Understanding the requirements for successful CSF-CTCs growth ex vivo is an ongoing effort. To that end, it is believed that providing essential factors that mimic the CSF microenvironment is of key importance22. Human meningeal cells (HMCs) secrete a variety of growth factors into the CSF, including FGF-2, EGF, IGFBP2, and IGFBP6, and are known to support the growth of CTC cells12,13,14,23,24. Therefore, a human cytokine array analysis was performed on HMC-conditioned media to identify potentially important components required for CTC survival. Indeed, several growth factors were upregulated in the media cultured with HMCs (Figure 3A). For example, granulocyte-macrophage colony-stimulating factor (GM-CSF), VEGF-A, and IGFBPs (IGFBP2, 3, 4, and 6).
The CSF-cellular components from patients may consist of multiple cell types, such as CTCs, immune cells, and fibroblasts. Non-CTCs will eventually stop passaging overtime. Generally, cells that propagate successfully and remain in proliferation are cancer (M-LMD) cells. Validation of growing cells in culture is indeed M-LMD cells, which can be done by IF detection of MLANA expression and transcriptomic analyses, which have previously been shown7.
As a proof of concept to show the potential use and application of established in vitro and in vivo PD-CSF-CTC lines, single-cell RNA-sequencing (scRNA-seq) analysis was used, and the results revealed several genes that were enriched and retained from the uncultured patient CSF-CTCs7. Two of them include receptor tyrosine-protein kinase ErbB3 and IGF-1R, which have implications on melanoma progression and chemotherapy resistance25,26,27.
To test whether they played a role in CSF-CTC survival, a crystal violet proliferation assay was conducted on PD-CSF-CTCs treated with FDA-approved drugs tucatinib and ceritinib that target ErbB28 and IGF-1R7,29 respectively. Anti-IGFBP2 antibody was included as a positive control that should hinder the growth of PD-CSF-CTC cultures. The results showed that the absence of IGFBP2 or IGF-1R was effective in reducing the proliferation of PD-CSF-CTCs (Figure 3B). Given that MAPK signaling is downstream of IGF-1R, calcein-AM live cell staining and MTT cell survival assays were also performed in three M-LMD PD-CSF-CTC lines by treating them with ceritinib or the MAPK inhibitors, dabrafenib and trametinib or a combination of all three. The data demonstrated that the viability of all three cell lines was significantly reduced by ceritinib, whereas dabrafenib and trametinib had mixed effects (Figure 3C). The result from debrafenib and trametinib treatments was surprising. All three PD-CSF-CTC lines were derived from M-LMD patients that harbored a BRAFV600E mutation7. This may suggest an acquired chemo-resistance effect of CSF-CTCs, which is something to be investigated in the future.
Next, as an example of how PD-CSF-CTCs can be utilized in vivo, murine-M-LMD models were established by intrathecally inoculated with varying numbers of PD-CSF-CTCs. The median survival times in mice were determined (Figure 3D). To visualize M-LMD progression, PD-CSF-CTC lines were tagged with a bioluminescent marker, such as the NL reporter system21, and captured by BLI (Figure 2C). The location of the LMD metastases was also demonstrated using immunohistochemistry with protein melan-A (MLANA)30 as a marker of the melanoma cells (Figure 3E). As a proof of concept to test therapeutic strategies against M-LMD in vivo, murine-M-LMD cohorts were given daily oral monotherapy of ceritinib or trametinib, or a combination of dabrafenib and trametinib or ceritinib and trametinib. The control (untreated) cohort received oral saline as a comparison. The results showed a significantly prolonged survival (Figure 3F) and delayed disease detection (Figure 3G) in the cohort that was treated with ceritinib and trametinib (untreated M-LMD median survival: 28.5 days vs. ceritinib and trametinib treated M-LMD median survival: 38.5 days; P value = 0.0052). These data underscore the potential usefulness of the developed M-LMD PD-CSF-CTC lines for conducting preclinical studies to determine the efficacy of novel therapeutics.
