All animal work was approved by the University of Rochester Committee on Animal Resources.
1. Preparation of tissue culture media
- Culture all explants in Dulbecco's Modified Eagle Medium (1x DMEM) with 1% v/v penicillin-streptomycin and 200 µM L-ascorbic acid in an incubator at 37 °C and 5% CO2. For the initial 48 h pretreatment, culture each explant in 70 mL of culture media supplemented with 100 nM dexamethasone74. After pretreatment, culture limbs for 7 more days without dexamethasone, changing media every 48-72 h.
NOTE: Addition of serum, such as fetal bovine serum, to the culture media is not advised consistent with recommendations provided by Wunderli, Blache, and Snedeker57. In brief, serum-free conditions better represent the avascular, nutrient-poor tendon microenvironment that exists in vivo. Furthermore, serum supplementation can promote tissue degradation under certain culture conditions75 and stimulate cell proliferation and migration out of tissue, both features of tendon pathology57. - For the unloaded group, culture each explant in 70 mL of media. For the baseline tension and static impingement groups, each platform requires approximately 125 mL of culture media to keep the limb submerged. This volume can vary depending on the positioning of the upper leg in the grips and 3D print parameters, primarily the infill density.
2. Explant dissection and dexamethasone pretreatment
- Euthanize mice via CO2 inhalation and secondary cervical dislocation, or according to institutional guidelines. This protocol utilizes C57BL/6 mice less than 1 year old. Hind limb size will increase with age and may become challenging to fit within the grips.
- Prior to dissection, transfer 70 mL of prewarmed (37 °C) culture media into a 100 mm (diameter) x 25 mm (height) Petri dish in a sterile biological safety cabinet (BSC). Add dexamethasone to achieve 100 nM working concentration.
- Dissections can be carried out on the benchtop using absorbent underpads, working swiftly through the dissection before transferring hind limb explants into the BSC. Assemble the surgical tools required for this dissection which include smooth, straight, fine tip forceps; straight, fine tip forceps with serrated teeth; and straight, sharp, fine scissors.
- For dissection of hind limb explants, place the mouse in a supine position and identify the hip joint. Using fine scissors, make a small (5-10 mm) incision through the skin overlaying the proximal and anterior (cranial) aspect of the upper leg.
- Pull the incision apart to expand, pinch the exposed upper leg using fingers, and carefully pull the skin distally to deglove the hind limb to the level of the ankle. Gently insert one scissor blade under the skin along the dorsal aspect of the foot and make an incision extending to the toes. Continue to pull the skin distally to completely remove.
- Position the mouse to visualize the Achilles tendon insertion onto the posterior (caudal) aspect of the calcaneus, near the ankle. Proximal to the Achilles tendon insertion, the plantaris tendon lies directly adjacent to the medial border of the Achilles tendon and extends distally toward the plantar aspect of the foot, passing over the posterior aspect of the calcaneus.
- To remove the plantaris tendon, carefully insert one tip of the smooth, fine tip forceps between the two tendons and extend the tip medially passing underneath the plantaris tendon. Draw the tip proximally and tear through the plantaris muscle. Using fine tip, serrated forceps, grab the detached proximal end of the plantaris tendon and pull distally to remove.
- At the hip joint, use fine scissors to cut through the pelvis and isolate the hind limb. Use the scissors to pry off the remaining pelvis and expose the femoral head.
- Transfer the hind limb explant to the BSC and into the dish containing cell culture media with dexamethasone. Move the dish into the incubator and pretreat for 48 h.
3. Explant culture and loading platforms
- As the 48 h pretreatment concludes, prewarm sufficient volumes of culture media (section 1). From this point forward, no dexamethasone will be added to culture media. At this time, limbs from the pretreated (day 0) group can be fixed, decalcified, and embedded in paraffin for future sectioning, staining and analysis.
- For the unloaded group, aspirate pretreatment media and transfer explants to fresh Petri dishes, add 70 mL of culture media each, and return to the incubator.
- For the baseline tension and static impingement groups, prepare explant platforms. Cut pieces of sandpaper similar in size to the grip platens. For the static impingement group, cut pieces of braided line approximately 18 inch in length and pre-tie a loose overhand knot halfway along the length of line. Tear pieces of aluminum foil to cover each acrylic bath and spray with 70% ethanol (EtOH). Transfer preparations to the BSC.
