBD intensity in the LIFU spinal cord when compared to the negative control (p = 0.016), despite similar DAPI intensity (p > 0.05). Please click here to view a larger version of this figure.
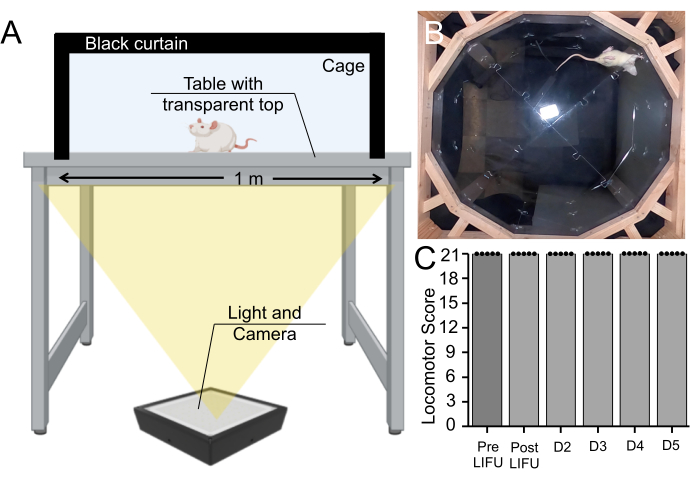
Figure 7: Behavioral assay pre- and post-sonication. (A) Basso, Beattie, Bresnahan apparatus setup, in which rats were recorded walking for 5 min from below. (B) Still image from a recorded video. This video was used to rate the rat's motor coordination and gait on the Basso, Beattie, Bresnahan scale. (C) Boxplot (n = 5) showing no change in motor scores pre-sonication, post-sonication, or during a 5-day survival period in rats that received MBs and LIFU treatment (p > 0.05). Please click here to view a larger version of this figure.
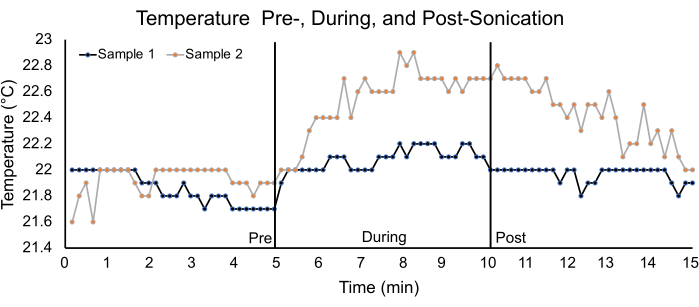
Figure 8: Temperature analysis using ex vivo spinal cords. Graph depicting temperature changes in two ex vivo spinal cord samples for a 5 min pre-, during- and post-sonication duration. The parameters used for sonication are listed in Table 1. For sample 1, the pre-, during-, and post-sonication average temperatures were 21.9 °C ± 0.1 °C, 22.1 °C ± 0.1 °C, and 22.0 °C ± 0.1 °C, respectively. For sample 2, the pre-, during-, and post- sonication temperatures were 21.9 °C ± 0.1 °C, 22.5 °C ± 0.3 °C, and 22.4 °C ± 0.2 °C, respectively. Please click here to view a larger version of this figure.
Supplementary Figure 1: CAD file of laser targeting apparatus. (A) View of the laser apparatus from below. Any laser can be placed within the central hole in the middle. (B) Lateral view of the laser apparatus. (C) Dimensions of the laser apparatus, with units in inches. Please click here to download this File.
Supplementary Video File 1: Video of a rat walking in the Basso, Beattie, Bresnahan apparatus. Please click here to download this File.
