Animal studies were conducted with the consent of the Local Ethical Committee (28/ŁB29/2016) in accordance with Directive 2010/63/EU of the European Parliament and of the Council of September 22, 2010, and institutional recommendations.
1. TNBS-induced murine model of Crohn's disease
NOTE: This protocol uses male BALB/C mice weighing 25-28 g. Animals are housed at a constant temperature (22-24 °C) and, relative humidity 55 ± 5%, and maintained in a 12 h light/dark cycle with free access to standard chow pellets and tap water ad libitum.
- Place the mouse into the induction chamber and close the lid tightly. Anesthetize the mouse briefly with isoflurane (25% O2 with O2 flow rate at 1.5-2 L/min).
NOTE: Respiratory rate should remain rhythmic and slower than normal and should not change in response to a noxious stimulus. - Instill 4 mg of TNBS in 0.1 mL of 30% ethanol in 0.9% NaCl or 0.1 mL of 30% ethanol in 0.9% NaCl as a vehicle control into the distal colon through a catheter.
NOTE: The catheter should be carefully introduced approximately 3 cm into the anus. - Monitor the mouse daily from day two to eight for clinical parameters including body weight, rectal bleeding, stool consistency and mortality.
- On day eight, euthanize the mouse by cervical dislocation.
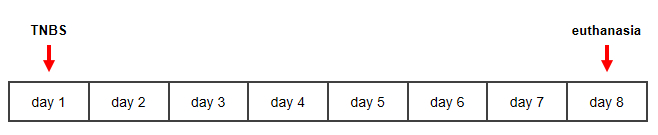
Figure 1: Timeline for TNBS-induced murine model of Crohn's disease. Please click here to view a larger version of this figure.
2. Separation and macroscopic evaluation of colon
NOTE: One day before colon separation, dilute 100 µL of antibiotic in 1 mL of phosphate buffer saline (PBS) and leave at 4 °C overnight.
- Clean the skin over the abdomen using 75% ethanol and sterile gauze.
- Cut the abdominal wall from breastbone to anus using sterile scissors and tweezers.
- Cut off the colon as close as possible to the anus and cecum.
- Place the colon on the Petri dish. Cut the colon along from the anus into the cecum end. Clean and wash the colon 2-4 times in cold antibiotic-PBS solution.
- Perform macroscopic evaluation using a caliper according to Table 1.
NOTE: Tissue adhesion* and erythema/hemorrhage#, fecal blood# and diarrhea# are subject to visual assessment. *Tissue adhesion evaluate using a three-point scale (0: colon without tissue adhesion, 1: colon with moderate tissue adhesion, 2: colon with extensive tissue adhesion); #based on absence (0) or presence (1) of erythema/hemorrhage, fecal blood and diarrhea.
| Adhesion* | Erythema/ hemorrhage# | Fecal blood# | Diarrhea# | Length of ulcer | Colon thickness | Colon length |
| points (0 – 2) | points (0 – 1) | points (0 – 1) | points (0 – 1) | cm/points | mm/points | cm/points |
| 0 – absent | 0 – absent | 0 – absent | 0 – absent | 0.5 cm = 0.5 point | n mm = n points | 0 – <10% shorter than the control |
| 1 – moderate | 1 – present | 1 – present | 0.5 – slight/loose stool | 1 – from 10 to 20% shorter than the control | ||
| 2 – present | 1 – present | 2 – over 20% shorter than the control |
Table 1: Macroscopic scoring of the intestine of mice with TNBS-induced model of Crohn's disease.
- Convert the length of the ulcer in centimeters to a point scale, i.e., every 0.5 cm of ulcer is counted as 0.5 point. Convert the thickness of the colon in millimeters to a point scale, i.e., every n mm corresponds to n points.
- Convert the length of the colon in centimeters on a three-point scale. The length of colon obtained from each mouse with TNBS-induced Crohn's disease is evaluated in relation to the average colon length for the control group (0: <10% shorter than the control, 1: from 10 to 20% shorter than the control, 2: over 20% shorter then the control).
- Calculate the total macroscopic score according to the equation: Total macroscopic score = adhesion (points) + erythema/hemorrhage (points) + fecal blood (points) + diarrhea (points) + length of ulcer (points) + colon thickness (points) + colon length (points).
3. Colon sample preparation
- Cut the colon into 1-2 cm fragments and place each on sponge in an appropriately labeled histological cassette.
