A Decellularization Methodology for the Production of a Natural Acellular Intestinal Matrix
Summary
The article describes a methodology for the production of an acellular matrix from rat intestine. The derivation of intestinal scaffolds is important for future applications in tissue engineering, stem cell biology and drug testing.
Abstract
Successful tissue engineering involves the combination of scaffolds with appropriate cells in vitro or in vivo. Scaffolds may be synthetic, naturally-derived or derived from tissues/organs. The latter are obtained using a technique called decellularization. Decellularization may involve a combination of physical, chemical, and enzymatic methods. The goal of this technique is to remove all cellular traces whilst maintaining the macro- and micro-architecture of the original tissue.
Intestinal tissue engineering has thus far used relatively simple scaffolds that do not replicate the complex architecture of the native organ. The focus of this paper is to describe an efficient decellularization technique for rat small intestine. The isolation of the small intestine so as to ensure the maintenance of a vascular connection is described. The combination of chemical and enzymatic solutions to remove the cells whilst preserving the villus-crypt axis in the luminal aspect of the scaffold is also set out. Finally, assessment of produced scaffolds for appropriate characteristics is discussed.
Introduction
Tissue engineering (TE) provides a therapeutic alternative to organ transplantation, bypassing issues of immunosuppression and organ shortage. TE has recently had successful applications in the clinic, with replacement of organs such as the bladder1, urethra2 and trachea, both in adults3,4 and children5.
Building a tissue-engineered organ necessitates the combination of a scaffold with the appropriate cells. A scaffold can be prepared using naturally-derived (e.g. collagen) and synthetic (e.g. poly-L-glycolic acid; PLGA) materials, or be obtained by the decellularization of native organs and tissues. Scaffolds that have been used thus far for intestinal TE have mainly been either decellularized (small intestinal submucosa) or synthetic (poly-L-glycolic acid and poly-lactic acid)6-13. These biomaterials are very simple in both macro- and micro-architecture, which may not be ideal if tissue-engineered intestine is to be clinically translated. An optimal biomaterial for the intestine should have an innate vascular tree that can be connected to the host's blood supply, a tiered tubular wall with different properties to reflect the layers of the intestinal wall and a villus-crypt axis on the luminal side to aid with repopulation by epithelial stem cells.
Decellularization is a novel methodology that produces scaffolds by removing cells from whole organs whilst maintaining their original architecture14. This is preferable to already existing scaffolds since they do not only replicate the structure of the organ but also contain chemical cues embedded within the extracellular matrix (ECM) that aid cellular proliferation and differentiation. In 2008 a cadaveric trachea was decellularized14, seeded with the patient's own cells, and transplanted to replace the main left bronchus in a young man3. Since then, a number of groups have reported the production of decellularized scaffolds for the heart15, liver16,17, and lung18-20 in small and large animals.
We have also adapted the same methodology to produce a small intestinal decellularized scaffold21. The goal of the method described herein is to produce decellularized intestinal matrices that maintain the macroscopic characteristics of the original tissue such as the blood supply, as well as the microscopic architecture of the villus-crypt axis in the intestinal lumen. We believe this methodology could ultimately be adopted for other organs to improve the efficiency of decellularization.
Protocol
1. Isolation of Rat Intestine
- Prepare a 1 L solution of Phosphate Buffered Saline (Sigma, UK) with 1% antibiotic/antimycotic (Sigma, UK) (PBS/AA). Fit the peristaltic pump (Masterflex L/S variable speed) with two tubes. Run 70% ethanol (EtOH) through the tubes of the peristaltic pump for 15 min at maximum speed, followed by PBS/AA for another 15 min.
- Euthanize adult Sprague-Dawley rats weighing approximately 250-350 g by CO2 inhalation and cervical dislocation in accordance with local animal guidelines and approvals (in the UK, Home Office guidelines under the Animals (Scientific Procedures) Act 1986).
- Autoclave the surgical instruments before use. Spray and wipe the abdomen of the animal using 70% EtOH.
- Perform a xifo-pubic laparotomic incision on the abdomen to ensure a clear surgical field.
- Eviscerate the small intestine on the right side of the animal onto a paper towel sprayed with 70% EtOH. Take care to continuously wet the intestine with PBS/AA so as to avoid dehydration of the tissue and denaturation of the extracellular matrix (ECM).