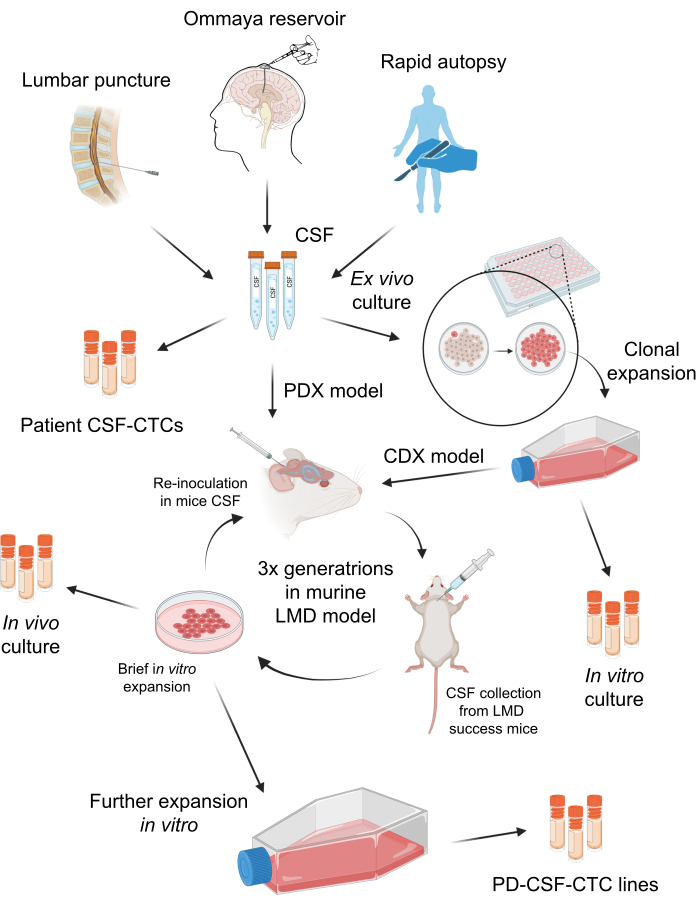
Figure 1: A schematic overview of the process of establishing patient-derived CSF-circulating tumor cells (PD-CSF-CTCs). CSF from patients can be sampled via lumbar puncture, Ommaya reservoir, or rapid autopsies. Through a series of in vitro and in vivo propagations, each step generates an intermediate CSF-CTC culture (i.e., patient CSF-CTCs, in vitro culture, in vivo culture) until establishing a PD-CSF-CTC line. Please click here to view a larger version of this figure.
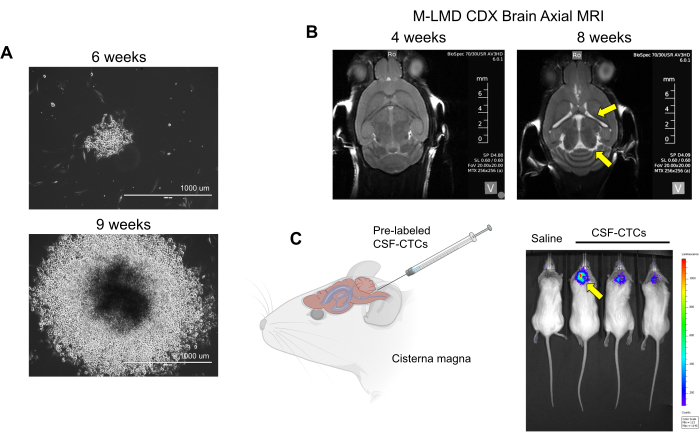
Figure 2: Examples of in vitro and in vivo culturing of CSF-CTCs derived from M-LMD patients. (A) Representative brightfield images showing the in vitro growth of an M-LMD CSF-CTC colony at 6 weeks and 9 weeks in HMC-conditioned media. Scale bar: 1000 µm. (B) MRI images at 4 weeks and 8 weeks after intrathecally inoculated with PD-CSF-CTCs; a successful establishment of a murine model of M-LMD. Yellow arrows point to enlarged ventricles and possible hydrocephaly in this M-LMD mouse. (C) Representative BLI visualization of M-LMD development in mice. The figure is adapted from Law et al.7. Please click here to view a larger version of this figure.
