The animal study was performed with the approval of the Institutional Animal Care and Use Committee (IACUC) at the University of the Pacific (Animal Protocols 19R10 and 22R10). Eight Male athymic nude mice aged 5-6 weeks, weighing 20-25 g, bred with the referenced Rodent Diet and housed under pathogen-free (SPF) conditions, were used for the present study. Cages, bedding, and drinking water were autoclaved and changed regularly. A schematic of tumor inoculation in mice is shown in Figure 1. See the Table of Materials for details related to all materials and instruments used in this protocol.
1. Establishment of three-dimensional MCS of A549-iRFP cells
- Incubate A549-iRFP cells (human lung adenocarcinoma) in a humidified atmosphere with 5% CO2 at 37 °C and grow them in complete growth medium DMEM containing 10% fetal bovine serum, 1% penicillin-streptomycin, and 1 µg/mL puromycin.
- Seed A549-iRFP cells into 96-well ultra-low attachment, round-bottom spheroid microplate at a seeding density of 4,000 cells/well, using 100 µL of complete growth medium supplemented with 0.3% collagen.
- Centrifuge the microplates at 300 × g for 7 min at 4 °C to facilitate the MCS formation. Examine the MCS morphology under a microscope to ensure cell aggregation after centrifugation.
- After 48 h, add 100 µL of complete growth medium to each well to achieve a total volume of 200 µL of growth medium per well.
- Replace 100 µL of growth medium in each well with fresh complete growth medium every other day.
2. Characterization of A549-iRFP MCS
- Observe and image the MCS morphology using a microscope and estimate the MCS volume by simulation with the referenced software from MATLAB based on the phase-contrast microscope images.
- Open one MCS image in ImageJ software.
- Use Freehand selections to select the edge of the MCS and add it to ROI Manager.
- Click Edit | Selection | Create Mask.
- Click Edit | Invert.
- Click File | Save As | Tiff.
- Open ReViSP software.
- Open the saved TIFF image by clicking Browse.
- Click Start to complete the MCS simulation.
- Measure the iRFP fluorescent signal using the infrared imaging system at the 700 nm channel and quantify the fluorescent signal using software (e.g., Image Studio).
- Open Image Studio software.
- In the Channels tab, select 700 and Intensity = 5.
- In the Scan Controls tab, select 84 µm, Medium, 0.0 mm, and Flip Image. Keep everything else as default.
- Click Start to start scanning.
- Assess and quantify cell viability using the 3D cell viability assay according to the vendor protocol.
- Assess and quantify cellular protein using the BCA Assay according to the vendor protocol.
3. MCS selection for tumor inoculation
NOTE: After MCS are seeded into spheroid microplates and grown for 2-3 weeks with regular growth medium exchange, select MCS with the following appropriate characteristics for tumor inoculation.
- Observe the MCS morphology under a microscope and choose MCS with a round shape with overall smooth edges but with 5-10 rough buddings (arrows in Figure 2F) and a diameter within the range of 700-800 µm.
- Measure the iRFP fluorescence (refer to step 2.2) and select the MCS whose fluorescent signals are within one standard deviation of the average.
4. Intrapulmonary MCS inoculation
NOTE: Use 70% isopropyl alcohol spray to clean the surgical station and the tools before handling the animals.
- Anesthetize each mouse with an IP injection of 80 mg/kg ketamine and 12 mg/kg xylazine; pinch the mouse feet with forceps to ensure full anesthesia.
- Inject 10 µL of buprenorphine hydrochloride (0.3 mg/mL) subcutaneously to reduce the pain.
- Apply ophthalmic ointment on the eyes to prevent dryness.
- Place the mouse in a dorsal posture and secure the limbs in a stretching position with tapes.
- Sterilize the back skin with iodine and alcohol swab sticks.
- Cut a 0.5-1 cm incision using surgical scissors on the left back side (Figure 1B). Carefully use forceps to separate the muscle and fat tissues until the chest wall and lung motion are visible.
- Transfer one selected MCS from a microplate into a glass Petri dish containing ice-cold PBS, using a pipette.
- Attach a 20 G needle onto a 100 µL glass syringe, precool them on ice, and draw 20 µL of a precooled mixture of PBS and Matrigel (1:1 v/v).
