The arthritis index score and paw thickness increased after modeling. Compared with the control group, the toes of the RA model group began to show red swelling at 6 days after modeling, with gradual aggravation. At 14 days, the red swelling in the ankle joint peaked, followed by gradual relief. The thickness of the paw changed similarly (P < 0.05) (Figure 1).
The inflammatory cell infiltration increased significantly after modeling. The pathological results showed that the infiltration degree of inflammatory cells in the ankle synovial tissue of the RA model mice was different at different stages. Peak inflammation occurred on day 14 post modeling (Figure 2).
Inflammatory cytokines increased and anti-inflammatory cytokines decreased in the serum. In the RA model group, the serum levels of pro-inflammatory cytokines (TNF-α, IFN-γ, and IL-6) significantly increased (P < 0.05), while anti-inflammatory cytokines (IL-4 and IL-10) significantly decreased (P < 0.05) (Figure 3).
The iNKT cells obtained by in vivo induction and in vitro purification mainly consisted of iNKT2 cell subsets, which secrete anti-inflammatory cytokines. Intraperitoneal injection of α-GalCer increased the frequency of iNKT cells in the body, predominantly the iNKT2 subgroup. The frequency of spleen iNKT cells in normal DBA/1 mice was about 2% of the lymphocytes, (iNKT2 was about 5%, iNKT1 about 15%, iNKT17 about 10%). Three days after the intraperitoneal injection of α-GalCer, the frequency of iNKT cells was about 6% of the lymphocytes, (iNKT2 was about 82%, iNKT1 about 1.5%, and iNKT17 about 0.5%). After purification by MACS, the purity of iNKT cells was over 85%, of which iNKT2 was about 92%, iNKT1 about 0.4%, and iNKT17 about 0.2% (Figure 4).
The harvested iNKT cells secreted more anti-inflammatory cytokines and fewer inflammatory cytokines. The iNKT cells were isolated from the spleens of normal mice and intraperitoneally injected with α-GalCer 3 days after the mouse spleen (α-GalCer group) and the cytokine levels in the cell culture supernatant were examined. Compared with the control group, the inflammatory cytokines (IL-17A, TNF-α, IFN-γ, and IL-6) of the α-GalCer group significantly decreased (P < 0.05), and the anti-inflammatory cytokine IL-4 level significantly increased (P < 0.05). There was no significant difference in IL-10 (P > 0.05). The IFN-γ/IL-4 ratio significantly decreased (P < 0.05) (Figure 5).
IVIS tracing confirmed that DiR-iNKT cells were adoptively infused into RA mice and immediately appeared in the lungs postinjection. Fluorescence was detected in the liver at 10 min and in the spleen at 60 min (Figure 6AI, 6AII, 6AIII). In the isolated organs, there was no fluorescence in the thymus and inguinal lymph nodes within 1 h. Fluorescence was detected in the lungs at 0 min, the fluorescence intensity was the greatest at 10 min, and then gradually weakened. There was weak fluorescence in the liver at 0 min, and then it gradually increased. The fluorescence in the spleen was detected at 30 min and then gradually increased (Figure 6AIV, 6C).
After the infusion of DiR-iNKT cells into RA mice, fluorescence was mainly concentrated in the liver and spleen (Figure 6BI, 6BII, 6BIII), but there was no fluorescence in the thymus and inguinal lymph nodes. The spleen and liver had the highest fluorescence intensity on day 1 after cell infusion, but it gradually weakened. On day 34, the surface fluorescence disappeared. On day 42, the fluorescence of the isolated organs disappeared. The average fluorescence signal intensity of liver after the cell infusion was higher than that of the spleen (Figure 6BIV, 6D).
