Summary
The goal of this protocol is to measure the center of pressure (COP) replacement using a high spatial resolution sensor sheet to reflect the spatial stability in a precision grip. The use of this protocol could contribute to greater understanding of the physiology and pathophysiology of grasping.
Abstract
The purpose of the protocol is to indirectly evaluate the direction of the finger force during manipulation of a handheld object based on the biomechanical relationships in which deviated force direction causes center of pressure (COP) replacement. To evaluate this, a thin, flexible, and high spatial resolution pressure sensor sheet is used. The system allows measurement of the COP trajectory in addition to the force amplitude and its temporal regulation. A series of experiments found that increased trajectory length reflected a sensorimotor deficit in stroke patients, and that decreased COP trajectory reflects a compensatory strategy to avoid an object slipping from the hand grip in the elderly. Moreover, the COP trajectory could also be decreased by dual task interference. This article describes the experimental procedure and discusses how finger COP contributes to an understanding of the physiology and pathophysiology of grasping.
Introduction
Force control is the fundamental basis of precision grip. Compared with power grip, precision grip evaluates the minimal force output reflecting the ability to manipulate an object. Multiple sensorimotor systems contribute to precision grip. For example, during a grip and lift task, visual information enables the perception of the object’s size and shape. After the fingertips touch the object, tactile signals are delivered to the somatosensory cortex to adjust the precision grip force. Grip force (GF) is generated when the fingertips make contact with the object, and it increases during the lifting phase1. When an object approaches the goal height in the air, healthy young adults produce the minimal GF to optimize cutaneous input from the finger pulps and conserve energy. On the other hand, older adults use a large grip force to avoid letting the object slip from their grip2. In stroke patients, onset of grip force is delayed and the ability to adjust the safety margin is impaired due to sensory and motor deficits. Exaggerated grip force is considered to be a strategic response to compensate for sensory and motor deficits3.
The standard protocol to measure GF control in precision grip was suggested by Johansson and Westling in the 1980s4. They developed a device to monitor both load and grip forces simultaneously. Since then, GF amplitude and its temporal regulation have been used as typical kinetic parameters in numerous studies on precision grip. Another kinetic parameter is the force direction5. The force direction results from a combination of grip and lift forces. In order to maintain stable precision grip, properly directed grip and lift forces must be generated between the thumb and index finger, and the deviated force direction can cause spatial instability. Although various load cell-type force direction instruments are used in grasping studies, these instruments have a limitation in terms of monitoring the grip force control in manipulating objects of different sizes and shapes used in daily living. Thus, a flexible and attachable sensor is essential to investigate the relationships between grip force control and daily functions.
The purpose of this protocol is to indirectly evaluate the finger force direction during manipulation of an object based on the biomechanical relationship in which deviated force direction causes Center of Pressure (COP) replacement. The COP is the center of all the forces, and represents how the forces are balanced on the sensor sheet. The use of COP to evaluate grip force control was first suggested by Augurelle et al.6. They monitored COP displacement to investigate the role of cutaneous feedback and found that deviated COP occurred after digital anesthesia. However, COP displacement was monitored only vertically in their study; therefore, the COP displacement in a three-dimensional space has not been adequately evaluated. To solve this limitation a thin, flexible, and high spatial resolution pressure sensor sheet was used to measure COP. Relatively high spatial resolution sensors (~60–100 points per cm2) to measure grip force control have been used7,8, but recent advances in spatial resolution (248 points per cm2) allow measurement of the COP trajectory as a parameter to quantify spatial stability. This paper describes the experimental procedure and discusses how finger COP contributes to the understanding of the physiology and pathophysiology of grasping.
Protocol
The series of studies in the present paper were approved by Gunma University Ethical Review Board for Medical Research Involving Human Subjects.
NOTE: Inclusion criteria for participants were the ability to understand the use of minimal force and the ability to perform the task with the thumb and index finger. Exclusion criteria were selected based on the purpose of the experiments.
1. Equipment preparation
- Connect two sensor connector cables to the USB ports of a computer. Pull up the lever attached to the sensor connector and insert the sensor’s tab into the insertion slot. Return the attached lever to its original position.
- Open the sensor software on a computer. Make sure that real-time pressure distribution maps appear automatically on the monitor when the sensor sheets are correctly connected.
- Pressure adjustment
- Insert the sensing area of the sensor sheet one by one into a compressor rig.
- Turn on the air valve of the compressor’s controller and start to apply pressure. Operate the regulator and adjust to the appropriate load value (i.e., 172 kPa) to check the indicator on the controller. Make sure that the whole area of the sensor sheet is equally pressurized on the monitor.