- Use the syringe to quickly aspirate one MCS from the Petri dish in a minimum volume of PBS-Matrigel mixture, keeping the MCS in the metal part of the needle.
NOTE: Keep a tight grip on the syringe and plunger to prevent the MCS from slipping out of the needle. - Gently insert the needle vertically between two rib bones to ~3 mm depth and slowly inject all the 20 µL PBS and Matrigel mixture that contains the MCS.
NOTE: Avoid excessive force during the insertion to prevent damage to the lung, vasculature, or heart. - Carefully remove the needle and apply triple antibiotic ointment to the wound.
- Seal the incision with surgical clips, which are to be removed after 2 weeks.
NOTE: Do not suture the incision because the suture lines may interfere with fluorescence imaging. The nude mice are able to heal naturally after surgery. - Place the animal on an infrared heat pad and cover it with laboratory wipes to maintain the body temperature. Monitor the animal for at least 30-60 min until it wakes up and moves properly.
- Inject 10 µL of buprenorphine hydrochloride (0.3 mg/mL) subcutaneously 3x a day for the first 48 h to reduce the pain.
5. Postsurgical monitoring
- Measure the body weight every 3-4 days.
- Measure the iRFP fluorescent signal from the tumor xenograft every 3-4 days on a small animal imaging system at 700 nm channel in four postures: left, right, dorsal, and ventral, while the mice are kept under anesthesia by isoflurane inhalation (flow rate: 1.5-2 L/min oxygen containing 1.5% isoflurane) over 2-3 min.
- Quantify the net fluorescent intensity of the xenograft cancer in vivo using software (e.g., Image Studio).
- Use a fixed rectangle (A1, 200 x 125 pixels) as the sampling window for the chest area of the mice.
- Use the free-hand function to trace the shape of the mice within the rectangle (A1) and measure the fluorescent intensity (F1) in area A1.
- Use another smaller rectangle (A2, 25 x 40 pixels) to measure the background fluorescence (F2) of the mice in the thigh area.
- Use equation (1) to calculate the net fluorescent intensity of the xenograft cancer in each mouse:
 (1)
(1)
Characterization of A549-iRFP MCS
A549-iRFP MCS were successfully cultured in spheroid microplates with the assistance of collagen and centrifugation. When MCS reached a diameter of approximately 500 µm after 1 week, both A549 and A549-iRFP MCS were exposed to a variety of anticancer drugs and formulations for 3 days and then maintained in drug-free growth medium for 4 additional days. The A549-iRFP MCS exhibited a response pattern closely mirroring that of the parent A549 cells. A549 and A549-iRFP MCS showed similar dose-response curves and IC50 values to cisplatin, one of the first-line anticancer drugs against lung cancer (Figure 2A). The viability of A549 and A549-iRFP MCS was inhibited to similar degrees by other anticancer drugs or formulations (Figure 2B).
The A549-iRFP MCS were monitored over a period of up to 6 weeks by iRFP fluorescence, cell viability, and cellular protein levels. The volume of MCS was estimated by software simulation based on the phase-contrast microscope images, and the simulated morphology exhibited similar shapes to those imaged by microscope and fluorescent signal (Figure 2C). The cell viability of A549-iRFP MCS was quantified by 3D cell viability assay, and the assay was validated with MCS of various sizes from 350 to 950 µm in diameter. There were no significant differences observed across various volume ratios between the growth medium containing MCS and the assay reagent, and between different shaking times of 5 minutes and 10 minutes. (Supplementary Figure S1). All four biomarkers increased with time, with larger variations at later time points (Figure 2D). The iRFP fluorescence exhibited strong correlations with the other three more traditional quantitative measurements of MCS: volume (Pearson r = 0.9307, p < 0.0001), cell viability (Pearson r = 0.7666, p < 0.0001), and cellular protein (Pearson r = 0.7317, p < 0.0001) (Figure 2E).