- Locate the superior mesenteric artery (SMA) arising in a 90° angle from the aorta towards the intestine. Use a 27 G cannula to enter the SMA from the aorta and quickly withdraw the needle to avoid tearing the wall of the vessel. Advance the plastic tube of the cannula into the SMA and secure using sutures (Vicryl 5/0).
- Confirm cannulation by injecting 1 ml of PBS/AA. Use spring scissors to incise the aorta proximal and distal to the SMA so as to release the cannula.
- To avoid leakage of feces when dissecting out the large intestine, place one (Silk 5/0) suture knot on the proximal end of the ileocaecal junction and one at the distal end of the sigmoid colon. Then cut the terminal ileum and colon between the two knots and remove the large intestine.
- Cut the intestine at the jejuno-duodenal junction and free the intestine from any connective tissue connections it might have with the abdomen.
- Transfer the small intestine in a Petri dish with PBS/AA. Cannulate the proximal section of the intestine with a plastic Pasteur pipette (LSL Laboratory Consumables) and secure it in place with sutures. Cut the pipette so it will fit the Luer-Lok of a 60 ml syringe (BD Plastipak). Flush the intestinal lumen 2x with 60 ml of PBS/AA to remove feces and debris.
2. Decellularization Methodology
- Connect the vascular cannula to a three-way stopcock. This will ease handling, minimize tension on the vascular tree and allow removal of bubbles from the tubing.
- Start running deionized water (resistivity 18.2 MΩ/cm) through the Masterflex L/S variable speed roller pump at 0.6 ml/hr. Ensure no bubbles are present within tubing prior to connecting with the intestinal lumen stopcock. Some bubbles may be present within the lumen from step 1.9, which may impair the decellularization process. Vary the speed of the pump and handle the tissue with forceps carefully to ensure the bubbles exit from the distal end. Do not connect the vascular cannula until this process is finished since high speeds may damage the vascular tree.
- Transfer apparatus to the cold room, since the following step of decellularization is performed at 4 °C. The low temperature allows removal of cells whilst minimizing tissue decomposition. Place the Petri dish in a container that will collect the overflowing solution. Perfuse both the intestinal lumen and the vascular tree with deionized water (resistivity 18.2 MΩ/cm) for 24 hr at 0.6 ml/hr. For the first hour check the apparatus regularly to ensure all connections are secure, leakage is minimal and no bubbles are present within the intestine.
- After 24 hr of treatment with deionized water, move decellularization apparatus outside the cold room as the rest of the steps are carried out in room temperature (RT).
- Weigh sodium deoxycholate (Sigma, UK) to prepare 300 ml of a 4% solution in deionized water. Weigh sodium deoxycholate under a suction hood, as it is an oral and eye irritant. Mix using a vortex until the solution is clear. The solution may be maintained at 4 °C for up to 1 month.
- Change the deionized solution to sodium deoxycholate, check the connections, remove any bubbles and perfuse at 0.6 ml/hr for 4 hr.
- Following the sodium deoxycholate step wash with PBS/AA for 30 min to avoid interaction between the sodium deoxycholate and DNase-I.
- Weigh out deoxyribonuclease-I (DNase-I, Sigma) and prepare 250 ml of a 2,000 kU solution in 1 M sodium chloride, pH 7.4. Mix using a vortex until the solution is clear. This solution must be prepared immediately before use and can't be stored.
- Perfuse with DNase-I for 3 hr at RT at a speed of 0.6 ml/hr.
- Following the DNase-I step, transfer the scaffold into a tissue culture hood and change plates and instruments. It is suggested to use aseptic technique.
- Wash with PBS/AA for 30 min to ensure all remnants of the decellularization solutions are removed. Place the scaffold in a new Petri dish and transfer to a UV Crosslinker (Spectroline, US). Run two sterilization cycles. Store in 5% PBS/AA and change the solution every 3 days.
Representative Results
Upon successful decellularization (Figure 1), the scaffold should have a macroscopic appearance similar to the one of the native intestine, but with translucent walls (Figure 2A). The preservation of macro-architecture should also be evident by the patency of the vascular tree. When dye is injected through the SMA cannula, it should distribute evenly throughout the scaffold and reach the capillary tree (Figure 2B). The scaffold should be free of nuclear and cytoplasmic material, something that can be assessed using a DNA quantification kit and simple histological analysis. Hematoxylin and eosin staining (H&E) should demonstrate an absence of nuclear and cytoplasmic material whilst preserving the small intestinal layers (Figure 3A). In particular, the maintenance of the villi and crypts on the luminal side should be evident following scanning electron microscopy (Figure 4). A conservation of extracellular matrix components such as collagen, elastin and glycosaminoglycans should also be expected. For example, Masson's Trichrome staining displays intact connective tissue in the scaffold (Figure 3B).