- While applying pressure to the sensor sheets, perform equilibration and calibration.
NOTE: Equilibration is an operation to adjust the reactivity of the sensor cells equally. Calibration is an operation to convert the pressure on the sensor sheet (raw sum) into a unit of weight (grams or Newtons) and display it. Both must be done for the sensor sheet before starting data collection for each participant.- Select Tools | Equilibration on the software main window. Click Equilibrate-1 | Start in the equilibration dialog box. Check the equilibration result in the dialog box and confirm the window of equilibration changes color to gray.
- Save the equilibration settings by clicking Save Eq. File in the equilibration dialog box. Enter the equilibration file name and click Save in the Save As dialog box.
- Next, perform calibration by selecting Tools | Calibration. Click the Add and enter the load value (134.33 N) in the Applied Force box.
- Click the Start button in the dialog box. Check the calibration result in the calibration dialog box and confirm that the calibration was done correctly; the value of Newton is shown as 134.33 and the value of loaded Cells matches with that of the sensor sheets being used if the calibration was done correctly.
- After that, save the calibration setting by clicking Save Cal. File. Enter the calibration file name and click Save in the Save As dialog box. After the equilibration and calibration, turn off the air valve on the controller and extract the sensor sheet from the compressor.
2. Measurement
- Preparation
- Connect each device and start up the software according to steps 1.1. and 1.2. Make sure that two real-time pressure distribution maps for each sensor sheet are displayed when the sensor sheets are connected via the cable at the same time.
NOTE: In this experiment, two sensor sheets are needed to measure the thumb and index finger, respectively. It is necessary to perform equilibration and calibration for each of them according to the procedures described in section 1.4. - Recall the equilibration and calibration files created in steps 1.4.2. and 1.4.5. With the real-time pressure distribution map active, select Tools | Load Equilibration File. Select the equilibration file and click Open. Then, select Tools | Load Calibration File. Select the calibration file and click Open. Make sure that the real-time pressure distribution map is displayed in Newtons after loading calibration file. Perform the above for each of the two maps.
- Attach the pressure-sensitive parts of the two sensor sheets to both sides of the iron cube using double-sided tape. To prevent the sensor sheets from being damaged, cut 3−5 mm lengths of tape and place them on the four corners on the outside of the iron cube. Make sure that the surface of the sensor sheet is on the outside.
- Place the iron cube on top of a setting stand on a table before the measurement.
- After arranging the measurement environment, fix the recording settings for the movie frames, period, and frequency. Select the Options | Acquisition Parameter command. In the data acquisition parameter dialog box, enter 36000 in the movie frames, 0.01 in the Period, and 100 in the frequency. Click OK and close the dialog box.
- Connect each device and start up the software according to steps 1.1. and 1.2. Make sure that two real-time pressure distribution maps for each sensor sheet are displayed when the sensor sheets are connected via the cable at the same time.
- Starting the measurement
NOTE: Figure 1 demonstrates a grip and lift task.- Have the participant sit in front of a table and adjust the table height (participant’s shoulder joint flexion 0° and elbow joint flexion 90° position). Set the iron cube and setting stand 30 cm from the participant in the midsagittal plane on the table. Wipe the participant’s finger pulps with an alcohol swab or towelette.
- Give the participant verbal instructions as follows: “Use minimal force with your thumb and index finger to grasp both sides of the iron cube to which the sensor sheets are attached. After that, lift it approximately 5 cm above the setting stand, hold it for 5−7 s, and then place it back on the setting stand.”
- If the participant is ready, give them a cue to start the task and start a recording by clicking Record on the toolbar. Click Center Of Force Trajectory to monitor the COP while recording. When the task is over, click Stop on the toolbar. After the recording, save the movie data by selecting File | Save Movie as. Enter the movie file name and click Save in the dialog box.
NOTE: The weight of the iron cube, number of lifts, and the interval between tasks should be considered according to the purpose of the experiment and task difficulty.
- Change the measurement conditions according to the purpose of the experiment. For example, to investigate the effect of dual task interference in a grip and lift task, adjust the measurement conditions as follows depending on the type of interference.
- For postural interference, have the participant stand in front of a table and adjust the table height. Give the participant verbal instructions as follows: “Stand on one leg, and use minimal force with your thumb and index finger to lift the iron cube approximately 5 cm above the setting stand. Hold it for 5−7 s and then place it back on the setting stand.”
- For visual interference, have the participant sit in front of a table and adjust the table height. Give the participant verbal instructions as follows: “Close your eyes. Use minimal force with your thumb and index finger with to lift the iron cube approximately 5 cm above the setting stand. Hold it for 5−7 s and place it back on the setting stand.” Allow participants to touch the sensors without exceeding 0.5 N before closing their eyes.
