All procedures were approved and conducted in compliance with the guidelines established by the Institutional Animal Care and Use Committee at the University of Missouri. Experiments were performed on adult male Sprague-Dawley rats, aged 11 to 15 weeks. These rats were housed in pairs and kept under a 12:12 light-dark cycle, with access to standard commercial pelleted food and water available at all times.
1. Animal preparation and anesthesia delivery
- Wear suitable personal protection equipment while handling rats.
- Administer inhalation anesthetic with 3-5% isoflurane, ensuring proper induction. Once the rat is adequately anesthetized, place it in a supine position and maintain the anesthesia with 1-3% inhaled isoflurane. Check the sufficiency of the anesthesia depth by gently applying pressure to the hindlimb footpad using forceps to ensure there is no withdrawal response.
NOTE: Based on the rat's size and weight, monitor the depth of anesthesia, and adjust the isoflurane concentration accordingly. - Maintain the temperature of 37 °C using a thermostatic warming plate to prevent variations in temperature that can impact CMAP amplitude and latency.
- Apply a veterinary petroleum-based ointment to the eyes to prevent dryness. Monitor the depth of anesthesia by observing the respiration rate and checking for withdrawal responses upon applying pressure to the footpad with forceps.
- Remove hair from the lower third of the chest and neck to be studied using clippers. Monitor the respiration of the rat during the entire experiment.
NOTE: Following the CMAP and MUNE recordings and discontinuation of anesthesia, do not leave the rat unattended until it has regained sufficient consciousness. Do not return the animal to the home cage until fully recovered.
2. Electrode placement and setup
- Place a pair of 28 G monopolar needle electrodes to record the CMAP, SMUP, and MUNE as depicted in Figure 1.
- Place the active (E1) needle electrode subcutaneously over the mid clavicular line inferior to the last rib border, and the reference (E2) needle electrode subcutaneously in the angle between the xyphoid process and last sternocostal cartilage.
NOTE: The needle electrodes should not be inserted into the diaphragm muscle; instead, they should be positioned in the subcutaneous area.
- Place the active (E1) needle electrode subcutaneously over the mid clavicular line inferior to the last rib border, and the reference (E2) needle electrode subcutaneously in the angle between the xyphoid process and last sternocostal cartilage.
- For stimulation of the phrenic nerve at the carotid sheet, use a pair of 28 G monopolar needle electrodes as the cathode and anode for nerve stimulation and placed subcutaneously over the lateral neck between the anterior and middle scalene muscles, separated by approximately 1 cm. Ensure that the placement of the stimulating needles is at the level below the fourth cervical vertebrae (C4).
NOTE: Avoid inserting the stimulating electrodes too deep to avoid injury of the phrenic nerve or other structure. Figure 1 illustrates electrode placement. - For the ground electrode, place a disposable surface electrode on the tail.
3. Data acquisition
- Phrenic CMAP
- Record phrenic CMAP responses by applying monophasic cathodic square-wave pulses with a duration of 0.1 ms and intensity ranging from 60 to 100 mA to stimulate the phrenic nerve.
- Obtain CMAP responses while progressively increasing the stimulus intensity until the amplitude of the response ceases to show any further increase. To ensure supramaximal stimulation, raise the stimulus intensity to approximately 120% of the level used to elicit a maximal response, and record an additional response. If the CMAP size no longer increases, consider this response as the maximum CMAP.
NOTE: Delivering stimulation during exhalation is preferable to minimize concurrent muscle activity noise during CMAP recording. - Measure and document the peak-to-peak amplitudes of the CMAP in millivolts (mV) (Figure 2).
NOTE: CMAP amplitude can be assessed base-to-peak and peak-to-peak. Clinical electrodiagnostic systems are often defaulted to assess base-to-peak which is calculated from the isoelectric baseline to the initial negative peak.
- Average single motor unit potential (SMUP) size and MUNE calculation
- Calculate the average SMUP size using an incremental stimulation technique.
- To elicit incremental responses, administer submaximal stimulation with a duration of 0.1 ms at 1 Hz frequency, gradually increasing the intensity in 0.03 mA increments until a minimal all-or-none response is achieved. Acquire the initial response with a stimulus intensity ranging between 2 mA and 10 mA.