Adoptive infusion of iNKT cells into RA mice can alleviate disease progression and improve clinical symptoms. The iNKT cells improved the clinical symptoms of RA mice after adoptive infusion. Compared with the untreated RA model group, the swelling of the ankle joint was relieved in the cell treatment group, and the scores significantly decreased from day 10 to day 20 postinjection. In the same period in the cell treatment group, inflammatory cell infiltration in the synovial tissue was reduced in comparison to the RA model group (Figure 2).
The success rates of thymus iNKT cells increased significantly (P < 0.05). Compared with the healthy control group, in the RA model group the rates of iNKT cells in the thymus decreased at the progress (day 11), peak (day 14), and recovery (day 20) stages. At peak inflammation, these values were minimal and rebounded in the remission phase. The cell therapy group showed significantly increased rates of iNKT cells at the peak (day 14) and recovery (day 20) stages in comparison with the RA model group (P < 0.05) (Figure 7).
After iNKT cell infusion, the success rate of iNKT1 and iNKT17 in the thymus decreased and iNKT2 increased. Compared to the control group, in the RA model group on day 11 iNKT1 and iNKT17 in the thymus significantly increased (P < 0.05), and iNKT2 significantly decreased (P < 0.05). On day 14, iNKT1 and iNKT2 in the thymus significantly increased (P< 0.05) and iNKT17 significantly decreased (P< 0.05). On day 20, iNKT1 in the thymus significantly increased (P < 0.05), iNKT2 did not significantly change (P > 0.05), and iNKT17 significantly decreased (P < 0.05). The iNKT1/iNKT2 ratio significantly increased during all three stages (P < 0.05).
Compared to the RA model group, on day 11 in the α-GalCer and the cell therapy groups, iNKT1 and iNKT17 were significantly lower (P < 0.05) and iNKT2 significantly increased (P < 0.05). On day 14, in the α-GalCer group iNKT1 and iNKT17 significantly decreased (P < 0.05), and iNKT2 did not significantly change (P > 0.05); in the cell therapy group iNKT1 and iNKT17 significantly decreased (P < 0.05) and iNKT2 significantly increased (P < 0.05). On day 20, in the α-GalCer group the iNKT1 significantly decreased (P < 0.05), iNKT2 did not change significantly (P > 0.05), and iNKT17 significantly increased (P < 0.05); in the cell therapy group iNKT1 and iNKT17 significantly decreased (P < 0.05) and iNKT2 significantly increased (P < 0.05). The ratio of iNKT1/iNKT2 significantly decreased during all three stages (P < 0.05) (Figure 7).
The levels of inflammatory cytokines were increased in serum and the anti-inflammatory cytokines were decreased after iNKT cell infusion. In the RA model group, the levels of TNF-α, IFN-γ, and IL-6in serum significantly increased (P < 0.05), while IL-4 and IL-10 showed markedly decreased amounts (P < 0.05) in comparison with the control group. In the iNKT cell therapy group, the levels of TNF-α, IFN-γ, and IL-6 in serum significantly decreased at the progress and peak stages of inflammation (P < 0.05), while IL-4 and IL-10 significantly increased (P < 0.05) in comparison with the RA model group (Figure 3).
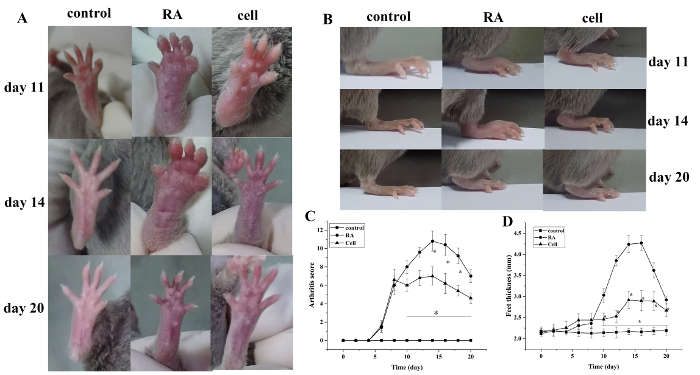
Figure 1: The joint swelling score and paw thickness change in mice. (A) Swelling of the ankle joint in mice. (B,D) Paw thickness in different groups. (C) Clinical score changes in different groups. The mouse arthritis score and the thickness of the paw were significantly reduced in the cell therapy group on days 10–20 (i.e., 2–12 days after treatment) after modeling. *P < 0.05 vs. control, **P < 0.05 vs. RA. Please click here to view a larger version of this figure.