- For cognitive interference, have the participant sit in front of a table and adjust the table height. Give the participant verbal instructions as follows: “As a calculation task, continuously subtract 7 from 100 as accurately as possible. While performing the calculation, use minimal force with your thumb and index finger to lift the iron cube approximately 5 cm above the setting stand. Hold it for 5−7 s and place it back on the setting stand.”
- For contralateral hand movement interference (Figure 2), have the participant sit in front of a table and adjust the table height. Place the peg board 30 cm from the participant in the midsagittal plane next to the iron cube and consider the size and number of pegs to adjust the task difficulty. Give the participant verbal instructions as follows: “Manipulate the iron cube with minimal force using your thumb and index finger. Lift and hold the iron cube approximately 5 cm above the setting stand with one hand, and invert the peg using the other hand. Repeat using the opposite hand.”
3. Data analysis
- Analysis of grip force
- Start the software on the computer. Click File | Open Movie, select the movie file for analysis and Open.
- As the recorded pressure distribution map appears, click Multiple Window View on the map and refer the graph 1 window. Find the point in time which the load (grip force) starts to be applied in each lift, and note the time with reference to this graph.
- After that, save the grip force data in ASCII format. Select File | Save ASCII after making the graph 1 window activated. In the object-graph 1 dialog box, select Panes with the file name and click Save ASCII. In the dialog box, select Save Force, Pressure, and Area values. Specify Force in the Y-axis box, Time in the X-axis box, and Absolute in the Y-mode. Click OK in the property dialog box. Enter the ASCII file name and click Save in the dialog box.
- If information on the contact areas between finger pulps and sensor sheets is needed, specify Contact Area in the Y-axis box and click OK. Enter the ASCII file name and click Save in the dialog box.
- Next, open the movie file. Confirm that the file is opened in spreadsheet format and Frames, Time, Absolute time, Raw Sum and Force are noted. With reference to the time noted in step 3.1.2., find a cell which the load starts to be applied; the load values starts to increase and exceed 0.5N in the force row.
- Calculate the total grip force used in a range, which is the sum of the values from the cell was applied in the force line.
- Analysis of center of pressure
- Start the software. Click File | Open Movie, select the movie file for analysis and click Open.
- With the pressure distribution map active, click Play Forward to play the movie. Make sure that the COP trajectory appears on the pressure distribution map. Find the frame which the COP starts to appear in each lift with Next Frame or Previous Frame, which are the commands to move forward or backward the frames. Then, note that frame number.
- After that, save the COP data in ASCII format. Select File | Save ASCII with the distribution map active. Specify Center of Force in the data type dialog box and Whole movie in the movie range dialog box. Click OK in the property dialog box. Enter the ASCII file name and click Save in the dialog box.
- Next, open the movie file. Confirm that the file opens in spreadsheet format and COMMENTS Frame, Time, Absolute time, Row, Col and Raw Sum are noted. With reference to the frame noted in steps 3.2.2., find a cell (1) which the COP starts to appear.
- Calculate the COP trajectory length between frames. Select a cell (2) after the row including the frame which the COP starts to appear. Insert the following calculation formula: (=SQRT((Row cell (2) -Row cell (1))^2+(Col cell (2) -Col cell (1))^2). The sum of the COP trajectory length between frames in a range is the total COP trajectory within that range.
NOTE: In the graph 1 window, the vertical line shows the load value (N), and the horizontal line shows the time (s). This load value corresponds to the grip force. Data saved in ASCII format can be used in applications such as spreadsheets and text editors. In this experiment, the participants were instructed to hold the cube for 5−7 s in the task, so the grip force and COP trajectory were calculated and recorded for 4 s from their first appearance. In the spread sheet of the COP data, the position of the COP on X- and Y-axis coordinates is shown as a value.
Representative Results
Several studies have introduced experimental protocols and two kinetic parameters (the COP trajectory and the GF) to measure finger force during manipulation of an object. In previous studies, it was found that the COP trajectory increased in stroke patients9. In cervical myelopathy patients, the GF correlated with the cutaneous pressure threshold and upper extremity function10. In healthy young subjects, the GF increased with cognitive interference11. Similar exaggerated GF was found in contralateral hand movement interference. Figure 3 shows the COP trajectories and the GF traces of the dominant index finger in single and dual tasks for representative young and elderly adults. The GF increased in the contralateral hand movement interference. In contrast, the COP trajectories tended to decrease (unpublished data).
