To illustrate the resolution of the data generated from isolated components of the eye, OCR and LPR was measured with three types of tissue (retina, RPE-choroid-sclera, and RPE cells) following a commonly used protocol (the mitochondrial stress test10; Figure 10, Figure 11, and Figure 12). The amount of tissue used for each tissue is shown in Table 1. Data was processed and graphed using the software package that was developed for the fluidics system. The preparation of retina and RPE-choroid-sclera is relatively straight-forward and takes less than 20 min for each tissue type. OCR was constant during the time that test compounds were injected, indicating stable health and function of the tissue and supporting the validity of the method (Figure 10). Once validated for each tissue type, we have not found it necessary to run controls where no test compounds are injected for each experiment. Consistent with data obtained using more conventional perifusion methods6,8,13, OCR decrease in response to oligomycin and increased OCR in response to FCCP. Changes in LPR were in the opposite direction of those observed for OCR: oligomycin increased LPR, which then decreased (but only slightly) in response to FCCP (Figure 11). To compare the statistical significance of the effect of each sequential test compound, t-tests were performed (which are calculated automatically by the software that comes with the instrument). Since the goal of the paper was to describe how to perform the method, the number of replicates carried was not always high enough to produce statistical significance. In general, though, when the number of replicates were 3 or more, effects of FCCP and oligomycin on both OCR and LPR were significant.
RPE cells have not been previously analyzed with flow systems but responded similarly to RPE-choroid-sclera (consistent with the view that a large fraction of OCR is due to RPE cells; Figure 11). These illustrative examples highlight ability of the system to maintain tissue viability as reflected by the stability of OCR in the control channels, and the high signal to noise ratio for changes in OCR of the magnitude induced by oligomycin and FCCP, which was more than 100 to 1. In addition, assays of outflow fractions can be used to correlate the rate of uptake or production of a wide array of compounds exchanging with the extracellular fluid are complementary to OCR (in this case, LPR). These features of the instrument allowed accurate quantification of characteristic differences in tissue responses between tissue types performed in parallel. OCR by RPE-choroid-sclera and RPE cells are consistently more sensitive to oligomycin than retina (Figure 11 and Figure 12), although for the RPE-choroid-sclera the duration of exposure to FCCP was not long enough to reach steady state. A point to consider arose when using DMSO as a solvent. At higher concentrations, (0.2%) DMSO had a transient effect on OCR by retina (presumably reflecting an effect of a change in osmotic pressure brought about by DMSO's effect on membrane permeability).
Based on the assumption that KCN completely inhibits respiration by its direct action on cytochrome c oxidase, OCR at the end of the KCN exposure is set to 0 and all OCR values are calculated based on the change relative to the KCN value. OCR can occur independent of the respiratory chain and cytochrome c oxidase. However, the magnitude of this contribution to overall OCR is generally not more than a few percent (data not shown) and the extended length of time that tissue is exposed to KCN ensures that substrates of oxidases that are not part of the electron transport chain have been depleted.
Statistical analysis
Single experiments were shown as indicated in the figures, but with multiple channels that were averaged. Data was then graphed as the average ± the standard error (SE; calculated as SD/√n).
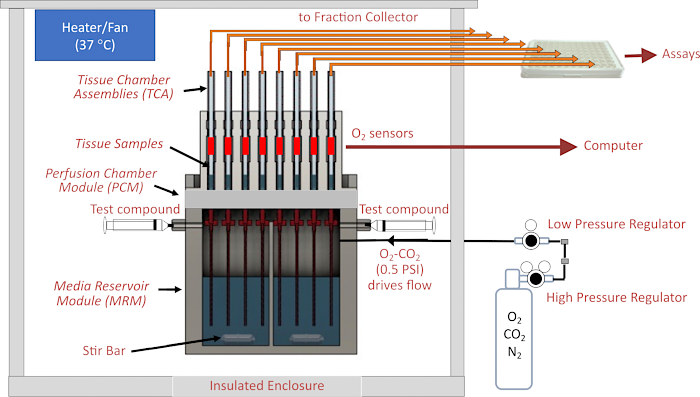
Figure 1. Schematic of the fluidics/assessment system. Major components include the enclosure, temperature control elements, fluidics and tissue chamber systems, regulation of gas pressure in the head space above perifusate, fraction collector/flow rate monitoring, and O2 detectors. Abbreviations: MRM = Media Reservoir Module, PCM = Perifusion Chamber Module, TCA= Tissue Chamber Assemblies. Please click here to view a larger version of this figure.