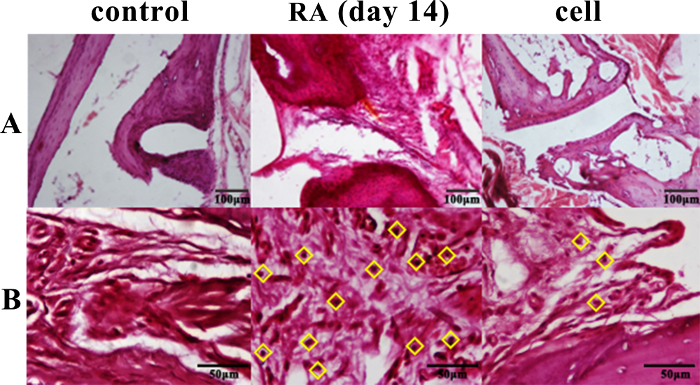
Figure 2: Histopathological changes of the ankle joint. The infiltration of inflammatory cells was significantly reduced in the cell therapy group and was significantly increased in the RA group on day 14. ◊ = inflammatory cells. (A) 100x (B) 400x. Please click here to view a larger version of this figure.
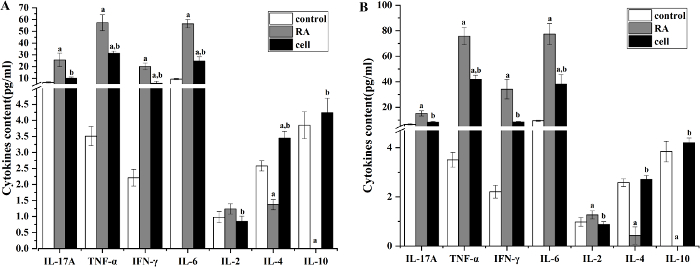
Figure 3: The levels of serum cytokines in each group. (A) Serum cytokines levels in mice on day 11 after modeling (pg/mL). (B) Serum cytokines levels in mice on day 14 after modeling (pg/mL). The levels of TNF-α, IFN-γ, and IL-6 significantly decreased, and the levels of IL-4 and IL-10 significantly increased in the cell therapy group. aP < 0.05 vs. control. bP < 0.05 vs. RA. Please click here to view a larger version of this figure.
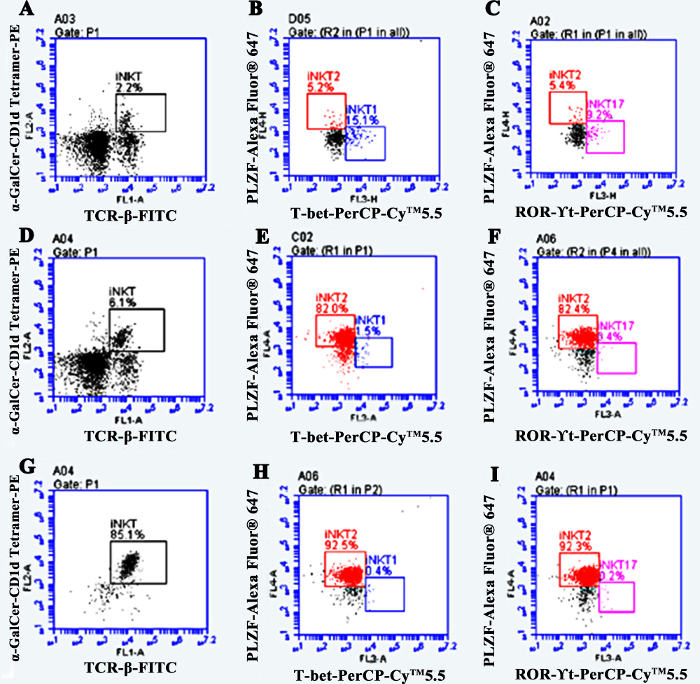
Figure 4: The rates of iNKT cells and proportion of iNKT cell subsets. (A,B,C) The rate of iNKT2 in normal mice is ~5%. (D,E,F) The rate of iNKT2 is about 82% after in vivo induction. (G, H, I) The rate of iNKT2 is more than 92% after MACS purification. Please click here to view a larger version of this figure.