NOTE: Sponges for histological cassettes prevent colon folding during dehydration and incubation in liquid paraffin. - Place the colon fragment in 4% formaldehyde and incubate for at least 24 h at 4 °C.
- Prepare and program the tissue processor for 1 h of incubation in 50%, 70%, 90%, 95%, 100% ethanol, xylene/100% ethanol (1:1; v/v), and xylene only, as well as for at least 3 h of incubation in liquid paraffin.
NOTE: Dehydration must be performed in increasing concentrations of ethanol and xylene, but the concentration of ethanol can be modified. The xylene/ethanol mixture is recommended but not required. - Transfer the colon fragment to a histological box and place in the pre-programmed tissue processor.
- Run the tissue processor.
- After incubation steps, place the colon fragment in a metal mold so that the two ends of the colon are in an upright position and fill one third of the mold with liquid paraffin.
- Place the mold in the cooling area (-5 °C) for a few seconds, and then move the mold to the warming area (70 °C). Place in the bottom part of the histological box and cover the entire colon fragment with liquid paraffin.
- Leave the metal mold with the colon fragment in paraffin for a few minutes in the cooling area. Remove the metal mold from the paraffin block and incubate for at least 24 h at 4 °C.
- Remove excess paraffin from the block and insert it into a fully automated rotary microtome.
NOTE: The paraffin block may be stored at -20 °C for a few minutes before this step. - Cut the colon fragment into 5 µm sections.
- Transfer the colon section to a water bath preheated to 40 °C.
- Use the labeled glass slide to remove the colon section from the water bath.
NOTE: The colon sections float on the water. Put the labeled glass slide in the water under the colon section and withdraw the glass slide carefully. - Leave the glass slide for 24 h at room temperature. For long term storage, keep the glass slide at 4 °C after 24 h of incubation at room temperature.
4. Immunohistochemistry with immunofluorescence staining
NOTE: Do not allow the colon section to dry at any step during the procedure.
- Remove paraffin by incubating the glass slide in xylene for 5 min. Repeat this step three times.
- Place the glass slide in xylene/100% ethanol (1:1; v/v) for 5 min. Repeat this step three times.
- Rehydrate the colon section in a series of decreasing ethanol concentrations, i.e., 70%, 50%, 30% and 10% ethanol for 5 min. Repeat each step three times.
- Rinse the glass slide under running water for 5 min.
- Preheat antigen retrieval buffer (10 mM sodium citrate; 0.05% Tween 20, pH 6.0) to 95-98 °C and heat the glass slide in boiling antigen retrieval solution for 10 min.
NOTE: The antigen retrieval step is optional but recommended. The unmasking solution should be optimized depending on the antibody used in the experiment. - Draw a circle around the colon section using a hydrophobic pen.
NOTE: This step is optional but recommended. The hydrophobic pen prevents waste of reagents by keeping the liquid pooled in a small volume inside marked the circle. - Incubate the section in 3% water solution of hydrogen peroxidase for 10 min.
- Wash in washing solution (50 mM Tris-HCl, pH 7.4; 150 mM NaCl; 0.05% Tween 20) for 5 min.
- Incubate in blocking solution (5% normal goat serum; 50 mM Tris-HCl, pH 7.4; 150 mM NaCl; 0.05% Triton X-100) for 1 h at room temperature.
NOTE: In the blocking solution, the normal serum must be from the same species as the secondary antibody. In stages where incubation is required, place the glass slide in a humidity chamber to prevent excessive evaporation. - Remove the blocking solution and add 20-50 µL of primary antibody against ERα, ERβ or GPER diluted in 1% bovine serum albumin with 50 mM Tris-HCl, pH 7.4, 150 mM NaCl, 0.05% Triton X-100.
NOTE: Recommended dilutions of primary antibodies are shown in Table 2.
| Antibody type | Antibody against | Clonality | Host species | Species reactivity | Dilution |
| Primary | ERα | Polyclonal | Rabbit | Human | 1:100 |
| Mouse | |||||
| Turtle | |||||
| Capybara | |||||
| ERβ | Polyclonal | Rabbit | Human | ||
| Monkey | |||||
| Rat | |||||
| Mouse | |||||
| Sheep | |||||
| Pig | |||||
| GPER | Polyclonal | Rabbit | Human | ||
| Rat | |||||
| Mouse | |||||
| Secondary | DyLight 650 | Polyclonal | Goat | Rabbit | 1:250 |
Table 2: Characteristics of antibodies.