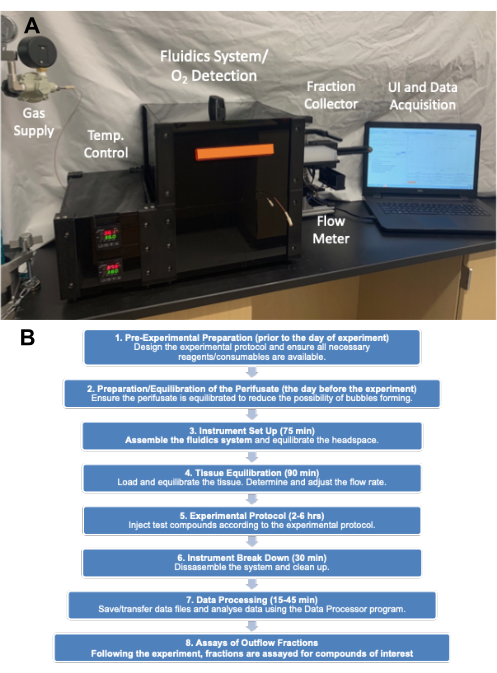
Figure 2. (A) Picture of the major components of the instrument. The major components consist of gas tank (pressure regulators), enclosure, fraction collector and computer. (B) Experimental flow chart showing the major categories of steps and the time it takes to complete them. Please click here to view a larger version of this figure.
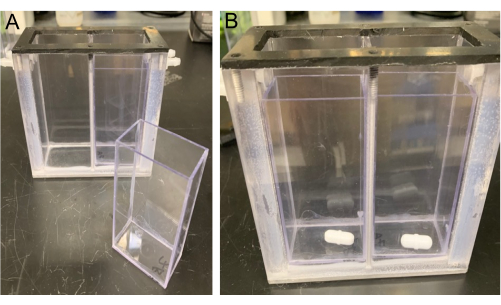
Figure 3. View of the MRM. The MRM is shown with an MRM insert (left) and stir bars (right) placed into the bottom of the MRM inserts (placed in each side of the MRM Divider). Please click here to view a larger version of this figure.
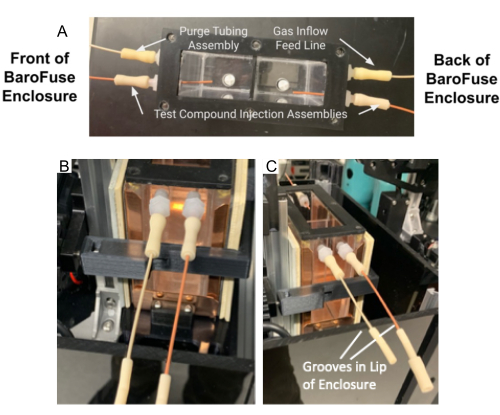
Figure 4. Tubing assembly and purge tubing assembly in the MRM. (A) Test compound injection tubing assembly and purge tubing assembly attached to ports on the MRM. (B–C) The test compound injection assembly and purge tubing assembly (B) are placed in the groove in the front of Enclosure (C). Please click here to view a larger version of this figure.

Figure 5. Powering up the MRM temperature controller. Please click here to view a larger version of this figure.
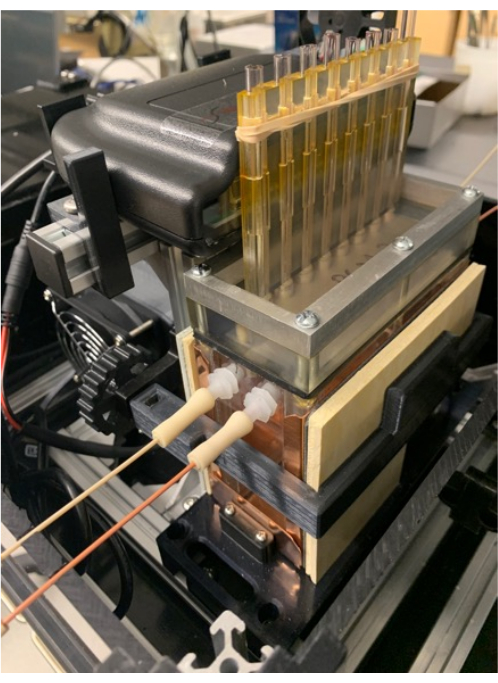
Figure 6. Tissue chambers and gas tank. Positioning the O2 detector on the detector stand (which also supports the MRM and PCM), and placement of the band around the fins of the PCM that help secure the tissue chambers in place. Please click here to view a larger version of this figure.