- Each platform includes an acrylic bath, base, volume reduction insert, clip, and grips. Each grip includes two platens and three different types of screws including one M5 x 0.8 mm thread x 10 mm long screw that attaches the grips to the base; two M6 x 1 mm thread x 20 mm long screws that extend the platens to clamp the grips; and four M3 x 0.5 mm thread x 14 mm long screws that, in combination with four compression springs, retract the platens to open the grips.
- Place all components into secondary containers capable of capturing all culture media in the event of a leak. Submerge in ≥ 10% bleach solution and soak for at least 1 h. Rinse off bleach solution with tap water (autoclave as needed) and move into the BSC.
NOTE: For troubleshooting contamination, consider autoclaving all tap water or using purified water. See the Discussion for additional tips when addressing contamination. - Use the M3 screws and compression springs to attach platens to the grips, secure the grips to the base using the M5 screw, and insert the M6 screws until they engage the platens. Use double-sided tape to attach sandpaper to the platens, then close the grips to promote adhesion of the sandpaper to the platens. Repeat for all platforms.
- When ready to load a platform, fully open the grips and using forceps, place the upper leg and knee between the platens with the superficial surface of the Achilles tendon facing upward (Figure 1A). Loosely close the grips to gently hold in place.
- Use forceps to grab the exposed femoral head or foot and manipulate the knee flexion angle as you gradually close the grips to secure in place. For the baseline tension group, extend the knee joint as described previously. As the grips tighten with the knee extended, the ankle should naturally extend. For the static impingement group, flex the knee joint between the grips as described previously.
- For the static impingement group, place the overhand knot of the string around the distal paw and tighten. Route the string through a slot in the base located underneath the explant and through the clip hole. Place the base into the acrylic bath and secure the clip to the top edge of the bath (Figure 1A).
- Pull the string to dorsiflex the foot to at least 110° with respect to the tibia and use a permanent marker to mark the string as it exits the clip. Take a photograph of the explant in this position to later quantify dorsiflexion angle (Figure 1A).
- Remove the base and attach the volume reduction insert by sliding along a track on the base. Place the base (now attached to the volume reduction insert) back into the acrylic bath and reposition the clip on the top edge. Pull the string to return to the original dorsiflexion angle using the marked string as a guide and secure the string to the outside of the bath with tape to maintain static dorsiflexion.
- For the baseline tension group, simply place the base with volume reduction insert into the acrylic bath once the explant is positioned between the grips and take a photograph for quantification of dorsiflexion angle.
- Add 125 mL of prewarmed (37 °C) culture media to each platform to submerge explants. Cover the top of the bath with aluminum foil, place in a secondary container, and move into the incubator. Culture for 7 additional days, changing media every 48-72 h.
NOTE: Tape placed across the top of the bath can prevent PLA parts from floating.
4. Fixation, decalcification and paraffin embedding
- Following explant culture, use scissors to trim toenails/distal toes and cut away the upper leg proximal to the Achilles myotendinous junction. Place each trimmed ankle joint into a processing cassette lined with foam biopsy pads. Push the ankle into the cassette corner to position the ankle at approximately 90° dorsiflexion and close the cassette to keep in place.
- Fix for 3 days in 10% neutral buffered formalin (NBF) and decalcify for 2 weeks in 14% ethylenediamenetetraacetic acid (EDTA) dissolved in distilled water (diH2O) with pH adjusted to 7.4-7.6 with glacial acetic acid.
- To remove salts, thoroughly rinse samples three times in both 1x phosphate buffered saline (PBS) followed by diH2O, 5 minutes each. Perform routine sample processing for paraffin histology: dehydrate through a graded series of EtOH, clear in xylene, and infiltrate with paraffin wax. Orient and embed samples in paraffin to obtain sagittal tissue sections through the Achilles tendon in medial-to-lateral progression as described in section 5 below (Figure 1B).
5. Tissue sectioning
- With a microtome, carefully trim into the sample until sections are parallel to the block face. Grossly trim into the ankle from the medial aspect of the joint, stopping before reaching the medial border of the Achilles tendon insertion.