Kurihara et al.9 investigated the grip force coordination of grasping in stroke patients. They found that the COP trajectory increased in the paretic hand, although the GFs were not significantly different from the nonparetic hand. Hemorrhagic patients showed longer COP trajectories of the thumb and index finger compared to those in ischemic patients. They also found that the kinetic parameters were correlated with not only somatosensory function, but also cognitive function.
In cervical myelopathy patients, Noguchi et al.10 evaluated the kinetic characteristics of individual finger grip force and investigated the relationship between the grip force and upper extremity function. They found that the GF was associated with the severity of hand dysfunction. Although there was no significant correlation in pinch power or grip power, there was a positive correlation between the GF and the cutaneous pressure threshold.
Lee et al.11 investigated dual task interference in a grip and lift task. They reported that the GF increased in both hands mainly due the dual cognitive task. They also found a correlation between the perceived difficulty and maximum grip force in the dominant hand.
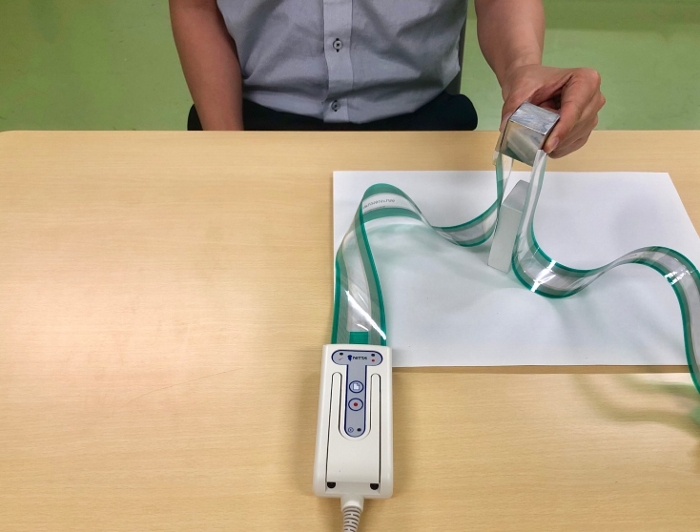
Figure 1: Grip and lift task. Participants gripped the cube using the thumb and index finger, lifted it approximately 5 cm, and held it for 5−7 s. Please click here to view a larger version of this figure.
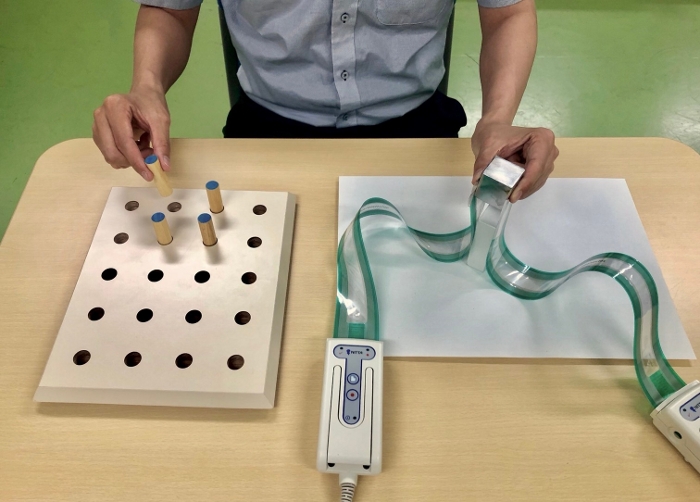
Figure 2: Dual task interference with contralateral hand movement. Participants performed a grip and lift task with one hand and simultaneously conducted a peg test with the other. Please click here to view a larger version of this figure.
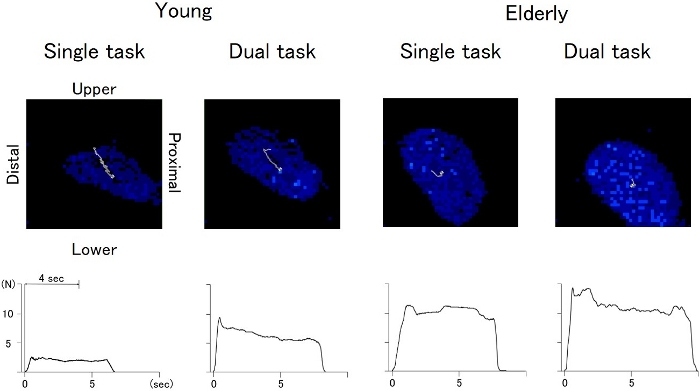
Figure 3: COP trajectories and the GF traces of the dominant index finger in single and dual tasks for representative young and elderly adults. Please click here to view a larger version of this figure.