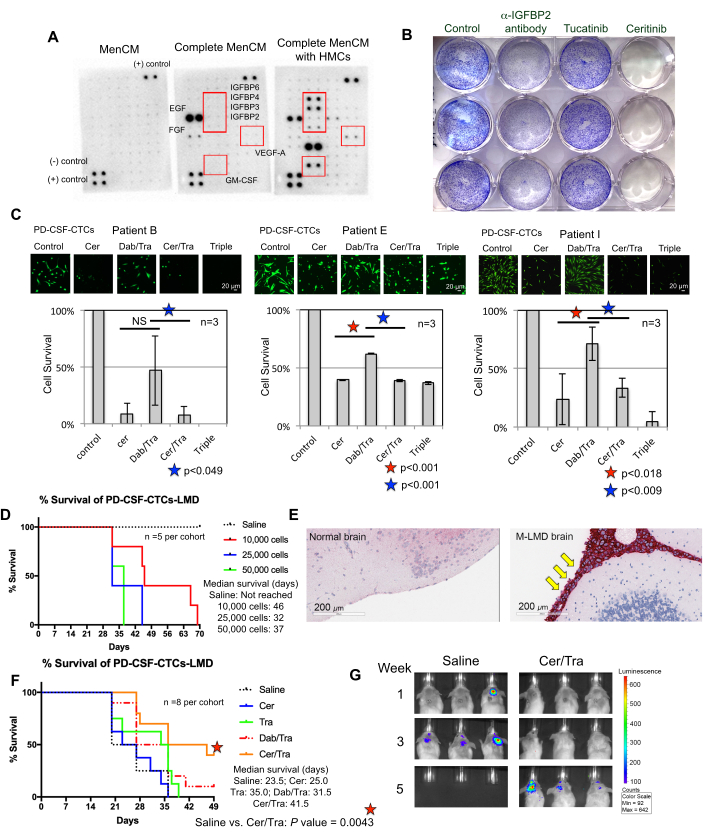
Figure 3: PD-CSF-CTC lines are used in various preclinical experiments to study M-LMD. (A) A human cytokine array showing an increase of different secreted growth factors (i.e., IGFBPs, VEGF-A, and GM-CSF) in culture media (MenCM) in the presence of human meningeal cells (HMCs). (B) A scanned image of a crystal violet cell proliferation assay to determine the efficacy of anti-IGFBP2 antibody, tucatinib, and ceritinib against one of the PD-CSF-CTC lines. The control condition was given vehicle treatment. The experiment was performed in triplicate. (C) Cell survival assay of three different established PD-CSF-CTC lines (from patients 09, 12, and 16) in vitro. Cells were treated with either ceritinib (cer), a combination of dabrafenib (dab) + trametinib (tra), cer + tra, or all three. Cells were collected at 72 h after treatment. Calcein-AM staining was used to visualize cell viability, and an MTT assay was used to determine cell survival. A paired sample t-test was used for statistical analysis. Scale bars: 20 µm. (D) A survival curve of a murine M-LMD model. NSG mice were inoculated intrathecally (via the cisterna magna) with one of the PD-CSF-CTC lines at 10,000, 20,000, and 50,000 cells. The median survival of M-LMD mice was determined. (E) IHC detection for MLANA, a marker for melanoma, in the brain sections of M-LMD mice. Positive MLANA was found in the meninges (stained in red; pointed by yellow arrows), whereas the normal (healthy) brain did not show cancer growth (negative for MLANA). Scale bars: 200 µm. (F) A representative efficacy experiment of murine M-LMD cohorts given either daily oral saline, cer, tra, dab/tra or cer/tra. Survival of mice was determined. The log-rank (Mantel-Cox) test was used for statistical analysis. (G) Representative BLI images of M-LMD progression in 5 weeks, comparing control (saline) treated vs. cer/tra treated murine M-LMD cohorts. Panel (C) of the figure is adapted from Law et al.7. Please click here to view a larger version of this figure.
Table 1: Summary of clinical CSF-CTCs obtained for ex vivo culture in M-LMD patients. A summary table of 11 M-LMD patients, which their CSF-CTCs have been attempted to propagate. The patients in the Table were previously characterized in Law et al.7. Please click here to download this Table.