Tumor progression in mice
After growing for 2-3 weeks, A549-iRFP MCS with appropriate characteristics, including morphology, MCS diameter, appropriately rough edges, and fluorescent signal (for detailed parameters, see protocol section 3), were selected for tumor inoculation. After the tumor inoculation surgery, the body weight of tumor-bearing mice was measured every 3 days and presented as the change ratio compared to the weight on Day 0 right before surgery. The mouse body weight decreased slightly after surgery and recovered quickly within 1 week. Without treatment, the body weight increased gradually until ~Day 40 but decreased drastically (~15%) in the following week, leading to the euthanasia (three-fold anesthetic overdose: 80 mg/kg ketamine and 12 mg/kg xylazine via IP injection) of mice according to IACUC guidelines (Figure 3A). Tumor-bearing mice were imaged every 3 days in four postures: left, dorsal, right, and ventral sides. Among these, the left (where the tumor is inoculated) and ventral (where both sides of the lungs can be observed) were selected as key postures for the quantification of net fluorescent intensity according to equation (1) (Figure 3B,C). The net fluorescence intensity from both postures showed a similar trend of tumor progression, with fluorescence from the ventral side growing slightly slower than the left side.
The MCS xenograft in this orthotopic model progressed through distinct phases mirroring the four clinical stages of NSCLC (Figure 3D)18,19,20. Around Day 8 post-MCS inoculation, concentrated fluorescence emerged in the left lung, signifying the establishment of a localized tumor in line with Stage 1 NSCLC in clinical settings. By approximately Day 11, the fluorescence notably intensified and/or dispersed across multiple sites in the left lung, indicating the presence of tumor(s) resembling Stage 2 NSCLC. Subsequently, at approximately Day 18, increased fluorescent signals were observed from the ventral side, suggestive of Stage 3-like progression of the xenograft. Moreover, anatomical examination and ex vivo imaging revealed tumor growth on the surface of the heart, a significant hallmark of Stage 3 NSCLC. By approximately Day 27 post-MCS inoculation, perfused fluorescence appeared on both sides of the lung, and open-chest anatomy disclosed perfused tumor growth in the heart, trachea, and major blood vessels, indicative of cancer metastasis akin to Stage 4 NSCLC.
Response of tumor-bearing mice to cisplatin
A pilot efficacy study was conducted on this orthotopic lung cancer murine model. Ten days after tumor inoculation, 5 mg/kg cisplatin or normal saline was injected via the tail vein of tumor-bearing mice, one injection per week, totaling two injections. The ventral-side images on tumor-bearing mice are presented in Figure 4A. The body weight and tumor fluorescence were monitored every 3-4 days. Compared with the normal saline group, the mice in the cisplatin group lost significant body weight after each cisplatin injection but recovered in the weeks after the cisplatin treatment (Figure 4B). The net fluorescence intensity in the cisplatin group showed a slower trend of increase than that in the saline group (Figure 4C). At the end of the in vivo fluorescence monitoring, the animals were sacrificed and their lungs dissected and imaged by fluorescence. After normalization by the total tissue protein, the fluorescent intensity of the lungs dissected from mice in the cisplatin group was confirmed to be lower than that of the normal saline group. (Figure 4E). In the ventral fluorescent imaging (Figure 4A), the images in the red rectangles indicate the first time when the tumor fluorescence was visualized in both the left and the right lungs, which is a key indicator of tumor metastasis at Stage IV NSCLC. Cisplatin, one of the first-line lung cancer drugs, slowed down the tumor metastasis from the left lung to the right lung (Figure 4D).
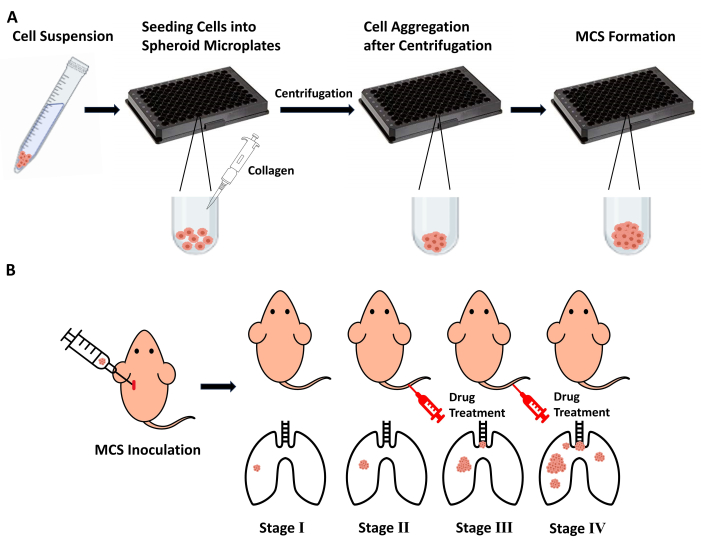
Figure 1: Flow chart of the study. (A) Seeding A549-iRFP cells into spheroid microplates to form MCS with the assistance of collagen and centrifugation. (B) Intrapulmonary inoculation of A549-iRFP MCS with appropriate characteristics into a mouse's left lung to construct the orthotopic lung cancer xenograft model, mimicking the four stages of lung cancer in clinical settings. The white syringe containing one MCS indicates tumor inoculation while the two red syringes indicate drug treatment administered through the tail vein. Abbreviation: MCS = multicellular spheroid. Please click here to view a larger version of this figure.
