On normal spine ultrasound imaging, the dura is an echogenic layer that surrounds the anechoic spinal fluid. The spinal cord is distinguished by its homogenous appearance and low echogenicity which is surrounded by an echogenic rim. This echogenic rim is due to the density shift from the spinal fluid to the spinal cord. The central canal appears as a bright central echo, while exiting nerve roots appear highly echogenic, particularly at the cauda equina16. Intraoperative ultrasound can play an advantageous role in the intradural mass lesion resection. In a standard case, preoperative CT or MRI approximates the location of an intradural mass with respect to known adjacent structures. With this approximation, a durotomy is made, usually with the extension of the durotomy in either direction for sufficient exposure of the lesion. In cases of cauda equina tumors, the lesion can rostrally migrate with respect to preoperative imaging20. With intraoperative ultrasound, the lesion can be readily visualized prior to dural opening and durotomy can be made more appropriately and accurately to the exact location of the mass20,21. Furthermore, with intramedullary lesions where there is a need for dissection through the spinal cord to reach tumors, risk of neural damage and subsequent neurological deficit can be reduced with the use of intraoperative ultrasound to guide the surgeon22. Additionally, a sterile compressed sponge is easily identified on ultrasound a hyperechoic material without acoustic wave attenuation and can be utilized as a surgical marker to distinguish tissue planes and limits for dissection15,23. An example is seen in Figure 1, 2 and 3 where a cervical intramedullary lesion was approached via a midline myelotomy. Intraoperative ultrasound was beneficial in visualizing and delineating tumor limits, as well as determining resection and resolution of tumor mass effect.
Intraoperative ultrasound is also particularly useful in operative cases with a posterior approach to resect lesions ventral to the thecal sac, especially in the cervical and thoracic spine where the spinal cord is vulnerable to injury with manipulation. While the ventral spinal canal can be approached anteriorly for better visualization of the lesion, there are associated increases in operative time, bleeding, and morbidity. Thus, a posterior approach is preferable, and inability to visualize the lesion directly can be overcome with intraoperative ultrasound to guide the surgeon. Cases where this technique is particularly useful include resection of intervertebral disc herniations, reduction of thoracolumbar burst fractures, resection of ventral extradural tumors, and in cases of spinal canal stenosis due to ossification of the posterior longitudinal ligament where confirmation of adequate posterior decompression is needed13, 14, 24,25,26,27,28,29,30,31,32,33,34. In a symptomatic thoracic disc herniation resection by posterior approach, intraoperative ultrasound aided in evaluating decompression and ensuring all compressive disc fragments were excised (Figure 4-5). Similarly, in the case of a lumbar burst fracture, intraoperative ultrasound was useful in confirming adequate decompression and removal of all fragments (Figure 6-7).
| Imaging technology | Advantage |
| Intraoperative ultrasound | • Real-time |
| • Excellent soft tissue resolution | |
| Cone beam CT and intraoperative CT | • 3D and multiplanar reconstructions |
| • Able to be paired with navigation systems | |
| Intraoperative MRI | • Multiplanar reconsutrctions |
| • Excellent soft tissue resolution | |
| Intraoperative fluoroscopy | • Real-time |
| • 2D images of bony structures |
Table 1. Comparison of intraoperative imaging techniques
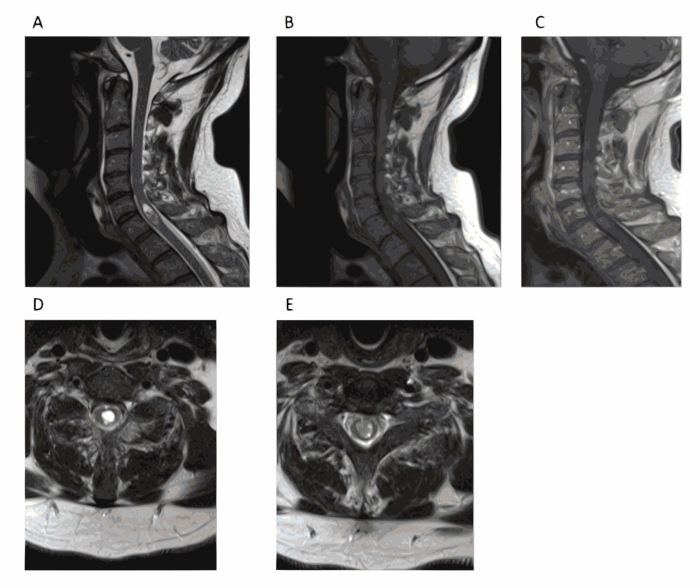
Figure 1. Preoperative images reveal an intramedullary lesion. A 54-year-old male with no significant past medical history presented with a 1-month history of fever. A cervical MRI revealed a C6 intramedullary lesion. The mass size did not change after 1 month and extensive workup did not reveal other possible causes of his fever. Patient was subsequently brought to the operating room for definitive diagnosis. (A) Sagittal T2-weighted MRI revealed an intramedullary lesion at C5-7 with fluid collection at the top of the mass. (B) Sagittal T1-weighted MRI. (C) Sagittal contrast-enhanced MRI shows scant rim enhancement. (D) Axial T2-weighted MRI at the level of the fluid collection. (E) Axial T2-weighted MRI of the lower part of the lesion. *This figure has been modified from Vasudeva et al.35. Please click here to view a larger version of this figure.
