A total of six patients received this surgical treatment (Table 1). Preoperatively, all patients were assessed based on PaO2/FiO2, systolic blood pressure, and creatinine levels and were assigned modified Marshall score10 and APACHE II scores (Table 2). All patients underwent surgery smoothly, and the duration of surgery ranged from 75 to 100 min, with an average of 84 ± 6.7 min. Preoperative bacterial cultures obtained through PCD tubes revealed Escherichia coli, Enterococcus faecalis, Pseudomonas aeruginosa, Burkholderia cepacia, and Acinetobacter baumannii. Postoperatively, systemic toxicity symptoms rapidly improved, and CT scans performed 1 week later showed a substantial reduction in necrotic tissue and peripancreatic fluid accumulation (Figure 4). Preoperatively, the blood white blood cell count, neutrophil ratio, and PCT were elevated in all six patients, and their values significantly decreased 1 week after surgery. Four patients had elevated blood amylase levels preoperatively, and 1 week after surgery, all patients had normal levels (Table 3).
A single patient experienced recurrent high fever without resolution at 2 weeks post-surgery, with unobstructed drainage. Repeat CT indicated increased peripancreatic necrosis and fluid compared to observations 1 week earlier. A repeat laparoscopic procedure was performed on the right side with the patient in the left lateral position using the same technique as the initial left-sided retroperitoneoscopic surgery. Symptoms were rapidly ameliorated after the second surgery. Complications occurred in two patients. One patient developed a fever shortly after surgery and exhibited drainage fluid containing yellowish fluid with fecal-like debris after 2 weeks. Considering the possibility of a colonic fistula, conservative treatment was initiated for 1 week. Since the drainage fluid still contained fecal-like material (approximately 10-50 mL daily), the patient underwent subsequent surgery for terminal ileostomy, after which the drainage fluid gradually cleared. Another patient exhibited bloody drainage through the drainage tube 1 week post-surgery, accompanied by progressively decreasing hemoglobin levels in blood tests, indicating intraperitoneal bleeding. The patient received transfusions of red blood cells, fresh frozen plasma, and cryoprecipitate, followed by enhanced hemostatic treatment, which successfully stopped further bleeding. The other four patients experienced no postoperative complications.
During the 1-year follow-up period, all patients achieved satisfactory clinical outcomes, with almost complete disappearance of the peripancreatic fluid and necrotic tissue.

Figure 1: Preoperative CT scan. The preoperative CT scan shows abundant peripancreatic fluid accumulation and necrotic tissue. Please click here to view a larger version of this figure.
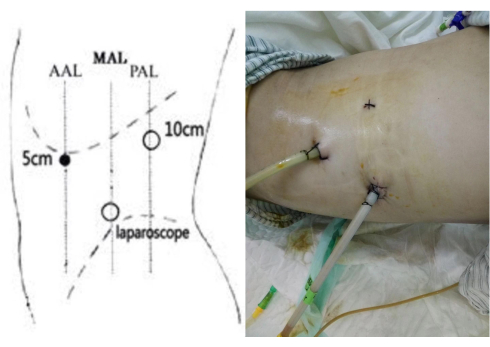
Figure 2: Trocar set up. Three-port arrangement of trocars in the retroperitoneoscopic adrenal surgery procedure and the postoperative placement of drainage tubes. Please click here to view a larger version of this figure.
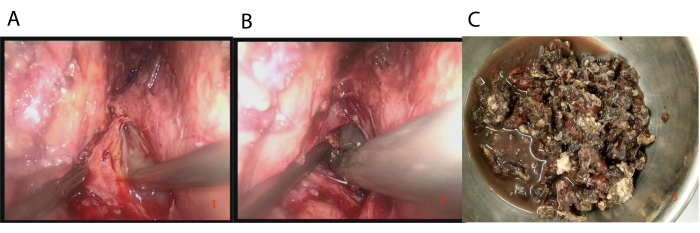
Figure 3: Surgical procedure. (A) Pus was discovered immediately after the aspirator entered the preperitoneal space adjacent to the kidney. (B) Careful extraction of black necrotic tissue using tissue forceps. (C) Excised pancreatic necrotic tissue during surgery. Please click here to view a larger version of this figure.
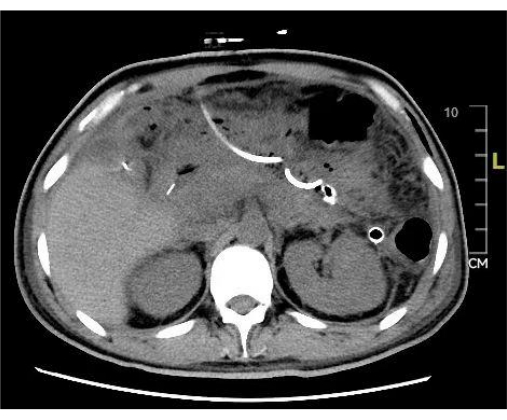
Figure 4: Postoperative CT scan. The postoperative CT scan shows a significant reduction in peripancreatic fluid accumulation and necrotic tissue after surgery. Please click here to view a larger version of this figure.
Table 1: Clinical data showing identified bacterial strains in patients receiving surgical treatment. Please click here to download this Table.
Table 2: APACHE II scores for patients. Please click here to download this Table.
Table 3: Clinical parameters of patients receiving surgical treatment before and after treatment. Please click here to download this Table.