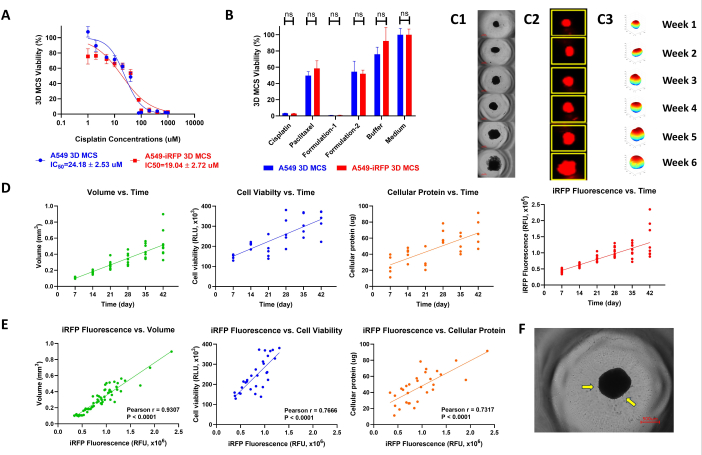
Figure 2: Characterization of A549-iRFP MCS. (A) Dose-response curves of A549-iRPF MCS and A549 MCS to cisplatin after 3-day exposure and 4-day drug-free growth (Mean ± SD, N = 3-4). (B) Cell viability of A549-iRFP MCS after 3-day exposure to anticancer treatments (cisplatin, paclitaxel, or two drug formulations developed in-house) and 4-day drug-free growth (Mean ± SD, N = 3-4). (C) Morphological studies of representative A549-iRFP MCS after 1-6 weeks of culturing by contrast phase microscopy (C1, scale bar = 500 µm), fluorescent confocal microscopy (C2), and software simulation (C3). (D) Dynamic change of the iRFP fluorescence, volume, cell viability, and cellular protein of A549-iRFP MCS over 1-6 weeks (N = 10 for iRFP fluorescence and volume; N = 5 for cell viability and cellular protein). (E) Correlation of iRFP fluorescence of A549-iRFP MCS with the other three traditional growth measurements (volume, cell viability, and cellular protein) over 1-6 weeks (N = 60). (F) An example of A549-iRFP MCS of appropriate characteristics for tumor inoculation (scale bar = 500 µm). Abbreviation: MCS = multicellular spheroid. Please click here to view a larger version of this figure.