Discussion
This experimental procedure provides evidence that a flexible pressure sensor sheet could be useful for evaluating spatial stability during precision grip. Altered grip force direction represents grasping spatial instability such as a finger slip. However, existing load cell-type force direction instruments have a limitation in terms of ensuring a natural reach-to-grip movement. To resolve this technical problem, the COP trajectory of the area between the finger pulps and contact surface based on a biomechanical relationship was monitored. The results suggest that the COP displacement is caused by deviated force direction. Thus, the study found that the COP trajectory length is a useful kinetic parameter for evaluating the spatial stability in a precision grip.
A critical factor influencing the outcome of the experiment was each participant’s understanding of the experimental protocol. If participants did not understand the aim of the experiment, they tended to use a relatively large GF in order to avoid spatial instability. Intentionally exaggerated GF interferes with the evaluation of precision grip. Another factor influencing the outcome can be the area between the fingertip and contact surface of the object. If the fingertip is not properly in contact with the surface of the object, the COP is not estimated appropriately. During practical trials, the examiner must adjust the location and orientation of the cube. When the cube is not placed properly, the fingertip protrudes from the edge of the cube, or participants tend to increase trunk and shoulder movements to compensate for hand orientation for grasping.
One limitation of the protocol is the unclear biomechanics of the COP. A slip, roll, or twist between the finger pulps and contact area can account for COP displacement, resulting in spatial instability. This is because the COP is calculated in the X- and Y- axes. Moreover, it is technically difficult to link the two COPs of the thumb and index fingers. Although there are limitations, it is clear that there are benefits to evaluating the spatial stability of grasping using the COP trajectory.
Disclosures
The authors have nothing to disclose.
Acknowledgements
We thank Mr. T. Nishida (Technician, Dept of Sales, Division of Device Performance Materials, Nitta Co., Ltd, Osaka, Japan.) for technical support.
Materials
| Alcohol swab | Wipe participant’s finger pulps | ||
| Compressor | Nitta Corporation | Apply pressure to the sensor seats | |
| Computer | |||
| Controller of compressor | Nitta Corporation | Use to manupirate the compressor | |
| Double-sides tapes | Use to attach the sensorseats to the iron cube | ||
| Iron cube | 150-250g, 30×30×30 mm | ||
| Sensor connector | Connect the sensorseats to computer. | ||
| Sensor sheet | Pressure Mapping Sensor 5027, Tekscan, South Boston, MA, 50 USA | ||
| Setting stand | Set the iron cube on it during the measurement | ||
| Software; I-SCAN 5027, Ver. 7.51 | Nitta Corporation | ||
| Table | Use for the measurement |
References
- Johansson, R. S., Flanagan, J. R. Coding and use of tactile signals from the fingertips in object manipulation tasks. Nature Reviews Neuroscience. 10 (5), 345-359 (2009).
- Cole, K. J. Grasp force control in older adults. Journal of Motor Behavior. 23 (4), 251-258 (1991).
- Lang, C. E., Schieber, M. H., Nowak, D. A., Hermsdörfer, J. Stroke. Sensorimotor control of grasping. , 296-310 (2009).
- Johansson, R. S., Westling, G. Roles of glabrous skin receptors and sensorimotor memory in automatic control of precision grip when lifting rougher or more slippery objects. Experimental Brain Research. 56 (3), 550-564 (1984).
- Parikh, P. J., Cole, K. J. Handling objects in old age: forces and moments acting on the object. Journal of Applied Physiology. 112 (7), 1095-1104 (2012).
- Augurelle, A. S., Smith, A. M., Lejeune, T., Thonnard, J. L. Importance of cutaneous feedback in maintaining a secure grip during manipulation of hand-held objects. Journal of Neurophysiology. 89 (2), 665-671 (2003).
- Monzée, J., Lamarre, Y., Smith, A. M. The effects of digital anesthesia on force control using a precision grip. Journal of Neurophysiology. 89 (2), 672-683 (2003).
- Fortier-Poisson, P., Langlais, J. S., Smith, A. M. Correlation of fingertip shear force direction with somatosensory cortical activity in monkey. Journal of Neurophysiology. 115 (1), 100-111 (2016).
- Kurihara, J., Lee, B., Hara, D., Noguchi, N., Yamazaki, T. Increased center of pressure trajectory of the finger during precision grip task in stroke patients. Experimental Brain Research. 237 (2), 327-333 (2018).
- Noguchi, N., et al. Grip force control during object manipulation in cervical myelopathy. Spinal Cord. , (2020).
- Lee, B., Miyanjo, R., Tozato, F., Shiihara, Y. Dual-task interference in a grip and lift task. The Kitakanto Medical Journal. 64 (4), 309-312 (2014).
