The process of experimental mouse modeling is illustrated in Figure 1. After 12 h of injection completion, an open-field video recorder was used to monitor the movement distance and immobility duration of different experimental groups of mice for 5 cycles (Figure 2A). During the 5 cycles, mice in the PI V group maintained a low level of movement distance within 3 min, while the immobility ratio within 3 min increased with each subsequent cycle (Figure 2B,C). Additionally, statistical analysis was conducted on the total movement distance of mice from different experimental groups during the 5 cycles. The PI V group showed the smallest total movement distance compared to the other experimental groups, and the difference was statistically significant (p < 0.001) (Figure 2D,E). With the exception of the control group and PI I group, the mice in the other experimental groups exhibited negative growth in D-Value weight. Among them, the PI V group showed the greatest change in weight, and the difference in weight change compared to the other experimental groups was statistically significant (Figure 2F). After evaluating the survival rate of an additional 10 mice in each experimental group, the results showed that the mortality rate of mice in group PI V reached 80% on the 5th day. However, there was no statistically significant difference in mortality rate between the other four experimental groups and the control group mice (Figure 2G).
Using a high-power microscope, significant cellular swelling, necrosis, and inflammatory cell infiltration were observed in the PI IV and PI V groups of mice (Figure 3A,B). Using the rating criteria as provided in Supplementary Table 2, the pancreatic pathology of different experimental groups of mice was evaluated, and observed significant differences in the pancreatic pathology score compared to the control group mice (p < 0.001) (Figure 3C; Supplementary Figure 1). In addition, compared to the control group,the levels of serum amylase and lipase in the measured mice were significantly higher in the PI II to PI V experimental groups, and the differences were statistically significant. Interestingly, there was no statistically significant difference in the PI I group mice (Figure 3D,E). The ELISA method was employed to assess the levels of inflammatory markers14, including TNF-α and IL-6, in the serum of mice. The findings revealed that TNF-α and IL-6 levels in the PI V group mice were significantly higher than those in the other experimental groups, and the differences were statistically significant (Figure 3F,G). Compared with the control group, the PCT levels increased in all four experimental groups, but only the difference in the PI V group was statistically significant (p < 0.05) (Figure 3H).
The apoptotic status of pancreatic tissues in different experimental groups of mice
By performing TUNEL staining on the pancreatic tissues of each group of mice, the cellular necrosis status in the pancreatic tissues of different experimental groups was observed (Figure 4A). The grayscale values (OD) per unit area of pancreatic tissue sections and the positive rate of cellular necrosis were semi-quantitatively analyzed using Image J software. The results showed that compared to the other experimental groups, the level of cell necrosis in the pancreatic tissues of the PI V group of mice was significantly increased, and the difference was statistically significant (p < 0.001) (Figure 4B,C). Protein immunoblotting experiments were performed to assess the expression levels of cysteinyl aspartate specific proteinase-3 (Caspase-3), a cellular necrosis marker, in the pancreatic tissues of mice from different experimental groups (Figure 4D). Quantification of caspase-3 expression showed that the expression level of caspase-3 protein in the pancreatic tissues of the PI V group was significantly increased, and the difference was statistically significant (p < 0.001). The protein expression levels were quantified and normalized to the internal control GapDH (Figure 4E). Additionally, fresh pancreatic acinar cell suspensions were labeled with Annexin V-FITC/PI and analyzed by flow cytometry. It was found that compared to the other experimental groups of mice, the PI V group had a significantly higher positive rate of cell death, which was statistically significant (p < 0.001) (Figure 4F,G).