Figure 1. Experimental plan. Timeline of decellularization procedure; PBS/AA: phosphate buffered saline with antibiotic-antimycotic, NaDeoxy: Sodium deoxycholate, RT: room temperature, DNAse-I: deoxyribonuclease-I. Click here to view larger image.
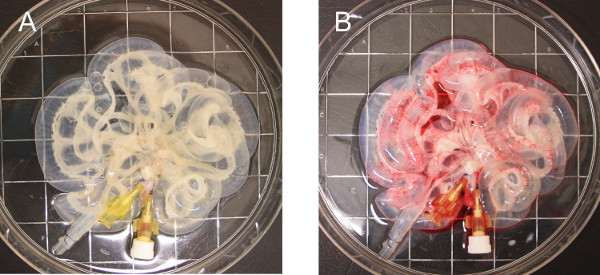
Figure 2. Scaffold macroscopic characteristics. Macroscopic appearance of the rat small intestine following successful decellularization (A). Injection of Rosso Ponceau dye through the SMA demonstrates an intact vascular network (B) ; SMA: superior mesenteric artery Click here to view larger image.
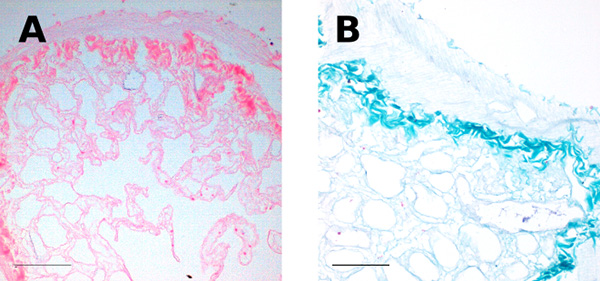
Figure 3. Histology. H&E (A) and MT (B) staining indicate an absence of cellular material with preservation of the connective tissue architecture; H&E: hematoxylin and eosin, MT: Masson's trichrome. Scale bar: 100 μm. Click here to view larger image.
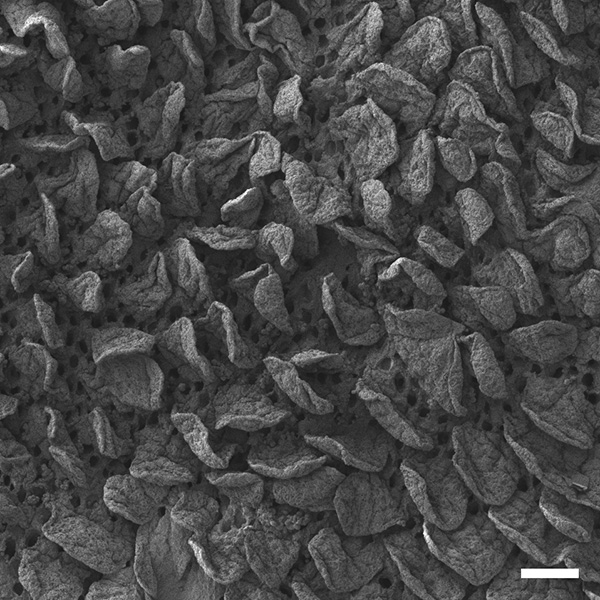
Figure 4. Electron Microscopy. Scanning electron microscopy indicates the preserved villus-crypt architecture in the scaffold lumen; Scale bar: 100 μm. Click here to view larger image.
Discussion
The most difficult steps in setting up this experiment involve the cannulation of the SMA and the establishment and maintenance of sterility. Cannulating the SMA in rodents without rupturing the wall can be quite difficult due to the size and position of the vessel. Alternatively, a suture may be placed around the proximal aorta prior to the SMA origin, followed by cannulation of the aorta itself distally, directing the plastic cannula into the SMA. During decellularization a combination of poor cannula placement and high flow rates may result in losing the vascular access. Sterility is a major issue due to the amount of bacterial flora present in the small intestine. Washing with PBS/AA following harvest is very important, and any sign of fecal matter or debris must be removed from the lumen. Placing a portion of the scaffold in a falcon tube with DMEM in the incubator following UV sterilization should be an indicator if sterility has been achieved. In the case of bacterial colonization, the media will change the pH with its color turning from red to yellow. To deal with this, further UV cycles are advised as well as washing with PBS containing a high concentration of antibiotic/antimycotic.