- Incubate with primary antibody overnight at 4 °C in darkness.
- Remove the antibody solution and wash in washing solution (50 mM Tris-HCl, pH 7.4; 150 mM NaCl; 0.05% Tween 20) for 5 min. Repeat this step three times.
- Add 20-50 µL of DyLight 650 secondary antibody diluted in 1% bovine serum albumin (containing 50 mM Tris-HCl, pH 7.4, 150 mM NaCl, 0.05% Triton X-100). Incubate with secondary antibody conjugated with dye for 1 h at room temperature in darkness.
NOTE: The recommended dilution of the secondary antibody is shown in Table 2. - Remove the antibody solution and wash in washing solution (50 mM Tris-HCl, pH 7.4, 150 mM NaCl, 0.05% Tween 20) for 5 min. Repeat this step three times.
- Add 2% DiOC6(3) diluted in 50 mM Tris-HCl, pH 7.4, 150 mM NaCl and incubate for 10 min at room temperature in darkness.
- Remove the solution and wash in washing solution (50 mM Tris-HCl, pH 7.4, 150 mM NaCl, 0.05% Tween 20) for 5 min. Repeat this step three times.
- Add a few drops of glycerol-based liquid with DAPI directly on the colon section and cover carefully with a cover slide. Incubate the colon section for least 24 h at 4 °C.
NOTE: Avoid air bubbles when covering the tissue with the cover slide. - Analyze the colon section under confocal microscope featuring 20x or 63x objectives and oil immersion using dedicated software.
NOTE: Table 3 lists characteristics of the fluorochromes used in this study.
| Fluorochome type | Wavelength (nm) | Dye | |
| Excitation | Emission | ||
| DAPI | 405 | 460 – 480 | Blue |
| DiOC6 (3) | 485 | 538 – 595 | Green |
| DyLight 650 | 654 | 660 – 680 | Red |
Table 3: Characteristics of fluorochromes.
Macroscopic characteristics of colons in mice with TNBS-induced Crohn's disease
Representative images of colons taken from control and TNBS-treated mice are shown in Figure 2. In mice with a TNBS-induced model of Crohn's disease, the length of the colon is reduced while the width of the colon is increased.

Figure 2: Representative colon obtained from the control mice (control) and TNBS-treated mice (TNBS). Please click here to view a larger version of this figure.
The evaluated macroscopic parameters are given in Table 1. Administration of TNBS to mice leads to an increase in the total colonic macroscopic score (Figure 3A) and inflammation length (Figure 3B) relative to the control mice.
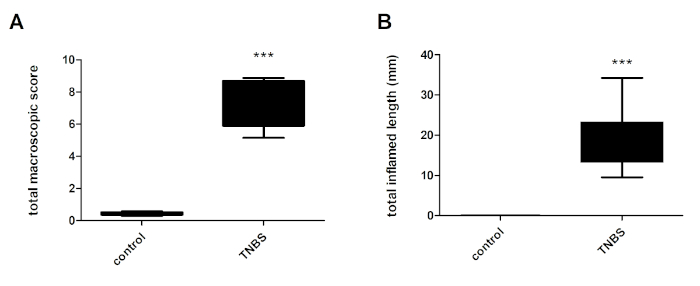
Figure 3: Total macroscopic score of the colon (A) and total colonic inflammation length (B) in control mice (control) and TNBS-treated mice (TNBS). Ten mice per group. Statistical analysis was performed using One-Way ANOVA followed by Newman-Keuls post-hoc test. Data are presented as means ± SEM; ***p < 0.001 TNBS vs. control. Please click here to view a larger version of this figure.
Estrogen receptor antibody validation
Validation of the specificity of the estrogen receptor antibodies used in the study was performed using MCF-7 cells. MCF-7 cells were chosen based on previous studies wherein several independent researchers found that estrogen receptors are present at the mRNA and protein levels. As shown in Figure 4, the antibodies used in the study allow the detection of both nuclear estrogen receptors, i.e., ERα (Figure 4A) and ERβ (Figure 4B), as well as the membrane-bound estrogen receptor, i.e., GPER (Figure 4C) in MCF-7 cells. Nuclear estrogen receptors are localized in the cytoplasm and nuclei, and the signal from GPER staining is only present in the cytoplasm of MCF-7 cells.
