Using the abovementioned procedure for a MCAO/R model with a Longa's score and TTC staining, different treatments of average weight (275/300/320 g), bolt types (2636/2838/3040/3043; Table 1) and ischemic times (2-3 h) and 1 day reperfusion were used to screen for the optimal brain ischemia model in rats. Model parameters of 300 g weight, 3040 thread bolt, and 3 h brain infarct time were the most suitable for the largest cerebral infarction, highest Longa's score and greatest model success ratio. This was significantly improved on the conventional treatment of a 275 g weight, 2636 thread bolt, and 2 h brain infarct time (Figure 1).
Furthermore, rats with 300 g weight, 3040 thread bolt, 3 h brain infarct time and a 2−3 Longa's score underwent sensorimotor function tests (a bilateral asymmetry test, a grid-walking test, a rotarod test, and a lifting rope test) and TTC staining to study the recovery status of brain ischemia from 1-90 days. The infarct and shrink volume were 23.4%, 19.6%, 16.1% (P < 0.01, compared with the first day) and 15.7% (P < 0.01, compared with the first day) after 1, 35, 60, and 90 days post MCAO/R, respectively (Figure 2). On the first day after MCAO/R, infarct volume was biggest. In time, the infarct volume became smaller and the shrink volume became larger. The infarct and shrink volume no longer changed after 60 days of MCAO/R.
The sensorimotor bias in the bilateral asymmetry test, the grid-walking error times in the grid-walking test and the lifting rope score in the lifting rope test all significantly increased, while the rotarod time in the rotarod test decreased significantly after 1 day of MCAO/R (Figure 3), which indicated that all four tests were meaningful in the stage of acute brain ischemia. However, only sensorimotor bias maintained large functional disorders with a time-dependent manner after 35, 60 and 90 days of MCAO/R. There were significant differences of grid-walking error times in the grid-walking test after 35 and 60 days of MCAO/R. These results indicated that the bilateral asymmetry test and the grid-walking test could be suitable sensorimotor function tests for the stage of recovery and sequela in rats.
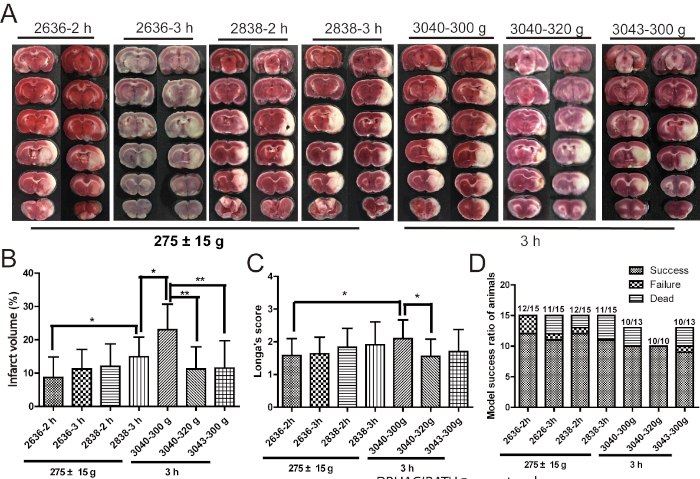
Figure 1: 300 g weight, 3040 thread bolt, 3 h brain infarct time may be the optimum condition of the brain ischemic injury induced by MCAO/R. (A,B) Pictures and cartogram of infarct volume of brain tissue (n = 9−12). (C) Longa's score (n = 9−12). (D) The statistics of model success ratio of rats (n = 10−15). Model success ratio = (total number of rats – death rats after MCAO/R – failure rats after MCAO/R)/total number of rats. Failure rats are the model rats that do not have a suitable Longa's score. Error bars represent S.D., *P < 0.05, **P < 0.01. This figure has been modified from Liu et al.15. Please click here to view a larger version of this figure.
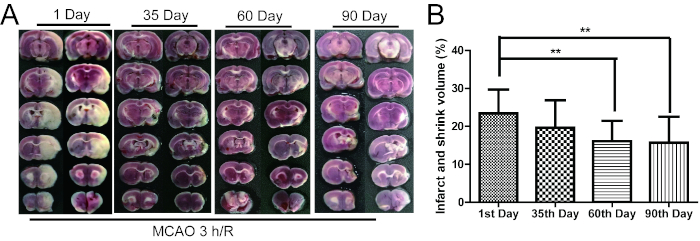
Figure 2: The infarct and shrink volume gradually decreased from 1 to 90 days after MCAO/R. (A) The TTC staining of rat brain tissue. (B) The cartogram of infarct and shrink volume (n = 16−19). Error bars represent S.D., **P < 0.01 vs. the first day after MCAO/R. This figure has been modified from Liu et al.15. Please click here to view a larger version of this figure.
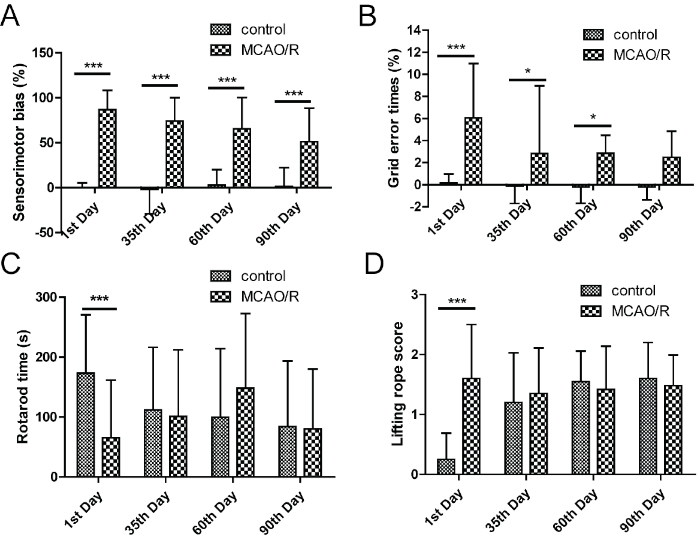
Figure 3: Bilateral asymmetry test and grid-walking test were the suitable sensorimotor function tests in the recovery and sequela stage of brain ischemia. (A) The right limb tearing favorability in debonding experiment. (B) The grid-walking error times in grid-walking test. (C) The length of time in rotarod test. (D) The score in lifting rope test. Error bars represent S.D., n = 15−19, *P < 0.05, ***P < 0.001. This figure has been modified from Liu et al.15. Please click here to view a larger version of this figure.
| Type | The diameter of thread bolt | The diameter of thread bolt head | Recommended weight of rat | Level |
| 2636 | 0.26 mm | 0.36 mm | 250-280 g | A4 |
| 2838 | 0.28 mm | 0.38 mm | 280-350 g | A4 |
| 3040 | 0.30 mm | 0.40 mm | 360-400 g | A4 |
| 3043 | 0.30 mm | 0.43 mm | >400 g | A4 |
| Note: A4 level thread bolt is the standard that the head end is hemispherical, the front end is covered with poly-lysine, marked, sterilized, and buy-on-use without any treatment (This Table has been modified from Liu et al., 2018). | ||||
Table 1: Thread blot information. This table has been modified from Liu et al.15.