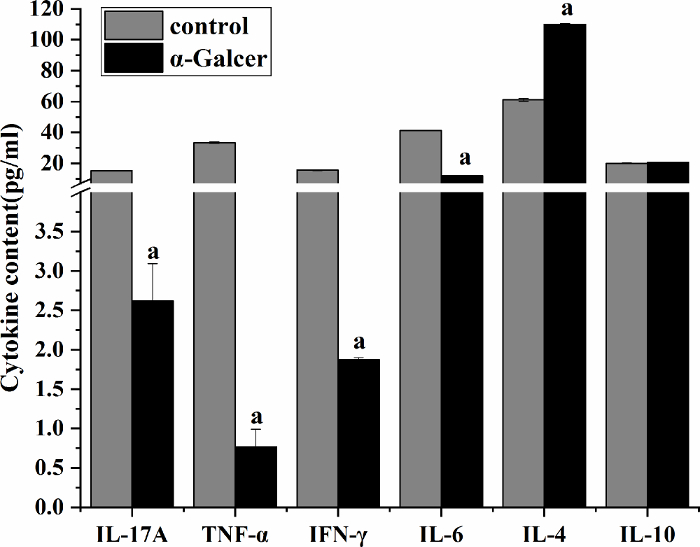
Figure 5: Cytokine levels in culture supernatant of mouse spleen-derived iNKT cells. The level of IL-4 significantly increased, and the levels of IL-17A, TNF-α, IFN-γ, and IL-6 significantly decreased. aP < 0.05 vs. control. Please click here to view a larger version of this figure.
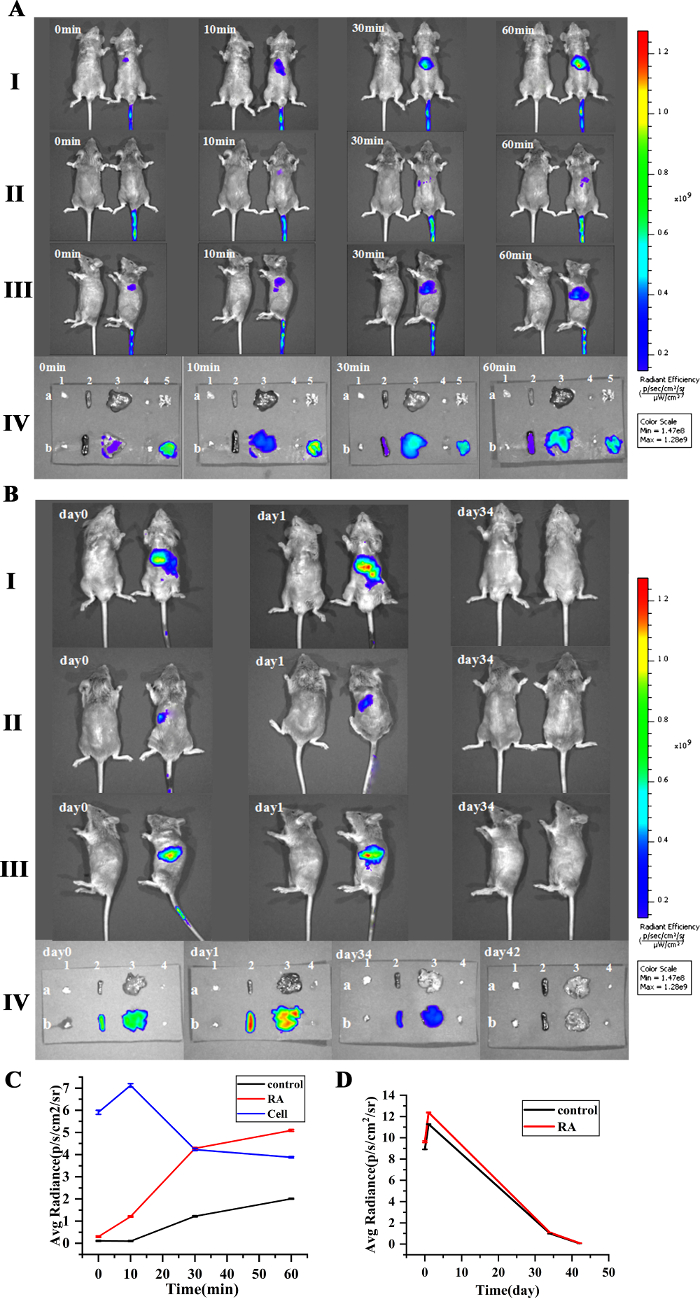
Figure 6: Distribution and metabolism of iNKT cells traced by caliper IVIS lumina II. (A,B) Migration path of iNKT cells. (C) The change of the average fluorescence signal intensity in the spleen, liver, and lung. (D) The change of the average fluorescence signal intensity in the spleen and liver. The fluorescence was detected in the lungs and liver at 0 min, and then gradually increased. The fluorescence intensity was strongest at 10 min in the lungs and then decreased. The fluorescence of the spleen was detected at 30 min, then gradually increased. The fluorescence of all