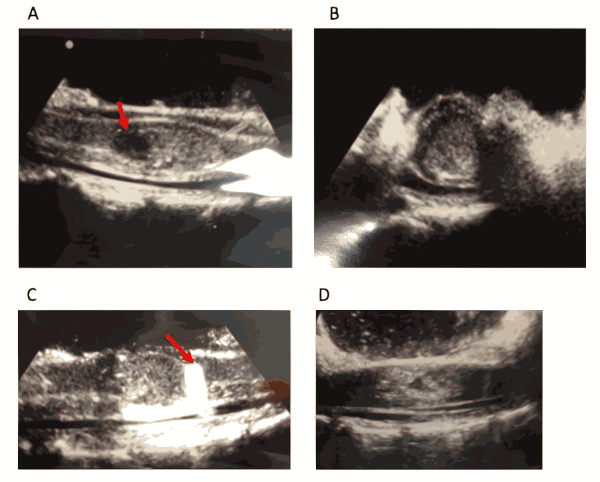
Figure 2. Intraoperative ultrasound of the spinal cord after laminectomy. Patient underwent a C5-7 laminectomy and subsequent resection of the intramedullary lesion. Intraoperative ultrasound was used to guide the surgical path through the spinal cord until the tumor could be visualized. (A) Intraoperative ultrasound correlated with preoperative MRI imaging, revealing fluid collection (white arrow). (B) Axial intraoperative ultrasound shows mass encompassing majority of the spinal cord. (C) A 0.5 cm x 0.5 cm piece of sterile compressed sponge (white arrow) was used during the operation to confirm the caudal limit of the tumor. (D) Intraoperative ultrasound post-resection confirming complete removal of tumor and resolution of mass effect. *This figure has been modified from Vasudeva et al.35. Please click here to view a larger version of this figure.
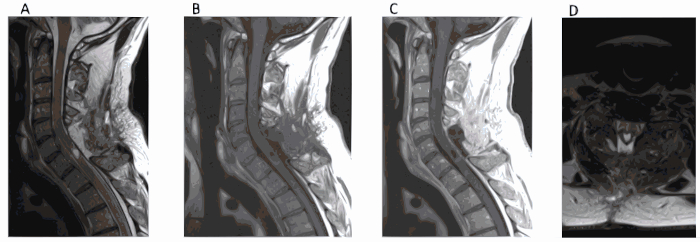
Figure 3. Post-operative resection imaging reveals complete tumor resection. Post-operatively, the patient returned to baseline and fever resolved. Pathology revealed grade II ependymoma. (A) Sagittal T2-weighted MRI 2 months post-operatively showing complete resection of the tumor. (B) T1-weighted MRI without contrast. (C, D) T1-weighted MRI with contrast. *This figure has been modified from Vasudeva et al.35. Please click here to view a larger version of this figure.
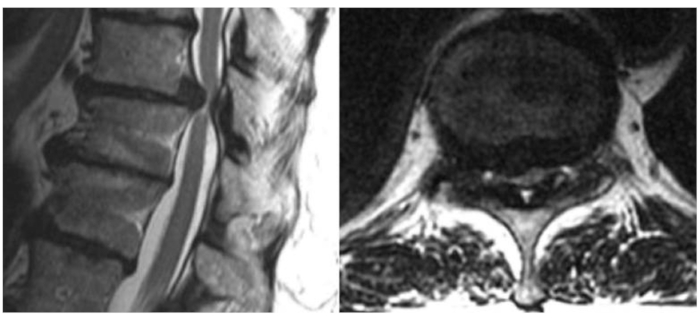
Figure 4. Preoperative MRI reveals severe spinal cord compression. A 73-year-old female presented with a history of several months of worsening gait dysfunction, spasticity, and numbness in her lower extremities. Motor strength was intact on neurological exam however she had marked clonus, 4+ lower extremity reflexes, and a wide-based staggering gait. CT and MRI revealed a large, noncalcified T10-11 intervertebral disc hernation with compression of the spinal cord. (A) Sagittal and (B) axial T2-weighted MRI revealing T10-11 disc herniation with spinal cord compression. *This figure has been modified from Vasudeva et al.35. Please click here to view a larger version of this figure.