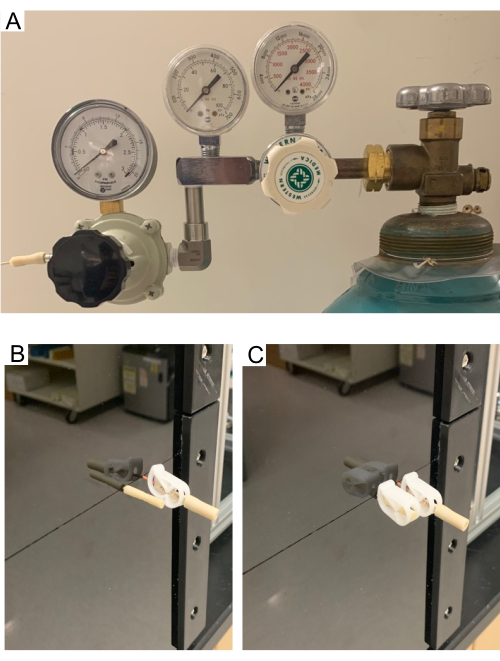
Figure 7. (A) High- and low-pressure regulators on the gas tank. (B–C) Purge tube. Purge tube allows the headspace in the MRM to clear of air and fill with gas from the supply tank. Pictures showing open purge tube (B) and close purge tube (C). Test compound injection assembly stays closed through the purge process. Please click here to view a larger version of this figure.
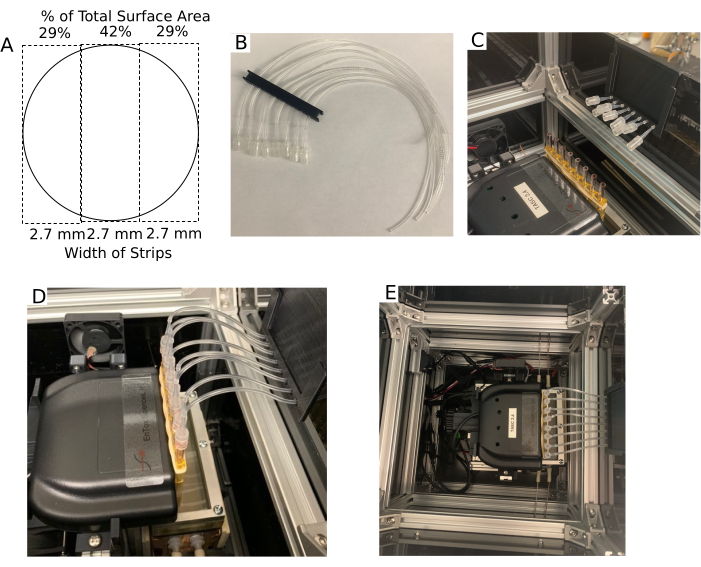
Figure 8. Tissue chamber and the outflow setup. (A) Dimensions of the Transwell membrane after it is cut into three strips of equal width. (B) Outflow multi-tube support. (C) Outflow multi-tube support positioned on the lip of the enclosure with the tubing adapters near the tissue chambers. (D) Picture of outflow tubing assemblies attached to the tissue chambers. (E) Aerial view of the enclosure without the Lid. Please click here to view a larger version of this figure.
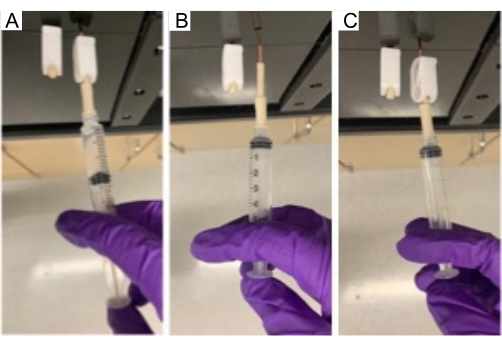
Figure 9. Injection of compound in MRM. Injecting a test compound through the injection port into the MRM using a 5 mL syringe. Please click here to view a larger version of this figure.