- Transfer the sample to an ice block to adjust temperature and hydration, and change blades (or shift to a fresh section of the current blade). Continue sectioning into the sample at 10 µm thickness and carefully identify entry into the Achilles tendon insertion with a brightfield microscope. Once identified, perform serial sectioning tracking section number (i.e., tissue depth) through the entire Achilles tendon insertion.
6. Deparaffinization/rehydration and slide selection
- For each assay below, select level-matched tissue sections from each pair of contralateral limbs. Prior to staining, place on a slide rack and move through 3 changes of xylene, 2 changes of 100% EtOH, 2 changes of 95% EtOH, and 1 change of 70% EtOH, 5 min each. Finish rehydrating in diH2O.
7. TUNEL to assess Achilles tendon viability
- For TUNEL labeling, stain according to the manufacturer's protocol. Incubate in 20 µg/mL proteinase K for 20 min at room temperature and rinse in diH2O. Incubate in 50 µL of TUNEL stain solution (5 µL enzyme solution, 45 µL label solution) for 1 h at 37 °C. Rinse in diH2O. Mount with antifade reagent containing DAPI and coverslip.
- Image the Achilles tendon insertion using a fluorescence microscope with a 4x objective lens. Include a DAPI channel (excitation/emission wavelengths = 360/460 nm) to visualize all nuclei, a TUNEL (TMR Red) channel (excitation/emission wavelengths = 540/580 nm) to visualize apoptotic nuclei, and if possible, a brightfield channel.
- For image analysis, import images into an image analysis software suitable for ROI-based processing, such as FIJI/ImageJ or MATLAB. Define a region of interest (ROI) outlining the entire Achilles tendon in view (Figure 2A), excluding cells in the epitenon that are highly susceptible to death induced by dissection and sudden change in environmental conditions when placed into culture.
- To do this, perform ROI selection in MATLAB by importing the brightfield image and using the drawpolygon() function to trace and enclose the boundaries of the tendon. MATLAB creates a Polygon object for the ROI, which can then be applied to the DAPI and TUNEL channel images to mask out pixel intensity data outside the ROI using createMask() in order to only analyze nuclei within the Achilles tendon.
- Import the DAPI and TUNEL channel images and identify a fluorescence intensity threshold for defining apoptotic (TUNEL+) nuclei by normalizing to the maximum fluorescence intensity of apoptotic nuclei in nonviable tissues such as bone, muscle or fat that are incidentally captured in the tissue section. Once the images are masked, calculate the fraction of apoptotic nuclei (TUNEL+ nuclei/DAPI nuclei) within the Achilles tendon.
8. Toluidine blue histology to characterize fibrocartilage formation
- Once rehydrated (Section 6), transfer slide rack with level-matched tissue sections from contralateral pairs of explants to 0.4% w/v Toluidine blue O in 0.1 M sodium acetate buffer with pH adjusted to 4.0 using glacial acetic acid. Incubate for 10 min at room temperature, then rinse 3x in diH2O for 30 s each.
- Dehydrate through three changes of 95% EtOH and two changes of 100% EtOH, 30 s each. Clear through three changes of xylene, 1 min each. Coverslip with xylene-based mounting medium.
- Obtain 24-bit Red-Blue-Green (RGB) color images of the Achilles tendon insertion. For example, for this protocol use an adapter to interface a digital color camera to the eyepiece of a simple brightfield microscope with a 4x objective.
- To quantify differences in Toluidine blue staining within the compressive tendon fibrocartilage (CTF)16 at the Achilles tendon insertion (Figure 3A,B), import RGB images into an image analysis software capable of defining and managing multiple ROIs. Options include the selections and ROI manager tools in FIJI/ImageJ or the image processing toolbox in MATLAB. Begin by setting the pixel/length scale.