The content of HMGB-1 in peripheral serum and the expression level of HMGB-1 in pancreatic tissue
In order to investigate the relationship between HMGB-1 protein and pancreatic injury, immunohistochemical staining and quantification were performed on the pancreatic tissues of mice in each experimental group. There was a statistically significant difference between the experimental and control groups (p < 0.001) (Figure 5A,B). ELISA was used to measure the levels of HMGB-1 in the serum of mice from different experimental groups. The results showed that compared to the control group, the serum levels of HMGB-1 were significantly higher in all experimental groups, with the highest level observed in the PI V group, and the difference was statistically significant (p < 0.001) (Figure 5C). Furthermore, Western blot analysis detected elevated expression of HMGB-1 protein in the pancreatic tissues of mice in all experimental groups, with statistically significant differences compared to the control group (p < 0.001) (Figure 5D,E).
Figure 1: Experimental flowchart. Day 2 and Day 3: Intraperitoneal injection. Day 4: The open field experiment was initiated after 12 h of the last intraperitoneal injection. Day 5: Euthanized 36 h after the intraperitoneal injection. Please click here to view a larger version of this figure.
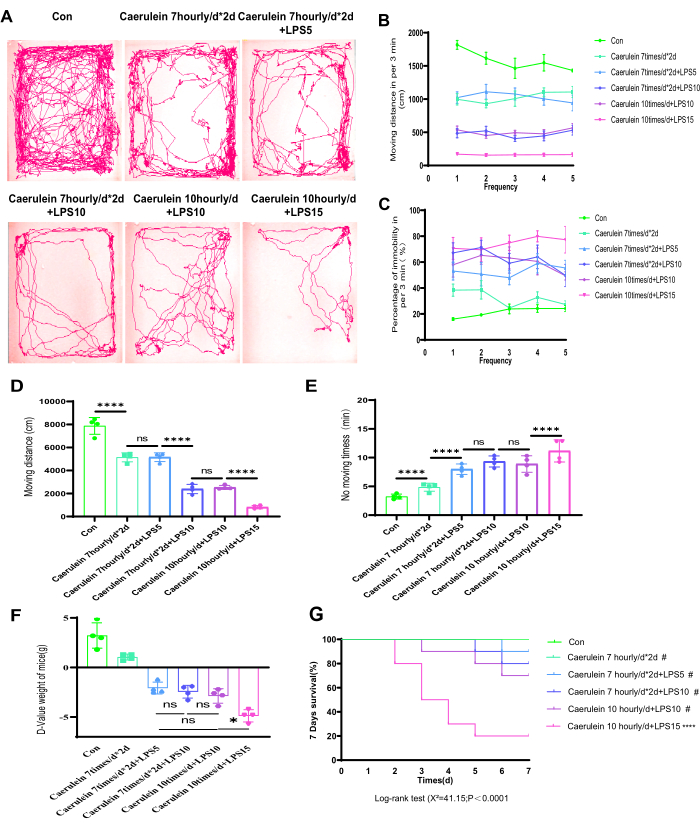
Figure 2: Macroscopic changes in the PI mice model. (A) The real-time movement trajectory plot of mice is depicted. (B) The total distance of movement within each monitoring period for different experimental groups of mice. (C) The percentage of immobility time within each monitoring period for different experimental groups of mice. (D,E) The total movement distance and immobility time percentage during 15 min were analyzed for mice in different experimental groups. (F) The D-value representing the weight of mice before and after the modeling process is shown. (G) The survival of 10 mice in each group was observed for the 7 days following the intraperitoneal injection. Data are expressed as means ± SEM, n = 4. "ns" denotes not significant, *P < 0.05, ****P < 0.001. Please click here to view a larger version of this figure.