- If the initial response does not occur with a stimulus intensity between 2 mA and 10 mA, modify the position of the stimulating cathode, either bringing it closer or moving it farther from the phrenic nerve in the neck, to decrease or increase the necessary stimulus intensity, respectively.
- If the first incremental response is achieved with a stimulus intensity ranging from 2 mA to 10 mA, save the first response and acquire additional increments with progressively higher stimulus intensities, adjusting in increments of 0.03 mA, to achieve a total of 9 additional increments that fulfill the following criteria in step 3.2.2.
NOTE: Each SMUP is quantified by subtracting each increment from the preceding increment.
- While measuring the incremental responses, make sure that each increment meets the following criteria:
- Make sure that the initial negative peak of the incremental responses aligns temporally with the negative peak of the maximal CMAP response.
NOTE: The slight movements observed due to background noise from respiratory cycles are inherent to the nature of the experiment. However, the consistent presence of SMUPs during live observation confirms their identity for that specific CMAP. - As the diaphragm is a dynamic muscle involved in respiration, each breathing cycle may induce baseline movement. Thus, verify the stability and absence of fractionation in each incremental response by confirming consistency across three duplicate responses.
NOTE: To distinguish low-amplitude evoked potentials, especially the first SMUP, from background noise due to respiratory activity, it is important to remain vigilant and observe for 3-4 respiratory cycles. Also ensure the alignment of peaks with those of the CMAP for accuracy. - Ensure that each increment is distinct and larger than the previous one. Therefore, visually distinguish incremental responses in real time, observing them as they overlay on the previously recorded increments.
NOTE: Multiple replicates of the stimulus at each amplitude might be conducted to ensure consistency in the increments and compliance with the predefined criteria. - After visually verifying each increment with the aforementioned criteria, confirm that the increment amplitude is at least 25 µV. If the increment is below 25 µV, discard the measurement and re-assess the response.
- Following the recording of 10 incremental responses, verify that the amplitude of each increment response is not greater than one-third of the combined amplitude of all 10 increments, representing the total amplitude of the final response. If this criterion is not satisfied, repeat the measurement of the 10 incremental responses.
NOTE: The threshold of one-third is based on the assumption that each incremental response represents the activation of a single motor unit. If the amplitude of any incremental response exceeds one-third of the combined amplitude of all ten increments, it suggests that the response may not be solely attributable to the activation of a single motor unit. Instead, it could be influenced by the recruitment of additional motor units or the presence of non-specific activity, such as electrical noise or artifacts22,26. - To estimate the average amplitude of the SMUPs, average the values of the 10 increments. Another method to measure average SMUP amplitude is to divide the entire amplitude of the final incremental response by the total number of increments11.
- Make sure that the initial negative peak of the incremental responses aligns temporally with the negative peak of the maximal CMAP response.
- Determine MUNE by dividing the maximum CMAP amplitude (peak-to-peak) by the average SMUP amplitude (peak-to-peak). In certain electrophysiological systems, SMUPs are recorded in microvolts (µV), while CMAP is usually expressed in millivolts (mV). If required, convert CMAP and SMUP measurements to the same units before calculating MUNE.
NOTE: Peak-to-peak CMAP, average SMUP, and MUNE are typically automatically calculated by clinic electromyography systems):

CMAP = Compound Muscle Action Potential
SMUP = Single Motor Unit Potential
MUNE = Motor Unit Number Estimation
- Calculate the average SMUP size using an incremental stimulation technique.
The CMAP, SMUP, and MUNE techniques outlined in this report enable the recording of neuromuscular function in the diaphragm muscle employing minimally invasive electrode placement (Figure 1). The parameters of amplitude and area can be employed to characterize the supramaximal CMAP size, providing an overall measure of muscle group output (Figure 2). However, in our current methods, we rely on amplitude to quantify both CMAP and SMUP sizes. CMAP, SMUP, and MUNE can be utilized to measure neuromuscular function in various rat models of neuromuscular disease. To demonstrate MU loss in the context of MN degeneration, rats underwent bilateral intrapleural injection with CTB-SAP (25 µg) to target phrenic MNs and extra CTB (25 µg), and control rats received unconjugated CTB (25 µg) and SAP (25 µg)1,27.