NOTE: Software choice is left to the discretion of the researcher and is certainly not limited to MATLAB or FIJI/ImageJ. The authors have provided MATLAB code (Supplementary File 2), documentation describing implementation (Supplementary File 3), and a sample image (Supplementary File 4). We encourage researchers to translate this code to alternative programming languages for use in other software as needed or preferred. - With the image displayed in the software of choice, identify the intersection of the deep tendon border with the calcaneus. From here, trace proximally 800 µm along the deep tendon border to establish the deep boundary of the CTF. For example, use the drawpolyline() function in MATLAB to interactively draw a polyline over the RGB image. MATLAB creates a Polyline object containing the vertices of the line, which can be processed and trimmed to a length of 800 µm.
- From this position, create the proximal boundary of the CTF by drawing a line segment connecting to the superficial tendon border that is perpendicular to the local fiber orientation.
- Move back to the intersection of the deep tendon border and the calcaneus and define the distal boundary of the CTF by drawing a line segment connecting to the superficial tendon border along the distinct tidemark separating the CTF from the attachment zone fibrocartilage (AZF)16 (Figure 3A,B). Lastly, generate the superficial boundary of the CTF by tracing the superficial tendon border to enclose.
- To describe spatial variations in GAG staining across the insertion, divide the total CTF into 4 quadrants (Figure 3A,B). Connect the midpoint of the deep and superficial CTF boundaries with a line segment to create a distal/proximal boundary. Passing through the midpoint of this boundary, connect the midpoints of the distal and proximal CTF boundaries along the fiber orientation to create a superficial/deep boundary.
- These 6 boundaries provide information that can be used to define the ROI representing the entire CTF, but also 4 quadrants subdividing the CTF. In MATLAB, for example, compile vertices defining the boundaries of each individual ROI (CTF, quadrants 1-4) into vectors and use images.roi.Polygon() to generate enclosed Polygon objects for each ROI.
- With ROIs defined, transform RGB pixel data into the Hue-Saturation-Value (HSV) color space using the color transformer plugin in FIJI, the rgb2hsv() function in MATLAB, or other software applying the appropriate transformation equations76. HSV data can then be projected into the 2D hue-saturation space, where each combination of hue and saturation encode a unique color (Figure 3C).
- Within each ROI, calculate the average hue and saturation that describe the average stain color in the ROI. This can be achieved in MATLAB, for example, by using the Polygon objects defining each ROI to mask the image using createMask() in order to analyze hue-saturation pixel data specifically within each ROI.
- Define another small ROI within the periosteal fibrocartilage (PF)16 (Figure 3A, B) and calculate average hue and saturation. Then, calculate the Euclidean distance separating the average color in each ROI of the CTF to that of the PF (Figure 3C).

NOTE: The Euclidean distance calculation describes the degree of similarity between the average color of the ROI to that of the PF, a quintessential fibrocartilaginous tissue16,17,77. A smaller Euclidean distance indicates a ROI color that is more fibrocartilaginous in appearance. - Use this distance to calculate fibrocartilage score, which assumes a maximum value of 1 if the ROI color is identical to the PF color and a minimum value of -1 if the ROI and PF color reach maximum separation within the hue-saturation color space.

- Average data for hue, saturation, and fibrocartilage score within each ROI across tissue sections from each limb. Perform paired statistical comparisons between groups of contralateral limbs.
9. SHG imaging to investigate change in collagen network organization
- Perform SHG imaging of the Toluidine blue stained sections using a capable microscope system with a 20x object lens. Acquire z-stacks through the section thickness and perform tile scanning as needed to fully capture the Achilles tendon insertion.
- Import SHG images into a preferred image analysis software and define ROIs encompassing and subdividing the CTF at the Achilles tendon insertion as described for the Toluidine blue image analysis in section 8 (Figure 4A,B).
- If SHG images are imported into MATLAB, use the approach for defining CTF ROIs in MATLAB as outlined in section 8 . After defining ROIs, transfer ROI coordinates into FIJI by exporting ROI vertices from MATLAB as .txt files and importing into FIJI using File > Import > XY Coordinates. Overlay the selection and send to the ROI manager for analysis.
- To quantify collagen organization, use the Directionality plugin in FIJI, which performs Fourier spectrum analysis to calculate distributions of fiber orientations across small windows spanning a ROI. The spread of this distribution, referred to as dispersion, is inversely related to fiber alignment.