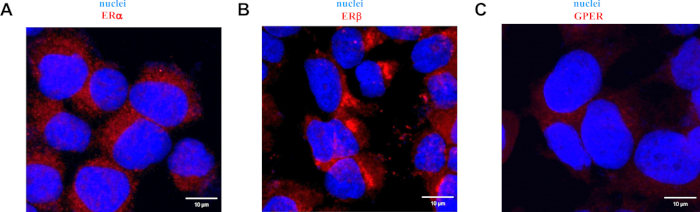
Figure 4: Representative images of immunofluorescence staining of ERα (A), ERβ (B) and GPER (C) in the MCF-7 cells. Detailed description at the top of the images. Scale bars: 10 µm. Please click here to view a larger version of this figure.
In addition to the positive control, a negative control was also performed, in which only the secondary antibody was used. Figure 5 shows an image of MCF-7 cells stained only with secondary antibody conjugated with fluorochrome and glycerol-based liquid with DAPI.
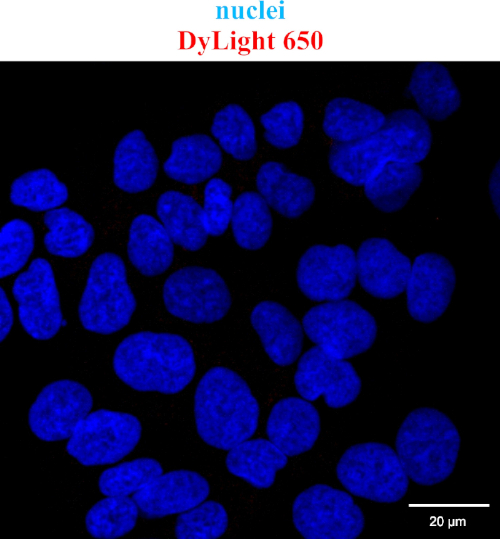
Figure 5: Representative image of immunofluorescence staining of DyLight 650 in the MCF-7 cells. Additional description is available above the image. Scale bars: 20 µm. Please click here to view a larger version of this figure.
Estrogen receptor localization in the TNBS-induced murine model of Crohn's disease
A strong cytoplasmic signal of ERα was found in the colon section obtained from control mice and mice with TNBS-induced Crohn's disease (Figure 6A). However, it appears that only in the intestine obtained from control mice had ERα localized in the goblet cell cytoplasm. Confocal microscopy also revealed cytoplasmic localization of ERβ in the colon section of both control and TNBS-treated mice (Figure 6B). Similarly, cytoplasmic localization of GPER was documented in the colon section obtained from control mice and TNBS-treated mice (Figure 6C).
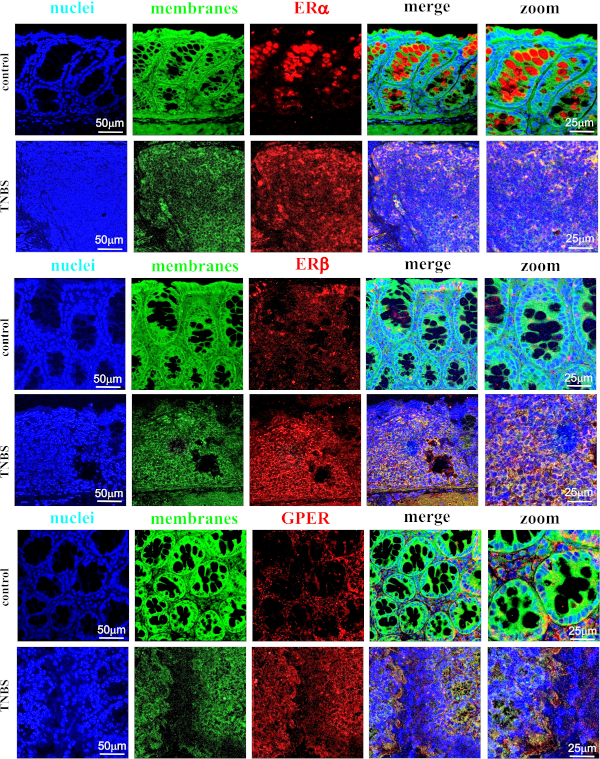
Figure 6: Representative images of immunofluorescence staining of ERα (A), ERβ (B) and GPER (C) in the colon section obtained from control mice (control) and TNBS-treated mice (TNBS). Additional description is available above each image. Scale bars: 50 µm; zoom scale bars: 25 µm. Please click here to view a larger version of this figure.