organs disappeared on day 42. The average fluorescence signal intensity of the liver is higher than the spleen after cell infusion (I: supine; II: lateral lying; III: prone; IV: isolated tissue; a: control group; b: cell infusion group; 1, 2, 3, 4, 5 are thymus, spleen, liver, inguinal lymph nodes, lungs). Please click here to view a larger version of this figure.
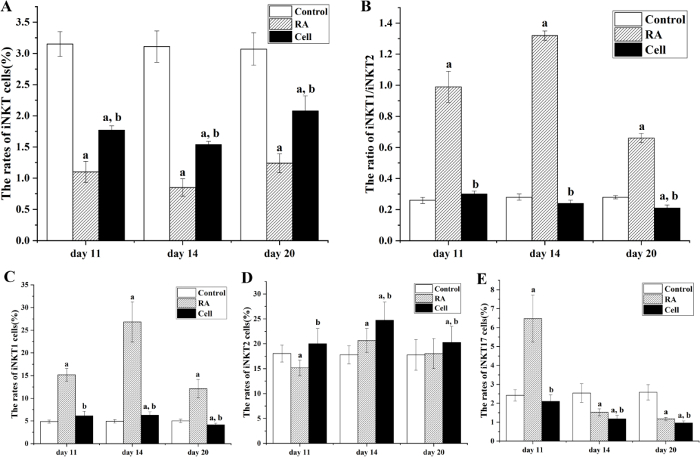
Figure 7: The rates of iNKT and its subsets in the mouse thymus. (A) The rates of iNKT cells at 11, 14, and 20 days after modeling. (B) The ratio of iNKT1/iNKT2. (C,D,E) The rate of iNKT1, iNKT2, and iNKT17. On days 11, 14, and 20 (days 3, 6, and 12 after cell therapy), the rates of iNKT cells significantly increased, the iNKT1 and iNKT17 of the thymus significantly decreased in the cell therapy group, and iNKT2 was significantly increased. aP < 0.05 vs Control. bP < 0.05 vs RA. Please click here to view a larger version of this figure.