A possible modification to obtain a scaffold with both vascular and venous access would be to cannulate the inferior vena cava (IVC) as well as the SMA. Decellularization from the venous and vascular sides should be attempted intermittently for all three solutions. Continuous decellularization may burst the capillaries by having positive pressure on both sides.
Over the years there have been a number of efforts in intestinal TE using different cell-scaffold combinations in vitro and in vivo6,9,12. The majority of the work has been performed using tubular nonwoven 95% PGA-5% PLGA scaffolds coated with collagen type I6,7,13,22. Following seeding with intestinal epithelial organoid units (OUs) and a period of implantation into the omentum of mice, they form cysts with muscle on the outside and epithelium on the inside which can then be tubularized. However, the porosity and simplicity in the design of these scaffolds does not permit for the generation of large pieces of artificial intestine in an in vitro environment such as that of a bioreactor. Additionally, the lack of an innate vascular network that can be connected to the recipient further limits the use of this scaffold for clinical translation. Besides the experiments with the PGA-PLGA scaffolds, other groups have used collagen or SIS scaffolds, both of which do not replicate the intricacy of the intestinal tract. SIS in particular is the only previous published methodology of intestinal tissue engineering and has been used in more than 150 medical settings, demonstrating the ability of decellularized scaffolds to provide mechanical stability and promote cell growth whilst leading to no immunogenic response. However, the lack of appropriate macro- and micro-architecture, has led to poor results in its' use for intestinal TE purposes9-11,23.
The benefits of the decellularization methodology we have described include the preservation of microscopic characteristics such as the luminal crypt-villus architecture that represent an appropriate environment for the repopulation by the intestinal stem cell niche. In the macroscopic aspect, the presence of a hierarchical vascular network will enable attachment to the recipient, allowing provision of nutrients and oxygen to all layer of the TE-intestine21. What is more, the maintenance of ECM components such as collagen, elastin and glyocosaminoglycans has an important role not only for mechanical characteristics but also directing cellular proliferation and differentiation. Most importantly, the ability of the decellularization methodology to be scaled up into larger tissues whilst maintaining the same characteristics is an important feature for clinical translation of TE.
The development of a natural intestinal matrix with a vascular network allows the creation of larger segments of artificial intestine that can be connected to the host.
Disclosures
The authors have nothing to disclose.
Acknowledgements
The authors thank the Wake Forest Institute of Regenerative Medicine for their help with development of this protocol. We acknowledge support by grants from the Great Ormond Street Hospital charity, the Foundation Eugenio Litta (Geneva, Switzerland), the Medical Research Council, the Royal College of Surgeons of England, the Sparks Children’s Medical Charity, the British Foreign Office for the UK/USA Stem Cell Collaboration Award and the Mittal Research Fund. We would also like to thank the Royal Society/ Wolfson Foundation for the tissue engineering laboratory refurbishment grant obtained for the Pediatric Surgery Department in the Institute of Child Health. PDC and SE are supported by the Great Ormond Street Hospital Children’s Charity.
Materials
| Name of Material | Company | Catalog Number | Comments |
| Ethanol solution, 70% in H20 | Sigma | 02877 | |
| Phosphate buffered saline tablets | Sigma | 79382 | |
| Antibiotic Antimycotic Solution (100x) | Sigma | A5955 | |
| Sodium deoxycholate | Sigma | D6750 | Oral and eye irritant; use protection |
| Sodium chloride | |||
| Deoxyribonuclease I from bovine pancreas | Sigma | D5025 |
References
- Atala, A., Bauer, S. B., Soker, S., Yoo, J. J., Retik, A. B. Tissue-engineered autologous bladders for patients needing cystoplasty. Lancet. 367 (9518), 1241-1246 (2006).
- Raya-Rivera, A., Esquiliano, D. R., Yoo, J. J., Lopez-Bayghen, E., Soker, S., Atala, A. Tissue-engineered autologous urethras for patients who need reconstruction: an observational study. Lancet. 377 (9772), 1175-1182 (2011).