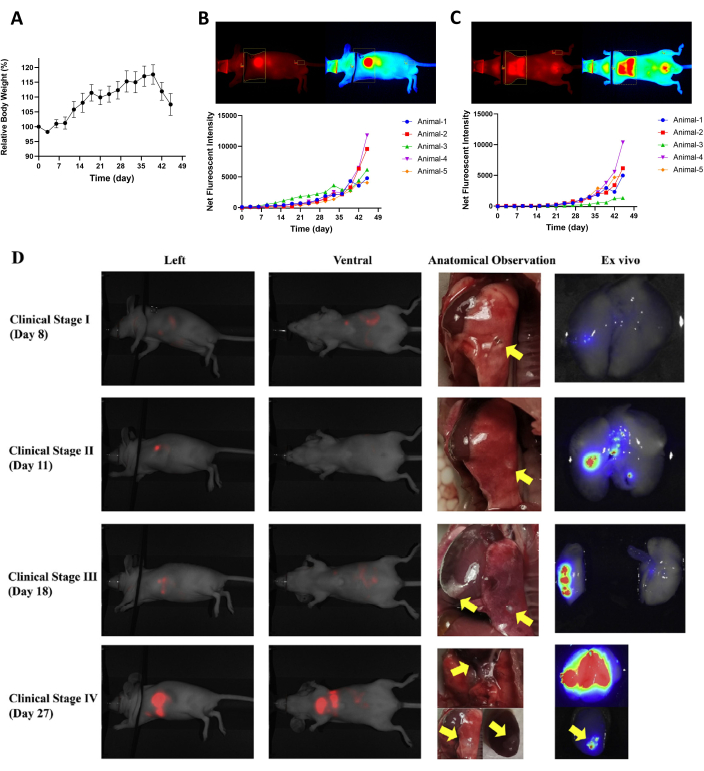
Figure 3: Tumor progression in the orthotopic murine model of NSCLC. (A) Change in body weight of mice after tumor inoculation (Mean ± SEM, N = 5). (B) Dynamic change of net fluorescent intensity in tumor-bearing mice based on left-side imaging (N = 5). (C) Dynamic change of net fluorescent intensity in tumor-bearing mice based on ventral-side imaging (N = 5). (D) Cancer progression mimicking the four clinical stages of NSCLC. Left-side imaging, ventral-side imaging, anatomical observation (yellow arrows indicate tumors in the lung and on the heart surface), and ex-vivo imaging of representative tumor-bearing mice at four stages. This figure is taken from Huang et al.18. Abbreviation: NSCLC = non-small cell lung cancer. Please click here to view a larger version of this figure.
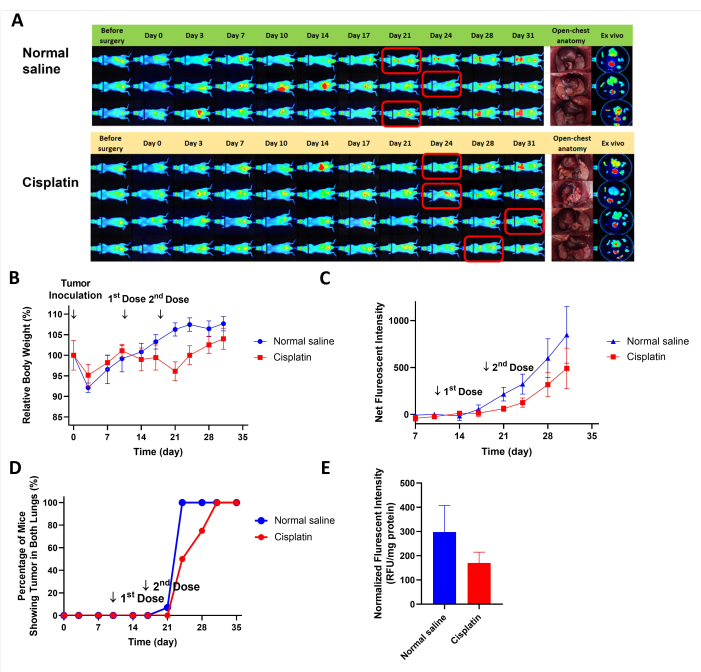
Figure 4: Tumor-bearing mice's response to cisplatin. (A) Ventral-side imaging of tumor-bearing mice after treatment with saline or cisplatin (images in red rectangles indicate when the tumor fluorescence can be first visualized in both the left and the right lungs). (B) Change in the body weight of tumor-bearing mice after saline or cisplatin treatments (Mean ± SEM, N = 3-4). (C) Dynamic change of net fluorescent intensity in tumor-bearing mice after saline or cisplatin treatments based on ventral-side imaging (Mean ± SEM, N = 3-4). (D) Percentage of mice showing tumor fluorescence on both the left and the right lungs. (E) Normalized fluorescent intensity of lungs dissected from mice sacrificed at the end of in vivo fluorescent imaging (Mean ± SEM, N = 3-4). Please click here to view a larger version of this figure.
Supplementary Figure S1: 3D cell viability assay on A549-iRFP MCS of various diameters. (A) ~350 µm; (B) ~550 µm; (C) ~750 µm; (D) ~950 µm. Please click here to download this File.