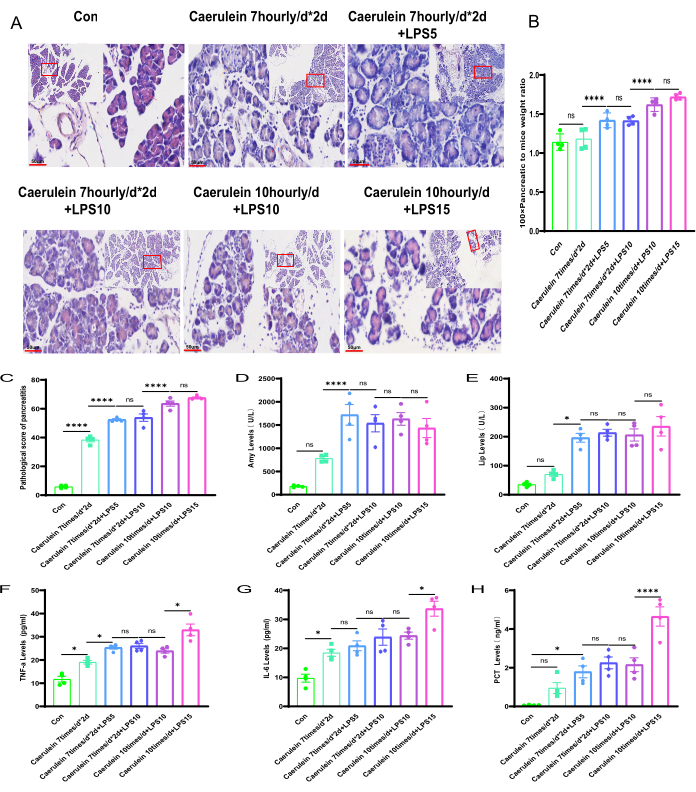
Figure 3: Pathological changes in mice pancreatitis among different experimental groups. (A) The H&E-stained histological sections of the mice pancreatic tissue in different experimental groups (paraffin-embedded pancreatic tissue sections stained with hematoxylin and eosin, magnifications of 100-fold and scale bars 200 µm, and 400-fold and scale bars 50 µm, respectively. Yellow long arrows indicate islets; red long arrows indicate acinar cells; brown long arrows indicate blood vessels; blue long arrows indicate ducts). (B) Calculation of the ratio of pancreatic weight to body weight in mice. (C) Pathological scoring of mice pancreas. (D,E) Detection of serum amylase and lipase levels in mice. (F–G) ELISA measurement of serum TNF-α and IL-6 levels in mice. (H) Assessment of PCT level.Data are expressed as means ± SEM, n = 4. "ns" denotes not significant, *P < 0.05, ****P < 0.001. Please click here to view a larger version of this figure.
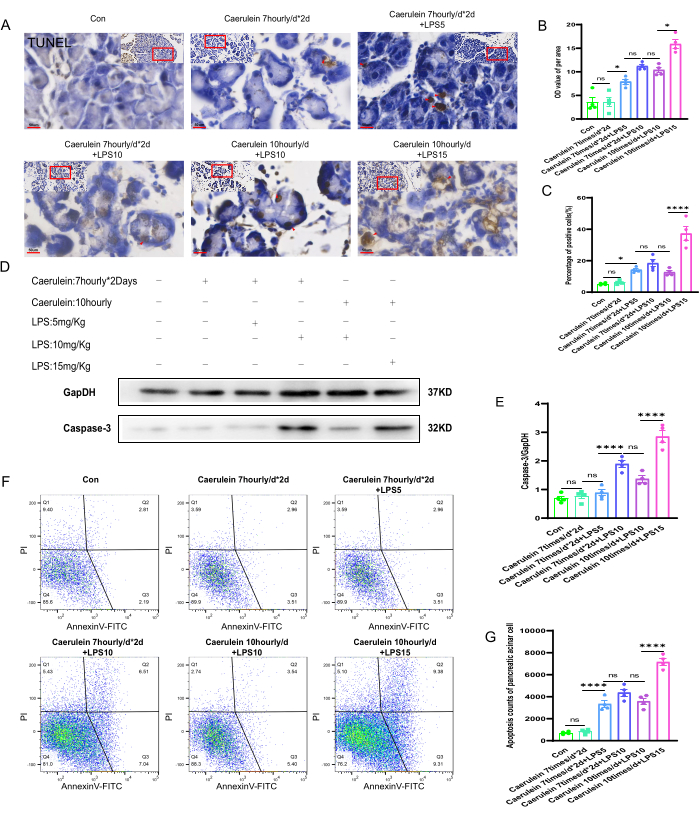
Figure 4: Apoptosis of pancreatic tissue in mice. (A) Representative images of TUNEL staining were obtained from pancreatic paraffin sections of mice and enlarged area images. (400x, scale bar 50 µm, brownish yellow is positive cells). (B,C) Quantitative analysis of the grayscale value per unit area of TUNEL-stained sections of mice pancreatic tissue and the percentage of positively stained dead cells. (D) The expression level of Caspase-3 in pancreatic tissue was detected by Western blot. (E) Quantification of Caspase-3 expression in pancreatic tissue. (F) Flow cytometry was employed to evaluate the extent of cell death in mice pancreatic acinar cells. (G) Enumeration of late-stage dead cells in mouse pancreatic acinar cells.Data are expressed as means ± SEM, n = 4. "ns" denotes not significant, *P < 0.05, ****P < 0.001. Please click here to view a larger version of this figure.