NOTE: Collagen fibers may assume variable orientations in different windows across the CTF due to gross curvature of the tendon rather than the absence of alignment/organization. To better distinguish changes in collagen organization from gross curvature of the tendon at the insertion, it is necessary to define smaller ROIs. - Import SHG images into FIJI and set the pixel/length scale. Project maximum pixel intensity data into a 2D composite image and add ROIs to the ROI Manager. Sequentially overlay each CTF ROI onto the image and draw 10 small sub-ROIs of consistent size within the ROI, adding the sub-ROIs to the ROI manager.
- Within each sub-ROI, run the directionality plugin in FIJI to calculate fiber dispersion. Average dispersion data across sub-ROIs within each CTF ROI, and average dispersion data within each CTF ROI across sections from each explant. Perform paired statistical comparisons between groups of contralateral limbs.
Representative images of TUNEL stained tissue sections demonstrate minimal apoptotic nuclei within the body of the Achilles tendon after 7 days of explant culture across experimental groups (Figure 2A). Quantification of these images provides evidence that the tissue culture protocol maintains up to 78% viability on average within the Achilles tendon after 7 days of explant culture across loading conditions (Figure 2B).
Qualitatively, enhanced Toluidine blue staining is appreciated after 7 days of static impingement compared to unloaded controls (Figure 3A,B), particularly in deep quadrants adjacent to the calcaneus where we have previously measured maximum transverse compressive strain5,6. Quantification of these Toluidine blue stained tissue sections indicates significant change in hue (Figure 3D), saturation (Figure 3E), and fibrocartilage score (Figure 3F) after 7 days of static impingement compared to contralateral unloaded explants. This altered GAG staining likely represents fibrocartilage formation secondary to static impingement within this model. Statistically significant differences in saturation and fibrocartilage score were only detected in quadrant 1 after 7 days of baseline tension (Figure 3E,F). Moreover, saturation and fibrocartilage score decreased relative to contralateral unloaded tendons, an opposite trend compared to static impingement. This data may support the hypothesis that tensile loading can attenuate or reverse impingement-driven fibrocartilage formation and warrants additional investigation in the future.
Quantification of SHG imaging suggests subtle but significant change in collagen fiber orientation after 7 days of static impingement, again in the deep and distal region adjacent to the calcaneus, as indicated by significant differences in dispersion (Figure 4C).
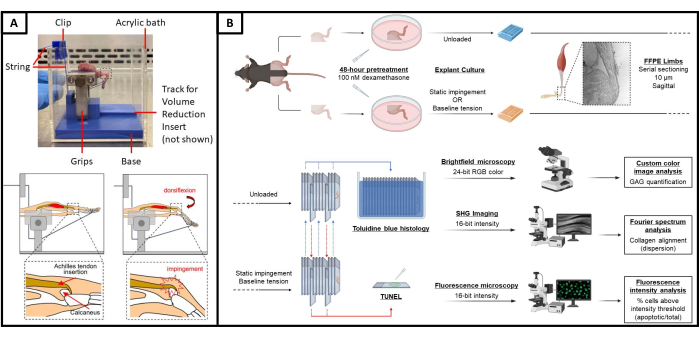
Figure 1: Explant platform and experimental design. (A) Photographic and schematic representation of the explant platform. (Top) Photograph of a whole murine hind limb explant loaded into the platform, with critical components labeled. (Bottom) Schematic depicting insertional Achilles tendon impingement elicited by passively applied ankle dorsiflexion in this explant model. (B) Schematic of study design and explant culture. Hind limb explants are pretreated in 100 nM dexamethasone for 48 h74. From each mouse, one hind limb explant is then cultured in a dish unloaded for 7 days, while the contralateral limb is loaded into the experimental platform to place the Achilles tendon under either baseline tension or static impingement for 7 days. Serial tissue sections from contralateral pairs of limbs are either stained with Toluidine blue to visualize GAG-rich tissue or used for TUNEL staining. Toluidine blue stained sections are then used for SHG imaging to assess collagen organization. Please click here to view a larger version of this figure.
