
Figure 1: Preparation of the catheter. (A and B) The guide cannula and the dummy cannula (catheter cap with inlet) are assembled and screwed. (C) Then the catheter is cut to 2 mm in size with the help of a scalpel. The microscopic observation showed that the usage of scissors for that purpose distorts the circular shape of the cannula tip, and, thereby, must be avoided.
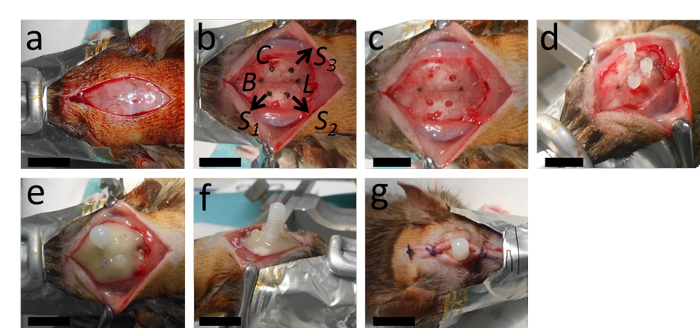
Figure 2: The implantation of the catheter. (A) The surgery starts with a longitudinal incision and removal of the periosteum. (B, C) This panel shows the marking of the place for the catheter at 2 mm posterior from Bregma and 2.4 mm lateral to the right from the sagittal suture; as well as the places for the holes intended for the three anchor screws with an appropriate distance from the catheter and Lambda. (D) After drilling the catheter hole (a 0.5 mm diameter, with a round drill tip) and the holes for the anchor screws (1.3 mm-diameter with a twisted drill tip), the anchor screws are tightened. (E, F) Then the catheter is inserted and the whole setup is stabilized with polymerizing dental cement. (G) The wound is stitched with two or three knots anterior and posterior to the catheter. B = Bregma; L = Lambda; C = Catheter; S1, S2 and S3 = places for the holes for the three anchor screws. The scale bars = 1 cm.

Figure 3: Preparation of rMOG/IFA emulsion. (A) The mixture of rMOG, PBS, and IFA is emulsified by pressing the inoculum from one syringe to another by pushing the pistons back and forth, (B) until it is white and viscous. (C) Subsequently, the inoculum is distributed to 1 mL syringes for the injection. 5 µg of rMOG is used in 200 µL of PBS/IFA mixture to sub clinically immunize one rat; however, due to the losses at the tips and walls of the syringes during the preparation, a larger volume should be prepared.
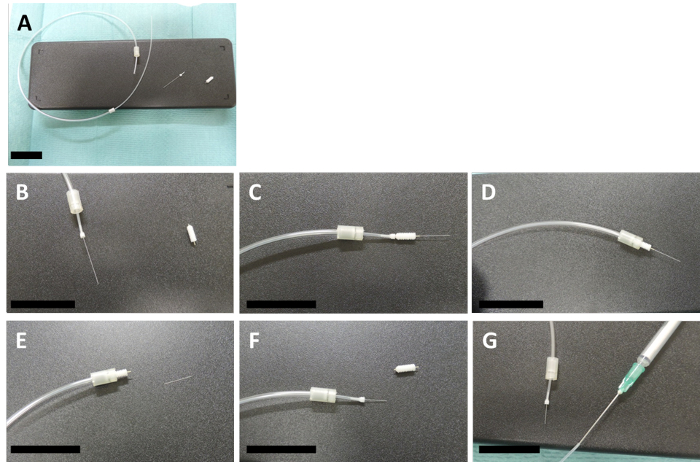
Figure 4: Preparation of the connector cannula. (A -cD) These panels show how a connector and an internal are assembled with a 2-mm size template guide cannula. (E) The internal is cut to the same size as the guide cannula with the help of a scalpel (F) and the template guide is then unscrewed. (G) The other end of the connector cannula is fixed to a 1 mL syringe, which contains the injection mix, with a 20 G needle. The scale bars = 3 cm.
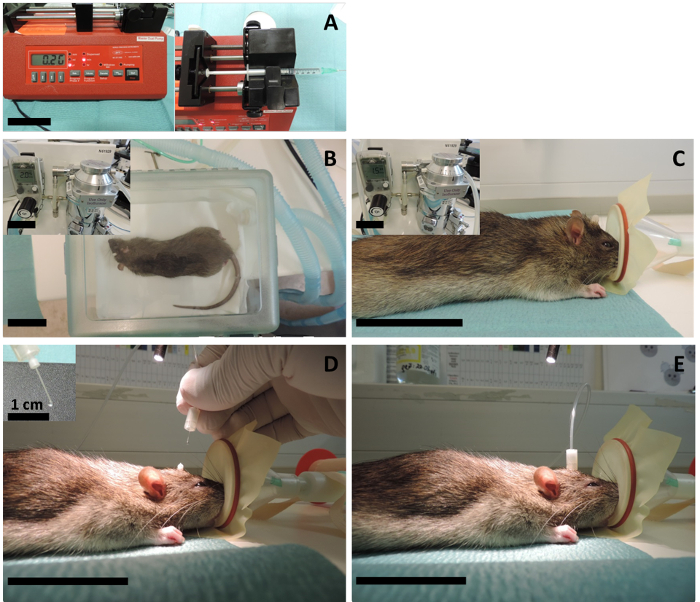
Figure 5: Intracerebral injection. (A) A programmable syringe pump is adjusted for a 2 µL/min injection speed, and the 1 mL syringe filled with cytokine mix (or sterile PBS for the controls) is mounted to the pump. (B) The animal is first anesthetized in the chamber using 5% isoflurane with a 2 L/min oxygen flow and then (C) the anesthesia is sustained through the mask using 2.5% isoflurane with a 1.5 L/min oxygen flow. (D) The catheter cap with the inlet (the dummy cannula) is screwed off and the injection cannula is inserted through the implanted catheter. Since the volume of the injection is very small, the investigator should be cautious to avoid air bubbles at the tip of the cannula. For that reason, it is important to start the insertion while the pump is in operation and only when there is a growing liquid bubble at the tip. The extra volume will not go into the brain anyway, as it breaks down on top of the catheter before the insertion. (E) Then the connector cannula is tightened, and the pump is let to operate for 10 min. After 10 min of injection, the pump is stopped, and the cannula is left inside for 15 – 20 min to allow for the diffusion of the injected volume to the interstitial fluid. The scale bars = 5 cm unless indicated otherwise.