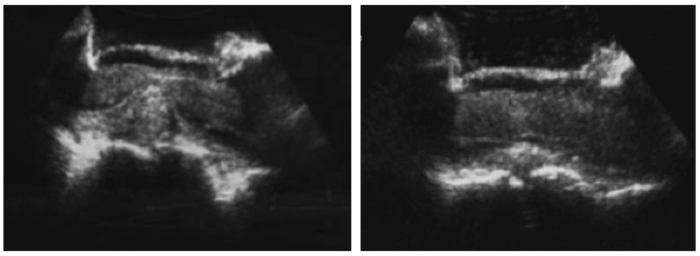
Figure 5. Intraoperative ultrasound reveals disc herniation and spinal cord compression. Patient underwent a right-sided T10-11 hemilaminectomy, facetectomy, and pedicle-sparing microdiscectomy with T9-11 fusion. (A) Intraoperative ultrasound was used to accurately determine the location of the disc herniation, (B) and to evaluate decompression and ensure complete removal of the herniated disc. Patient returned to her neurological baseline postoperatively and her prior symptoms had resolved at her 1-month follow up. *This figure has been modified from Vasudeva et al.35. Please click here to view a larger version of this figure.
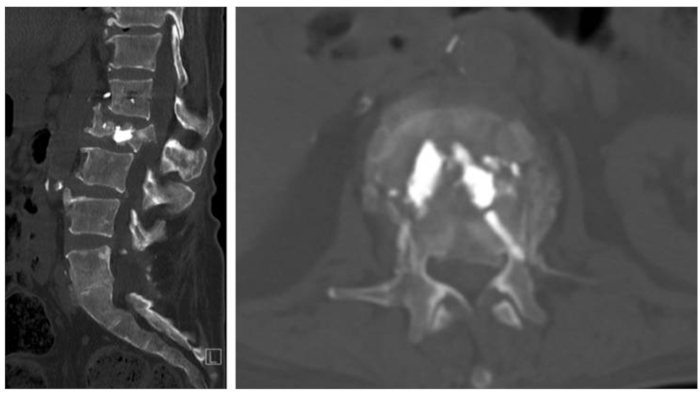
Figure 6. Preoperative CT demonstration pathological L2 burst fracture. A 57-year-old female with a history significant for metastatic appendiceal cancer and a balloon kyphoplasty at L1 and L2 a month prior for pathologic compression fractures presented with mechanical back pain and acute-onset of left anterior thigh pain. Motor strength was intact throughout, however she had decreased sensation to light touch over her left anterior thigh. (A) Sagittal and (B) axial CT revealed pathological L2 burst fracture. *This figure has been modified from Vasudeva et al.35. Please click here to view a larger version of this figure.
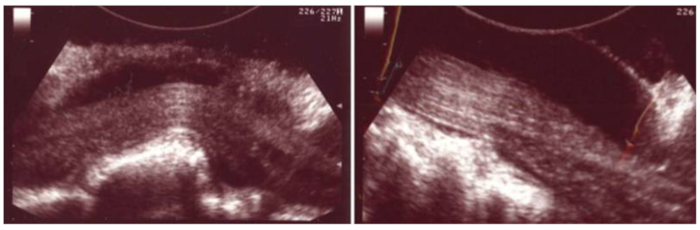
Figure 7. Intraoperative ultrasound reveals retropulsed bone fragment and subsequent complete reduction of fracture. Patient underwent an L1-L2 laminectomy, left transpedicular reduction of the fracture, and T12-L3 posterolateral fusion. Intraoperative ultrasound was used to identify any residual bone fragments. (A) A retropulsed bone fragment that was not directly visualized was seen in the ventral spinal canal displacing the thecal sac. (B) Complete reduction of the fracture and adequate decompression of the spinal canal was confirmed with ultrasound. Postoperatively, the patient returned to baseline with symptom resolution. *This figure has been modified from Vasudeva et al.35. Please click here to view a larger version of this figure.

{kind=link}