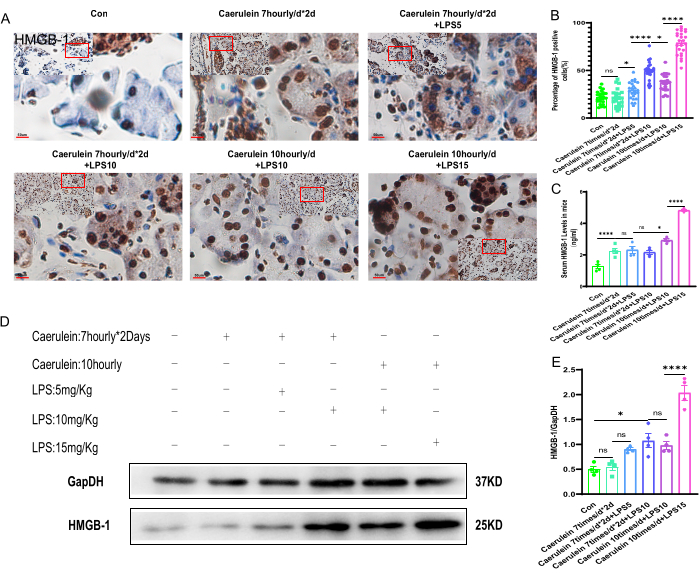
Figure 5: The HMGB-1 expression in mice pancreatic tissue. (A) Representative images and enlarged images (x400, scale bar 50 µm) of immunohistochemical staining of HMGB-1 on pancreatic sections. The brownish-yellow color indicates positive cells (n = 4). (B) The percentage of HMGB-1 positive cells in pancreatic tissue sections (n = 24). (C) The level of HMGB-1 in mouse serum (n = 4). (D,E) A Western blot was performed to detect the expression level of HMGB-1 in pancreatic tissue and to obtain the quantification results (n = 4).Data are expressed as means ± SEM, "ns" denotes not significant, *P < 0.05, ****P < 0.001. Please click here to view a larger version of this figure.
Supplementary Figure 1: Multiple organ injury in the PI V group mice model. (A) Representative images of histological changes in the pancreas, lung, liver, and kidney tissues collected from the CON and PI V group mice were analyzed using H&E staining (200x magnification, scale bar 50 µm). Pathological alterations associated with acinar cell necrosis are indicated by black arrows. Yellow arrows indicate pathological changes characterized by interstitial hemorrhage and edema in the alveoli. Hepatocyte edema and necrosis are denoted by green arrows. Glomerular hemorrhage-related pathological changes are marked by red arrows. (B) Calculation of histological scores was performed on pancreas, lung, liver, and kidney tissues obtained from the CON group and PI V group mice. Please click here to download this File.
Supplementary Table 1: Intraperitoneal injection protocol. Please click here to download this File.
Supplementary Table 2: Pathological scoring criteria for severity of pancreatitis. Please click here to download this File.