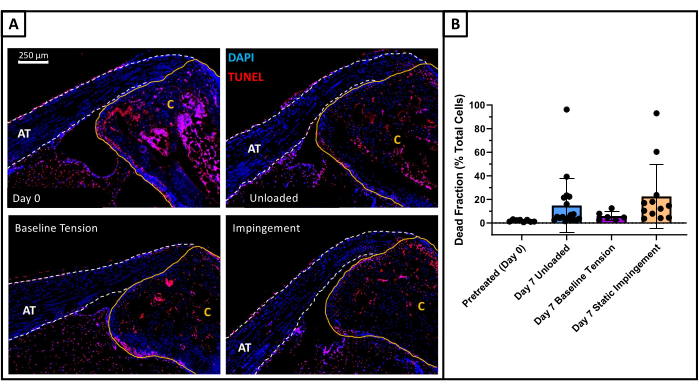
Figure 2: Explant viability. (A) Representative images of TUNEL stained sections from pretreated (day 0) explants (top left), unloaded tendons (top right), tendons maintained at baseline tension (bottom left), and statically impinged tendons (bottom right). The Achilles tendon is outlined in a dashed white line and labeled AT, while the calcaneus is outlined in a solid yellow line and labeled C. Apoptotic nuclei appear red (TUNEL), all nuclei appear blue (DAPI). (B) Quantification of dead cell fraction was on average less than 22% for the unloaded, baseline tension, and static impingement groups. Data represents mean ± standard deviation. Outliers are present in these data sets with greater than 50% cell death, which may be attributed to tendon damage induced by poor dissection technique. The average dead cell fraction with statistical outliers removed is less than 15% for all groups. No statistically significant difference in cell death was found between unloaded, baseline tension and static impingement groups (p < 0.05). Day 0 control: n=8. Unloaded: n=18. Baseline Tension: n=8. Static Impingement: n=12. Please click here to view a larger version of this figure.
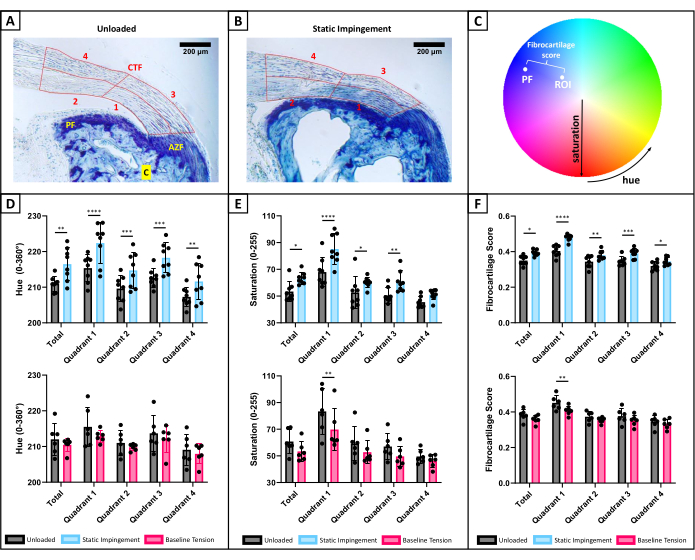
Figure 3: Toluidine blue histology. (A) Representative Toluidine blue stain after 7 days of unloaded culture depicting the compressive tendon fibrocartilage (CTF), attachment zone fibrocartilage (AZF), and periosteal fibrocartilage (PF) at the Achilles insertion16. Calcaneus labeled C. ROI capturing the CTF is outlined in red and is further subdivided into 4 quadrants to provide additional spatial information. (B) Representative Toluidine blue stain after 7 days of static impingement, with enhanced staining of the CTF, especially in quadrant 1 where we have previously measured maximum transverse compressive strains5,6. (C) Schematic of the hue-saturation color space used for color image analysis. Color is described by a combination of hue (0°-360°) and saturation (0-255)76. The average color in each ROI is normalized to the average color of the PF by calculating Euclidean distance separating colors in each ROI from the color in the PF, which provides a normalized fibrocartilage score. (D-F) Changes in Toluidine blue stain after 7 days of static impingement (top) and baseline tension (bottom) compared to contralateral unloaded tendons. Data represents mean ± standard deviation. (D) Quantification of hue indicates significant differences in average hue across all regions after 7 days of static impingement compared to contralateral unloaded tendons. No similar trend was detected after 7 days of baseline tension compared to contralateral unloaded tendons. (E) Quantification of saturation, with significant changes in average saturation across the entire CTF and within quadrants 1-3 after 7 days of static impingement compared to contralateral unloaded tendons. Conversely, significant differences were only detected in quadrant 1 after 7 days of baseline tension, where saturation decreased compared to contralateral unloaded tendons. (F) Quantification of fibrocartilage score, with significant changes in fibrocartilage score across all regions after 7 days of static impingement compared to contralateral unloaded tendons. Conversely, significant differences were only detected in quadrant 1 after 7 days of baseline tension, where fibrocartilage score decreased compared to contralateral unloaded tendons. The data suggest enhanced GAG stain brought about by static impingement indicative of increased fibrocartilage formation. Data describing the total CTF were compared using Wilcoxon matched-pairs signed rank tests. Quadrant data were compared using repeated measures two-way ANOVA with Šídák's multiple comparisons test. *p < 0.05. **p < 0.01. ***p < 0.005. ****p < 0.001. Baseline Tension vs. Unloaded: n = 6 pairs. Static Impingement vs. Unloaded: n = 8 pairs. Please click here to view a larger version of this figure.