- Macchiarini, P., Jungebluth, P., et al. Clinical transplantation of a tissue-engineered airway. Lancet. 372 (9655), 2023-2030 (2008).
- Macchiarini, P., Walles, T., Biancosino, C., Mertsching, H. First human transplantation of a bioengineered airway tissue. J. Thorac. Cardiov. Surg. 128 (4), 638-641 (2004).
- Elliott, M. J., de Coppi, P., et al. Stem-cell-based, tissue engineered tracheal replacement in a child: a 2-year follow-up study. Lancet. 380 (9846), 994-1000 (2012).
- Grikscheit, T. C., Siddique, A., et al. Tissue-engineered small intestine improves recovery after massive small bowel resection. Ann. Surg. 240 (5), 748-754 (2004).
- Sala, F. G., Matthews, J. A., Speer, A. L., Torashima, Y., Barthel, E. R., Grikscheit, T. C. A Multicellular Approach Forms a Significant Amount of Tissue-Engineered Small Intestine in the Mouse. Tissue Eng. Part A. , (2011).
- Matthews, J. A., Sala, F. G., Speer, A. L., Warburton, D., Grikscheit, T. C. VEGF optimizes the formation of tissue-engineered small intestine. Regen. Med. 6 (5), 559-567 (2011).
- Chen, M. K., Badylak, S. F. Small bowel tissue engineering using small intestinal submucosa as a scaffold. J. Surg. Res. 99 (2), 352-358 (2001).
- Wang, Z. Q., Watanabe, Y., Toki, A. Experimental assessment of small intestinal submucosa as a small bowel graft in a rat model. J. Pediatr. Surg. 38 (11), 1596-1601 (2003).
- Wang, Z. Q., Watanabe, Y., Noda, T., Yoshida, A., Oyama, T., Toki, A. Morphologic evaluation of regenerated small bowel by small intestinal submucosa. J. Pediatr. Surg. 40 (12), 1898-1902 (2005).
- Hori, Y., Nakamura, T., et al. Experimental study on tissue engineering of the small intestine by mesenchymal stem cell seeding. J. Surg. Res. 102 (2), 156-160 (2002).
- Gardner-Thorpe, J., Grikscheit, T. C., et al. Angiogenesis in tissue-engineered small intestine. Tissue Eng. 9 (6), 1255-1261 (2003).
- Conconi, M. T., Coppi, P. D., et al. Tracheal matrices, obtained by a detergent-enzymatic method, support in vitro the adhesion of chondrocytes and tracheal epithelial cells. Transpl. Int. 18 (6), 727-734 (2005).
- Ott, H. C., Matthiesen, T. S., et al. Perfusion-decellularized matrix: using nature’s platform to engineer a bioartificial heart. Nat. Med. 14 (2), 213-221 (2008).
- Uygun, B. E., Soto-Gutierrez, A., et al. Organ reengineering through development of a transplantable recellularized liver graft using decellularized liver matrix. Nat. Med. , 1-8 (2010).
- Uygun, B. E., Price, G., et al. Decellularization and recellularization of whole livers. J. Vis. Exp. (48), e2394 (2011).
- Petersen, T. H., Calle, E. A., et al. Tissue-Engineered Lungs for in Vivo Implantation. Science. 329 (5991), 538-541 (2010).
- Ott, H. C., Clippinger, B., et al. Regeneration and orthotopic transplantation of a bioartificial lung. Nat. Med. 16 (8), 927-933 (2010).
- Calle, E. A., Petersen, T. H., Niklason, L. E. Procedure for lung engineering. J. Vis. Exp. (49), e2651 (2011).
- Totonelli, G., Maghsoudlou, P., et al. A rat decellularized small bowel scaffold that preserves villus-crypt architecture for intestinal regeneration. Biomaterials. 33 (12), 3401-3410 (2012).
- Sala, F. G., Kunisaki, S. M., Ochoa, E. R., Vacanti, J., Grikscheit, T. C. Tissue-engineered small intestine and stomach form from autologous tissue in a preclinical large animal model. J. Surg. Res. 156 (2), 205-212 (2009).
- Demirbilek, S., Kanmaz, T., Ozardali, I., Edali, M. N., Yücesan, S. Using porcine small intestinal submucosa in intestinal regeneration. Pediatr. Surg. Int. 19 (8), 588-592 (2003).