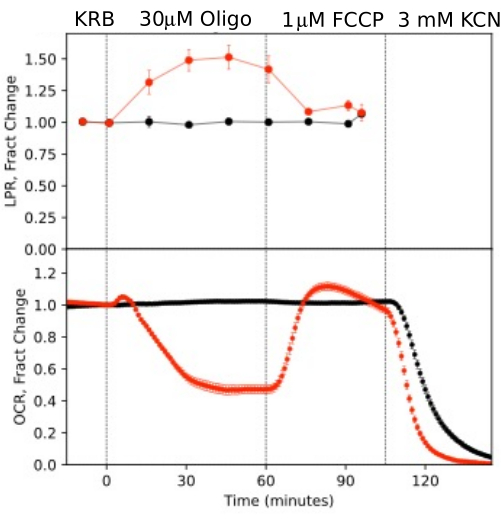
Figure 10. OCR and LPR curves in response to test compounds. OCR and LPR by retina isolated from mice (1 retina/channel) in response to the presence or absence (control) of test compounds as indicated. Each curve is the average of 6 replicates from a single experiment (error bars are SE; p-values are calculated by performing paired t-tests comparing steady state values for each test agent with that of the previous test agent). Please click here to view a larger version of this figure.
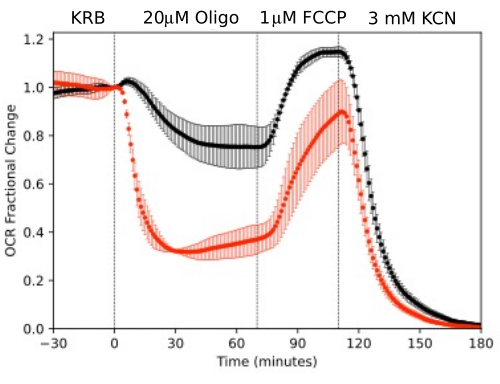
Figure 11. OCR curves. OCR by RPE-choroid-sclera and retina isolated from mice (1 retina or 2 RPE-choroid-sclera/channel) measured in parallel in response to test compounds as indicated. Data is the average of replicates from a single experiment (n = 2 and 4 for RPE-choroid-sclera and retina respectively; p-values are calculated by performing paired t-tests comparing steady state values for each test agent with that of the previous test agent). Please click here to view a larger version of this figure.
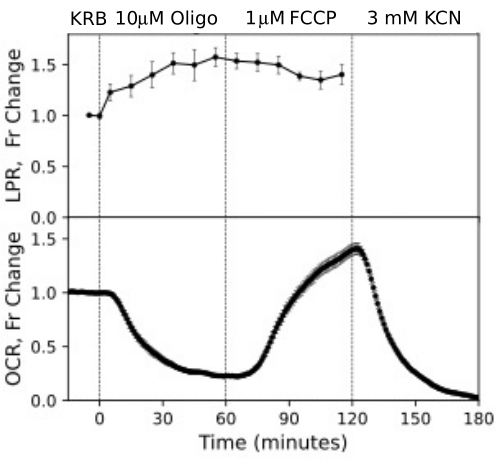
Figure 12. OCR and LPR curves from RPE cells. OCR and LPR from RPE cells attached to transwell membranes that were cut into strips and loaded into the perifusion chambers. Data is the average of replicates from a single experiment (n = 3, with 1.5 membranes/channel (360,000 cells/channel); p-values are calculated by performing paired t-tests comparing steady state values for each test agent with that of the previous test agent). Please click here to view a larger version of this figure.
| TISSUE/CELL | Amount/Channel | FLOW RATE: mL/min |
| Retina (mouse) | 1 | 0.025 |
| RPE-choroid-sclera (mouse) | 2 | 0.02 |
| RPE Cells on Transwell Membranes | 360,000 Cells (4 x 1/3 filter strips) | 0.016 |
Table 1. Recommended operating specifications for different tissue.
Supplementary Figure 1. Graphical representation of experimental design. Timing and composition of exposure to test compounds, and timing of fraction collection. Concentration increment (Conc Inc) is the change in concentration to be implemented. Please click here to download this File.
Supplementary Figure 2. User interface at startup. UI of the startup window of the O2 detection software that monitors the O2 in the tissue chambers inserted into the PCM. Please click here to download this File.
Supplementary Figure 3. User interface for experiment settings. UI for entering experimental information (left) and selecting times for collection of outflow fractions (right). Please click here to download this File.
Supplementary Figure 4. User interface of the injection page. Injection page which calculates injection volumes based on desired concentrations of test compound and volume left in the MRM. Please click here to download this File.
Supplementary File 1: Methods for tissue sample preparation. Please click here to download this File.