In Figure 3, findings in an adult control rat and an adult rat (12 weeks) seven days following intrapleural CTB-SAP injection are compared. Following intrapleural injection of CTB-SAP, MUNE is reduced at 60 estimated functional motor units compared with normal findings of 74 functional motor units in the control rat. However, the CMAP amplitude in the CTB-SAP rat (14.25 mV peak-to-peak) exhibited minimal changes compared to the control (14. 5 mV peak-to-peak) likely due to collateral sprouting. In Figure 4, diaphragm CMAP, SMUP, and MUNE were acquired bilaterally and averaged at baseline/preinjection (n = 14), as well as 7 (n = 14), 14 (n = 14), 21 (n = 6), and 28 (n = 14) days post injection. In Figure 4, no baseline differences between groups were found. MUNE showed a significant change for time (p < 0.05), CTB-SAP (p < 0.001), and interaction time x CTB-SAP (p < 0.01) with ~40% reduction of MUNE in CTB-SAP rats. The average SMUP of CTB-SAP rats demonstrated a significant change with time (p < 0.05) and CTB-SAP (p < 0.01), but no significant interaction with ~50-60% increase in SMUP amplitude. CMAP showed no significant change.
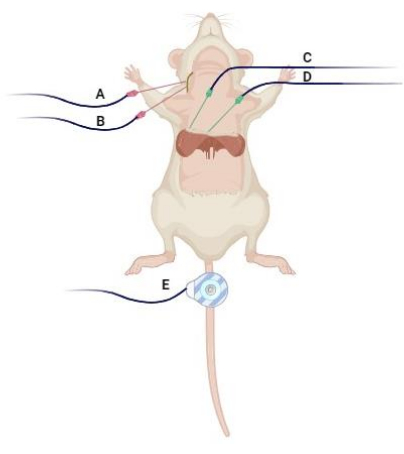
Figure 1: Electrode placement. The (A) stimulating cathode and (B) anode are subcutaneously inserted in the lateral neck between the anterior and middle scalene muscles approximately 1 cm apart. The (C) "active" electrode (E1) and (D) "reference" recording electrode (E2) are positioned over the midclavicular line inferior to the last rib border, following the angle between the xiphoid process and the last costosternal cartilage. Additionally, (E) a disposable disk electrode is situated on the tail as a ground to minimize artifacts. Created with BioRender.com. Please click here to view a larger version of this figure.
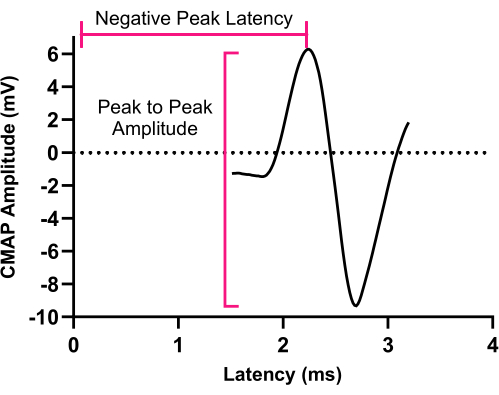
Figure 2: Compound muscle action potential. An illustration of a representative CMAP response recorded from the left hemidiaphragm muscle. CMAP peak to-peak amplitude is determined from negative peak voltage to positive peak voltage. Abbreviation: CMAP = Compound muscle action potential. Please click here to view a larger version of this figure.