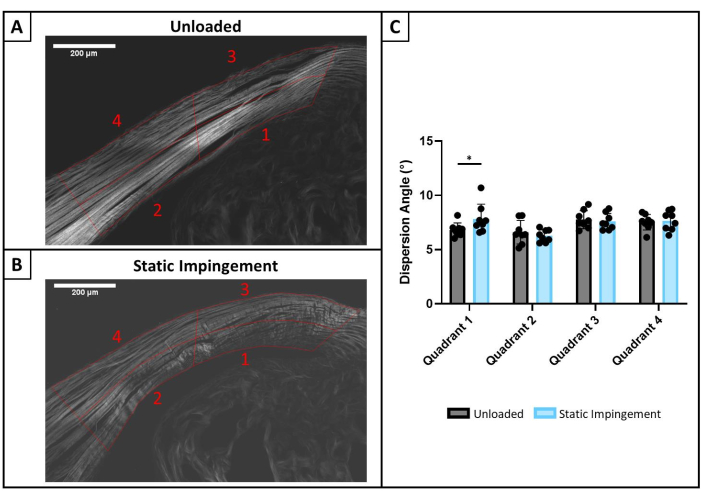
Figure 4: SHG imaging. (A) Representative SHG image after 7 days of unloaded culture compared to (B) 7 days of static impingement. CTF is outlined in red and divided into 4 quadrants as labeled, consistent with ROIs in Toluidine blue analysis above. (C) Within each quadrant, Fourier spectrum analysis was performed in a moving sub-window using the Directionality plugin in FIJI. The spread of the distribution of fiber orientations within each sub-window is termed dispersion (°) and is inversely related to fiber alignment. Dispersion = 0° represents perfect parallel alignment of fibers. Increasing dispersion represents decreasing collagen fiber alignment. Data represent mean ± standard deviation. Statistically significant differences in dispersion were detected in quadrant 1 following 7 days of static impingement compared to contralateral unloaded tendons, suggesting increased collagen disorganization. Quadrant data were compared using repeated measures two-way ANOVA with Šídák's multiple comparisons test. * p < 0.05. Static Impingement vs Unloaded: n = 5 pairs. Please click here to view a larger version of this figure.
Supplementary File 1: CAD files. These CAD files, compiled in multiple file formats, can be used to 3D print the platform base, volume reduction insert, and clip. Please click here to download this File.
Supplementary File 2: MATLAB files. The compiled MATLAB files allow for quantification of Toluidine blue histology as described in section 8 of the protocol to assess fibrocartilage formation through spatial change in GAG staining at the Achilles tendon insertion. Please click here to download this File.
Supplementary File 3: Guidelines for implementing MATLAB code. This document describes a pipeline for quantifying changes in GAG staining at the Achilles tendon insertion via image analysis of Toluidine blue histology using the provided MATLAB code. Please click here to download this File.
Supplementary File 4: Sample image of Toluidine blue histology. This RGB color image of Toluidine blue histology can be used to execute the provided MATLAB code. Please click here to download this File.