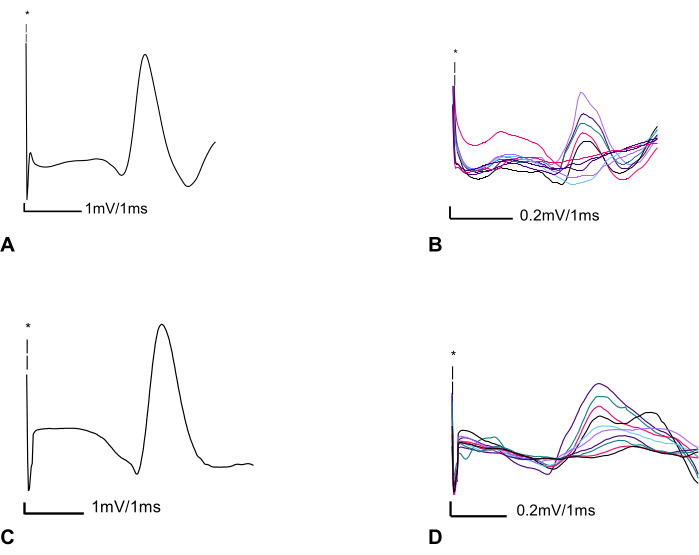
Figure 3: Two representative CMAP and MUNE recordings from a control rat, and an adult rat seven days after CTB-SAP intrapleural injection. (A) Left phrenic compound muscle action potential (CMAP) in a control adult rat (12 weeks of age) with peak-to-peak amplitude of 14.5 mV. Screen sensitivity = 1 mV/division and screen duration 1 ms/division. (B) Ten subsequent incremental responses with a total amplitude of 1.940 mV are divided by 10 to determine the average SMUP size (0.194 mV). Screen sensitivity = 0.2 mV/division and sweep speed of 1 ms/division. Calculated MUNE = 74 (MUNE=CMAP/average SMUP (14.5 mV/ 0.194 mV)) (C) Phrenic CMAP seven days following CTB-SAP injection showing almost no change in CMAP peak-to-peak amplitude 14.25 mV. Screen sensitivity = 1 mV/division and sweep speed of 1 ms/division. (D) Ten subsequent incremental responses with a total peak-to-peak amplitude of 2.360 mV divided by 10 to obtain an average SMUP size of 0.236 mV. Screen sensitivity = 0.2 mV/division and a sweep speed of 1 ms/division. Thus, the calculated MUNE was 60. Abbreviations: CMAP = compound muscle action potential; MUNE = motor unit number estimation; CTB-SAP = cholera toxin B fragment conjugated to saporin; SMUP = single motor unit potential. *Illustrates the artifact caused by electrical stimulation; it is important to note that due to the contrast between the amplitude of the electrical stimulus and CMAP, as well as incremental responses, we graphed only a portion of the stimulus. Blind-colored friendly colors have been utilized to enhance the visualization of the incremental responses for improved accessibility. Please click here to view a larger version of this figure.
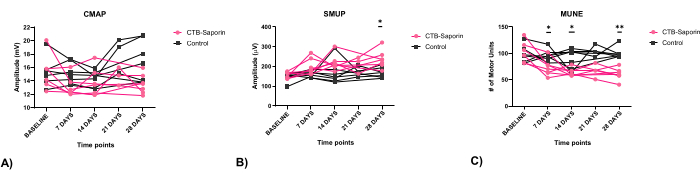
Figure 4: Electrophysiological assessment of CMAP, SMUP, and MUNE following CTB-SAP. No baseline differences between groups were found (seven 11-week-old male rats in both CTB-SAP and control groups). (A) CMAP showed no significant change. (B) The average SMUP of CTB-SAP rats showed a significant change over time (p < 0.05) and with CTB-SAP (p < 0.01), with no significant interaction, indicating a 50-60% increase in SMUP amplitude. (C) Seven days after CTB-SAP injection, the mean MUNE significantly decreased by 27.07%, from 102.58 ± 20.54 to 72.43 ± 15.59 estimated functional motor units (Mean ± SD). This reduction persisted, with an additional 11.75% decline at 28 days (MUNE: 60.64 ± 11.33, p < 0.01). All measurements at baseline, 7, 14, and 28 days after injection were obtained from 14 rats, with n = 7 rats injected with conjugated CTB-SAP and n = 7 rats receiving unconjugated CTB and SAP as the control group. Six rats were used on day 21. CMAP, SMUP, and MUNE data are presented as mean, and comparisons were performed using two-way ANOVA. Asterisks indicate differences at various time points: *p < 0.05, and **p < 0.01. Abbreviations: CMAP = compound muscle action potential; MUNE = motor unit number estimation; CTB-SAP = cholera toxin B fragment conjugated to saporin; SMUP = single motor unit potential. Please click here to view a larger version of this figure.
