This protocol induced bacterial sepsis in neonatal mice, and we used longitudinal intravital imaging, enumeration of bacteria in the blood, histological assessments of pathology, and inflammatory cytokine expression profiles to study the course of disease. Signs of morbidity were observed in neonatal pups infected with both low (~2 x 106 CFUs) and high (~7 x 106 CFUs) inoculums of E.coli over time. Pups that received the greater inoculum displayed more prominent signs of distress that included reduced mobility, the inability to correct their posture, and impaired ability to maintain an upright position by 24 h post-infection (hpi). There was, however, a range of morbidity as some pups appeared worse than others. Immediately following infection, one low-dose animal died due to isoflurane exposure during an imaging session to establish baseline. By 24 hpi, two of six high-dose animals succumbed to the systemic infection (33.3% mortality). Infected pups that received either a high or low dose inoculum weighed significantly less than their control littermates at 24 hpi (Figure 1A,B). All the pups that received the higher inoculum met endpoint criteria at 24 hpi. As such, all the infected pups in this group were euthanized following imaging. Bacteria in the blood were enumerated for a subset of mice that received the lower inoculum, and for all animals that received the higher inoculum since they were all euthanized. The results from two experiments performed similarly indicate that while most animals had high levels of bacteria in the blood (CFUs/mL) at 24 hpi, some animals did not have detectable bacteria in the blood (Figure 1C). The latter suggest that they cleared the infection by this time point. As expected, pups that received the higher inoculum had nearly three orders of magnitude more CFUs/mL at 24 hpi relative to pups that received the low dose inoculum (Figure 1C).
Live animal imaging of luminescent bacteria further confirmed the dissemination of bacteria and increase in growth in neonatal pups over time at 10 and 24 hpi (Figure 2 and Figure 3). Additionally, using intravital imaging with the microCT, we were able to identify infection foci, including the brain (Figure 2B), lungs (Figure 2B, Figure 3A,B), and other peripheral tissues (Figure 2B). The lungs of some highly infected mice demonstrated opaque regions consistent with inflammatory consolidation that co-localized to luminescent bacterial signal (Figure 3A). These regions of presumed inflammatory exudate are not found in uninfected control lungs (Figure 3A). Further evidence of a pronounced inflammatory cytokine response within the lungs of infected pups is demonstrated by gene expression analysis of IL-1β, IL-6, and TNF-α. A significant increase in expression relative to controls was observed for all three cytokines in both the low and high inoculum groups (Figure 4A). Histopathology of the lung was also examined at 24 hpi in control and infected pups. Despite similar inflammatory cytokine profiles, a progressive increase in pathology was commonly observed from the lower to the higher inoculum. Compared with tissue from uninfected controls, the lungs of infected pups showed notable inflammatory changes, thickening of the alveolar wall, increased alveolar hemorrhaging, and inflammatory infiltration (Figure 4B). In the most severe infections, the pulmonary congestion and areas of hemorrhage contributed to a massive reduction in open air space (Figure 4B). Collectively, these results demonstrate that in our model of early onset neonatal sepsis, dissemination of luminescent bacteria can be followed over time from a subscapular inoculation site to important infection foci and cause significant inflammation and pathology in severely infected animals.
To study host factors that contribute to bacterial killing by innate immune cells such as monocytes, macrophages, and neutrophils, we developed a sensitive in vitro assay to measure bacterial clearance. Ly6B.2+ cells isolated from the spleens of neonatal mice were infected with bioluminescent E. coli at a range of MOIs for 1 h and then treated with gentamicin to kill extracellular bacteria. At 3, 6, 20, and 48 hpi, intracellular luminescence was measured with a multimode reader. As expected, with increasing MOI, more luminescent signal was recorded at 3 h (Figure 5). Gradually, this signal was lost, indicative of bacterial clearance (Figure 5). This assay is amenable to supplemented cytokines, neutralization of secreted effectors, and the addition of pharmacological inhibitors of cellular pathways to study interventions that may promote bacterial clearance and serve to improve outcomes in the neonatal sepsis model described here.
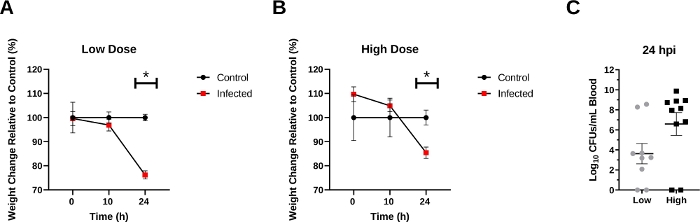
Figure 1: Changes in body weight and bacterial replication in septic neonatal mice.
(A,B) Individual mouse weights within a group (low and high) expressed as a percentage of the mean weight of littermate control pups. Data are presented as mean percentage ± SEM. Individual t-tests at each post-infection time point reveal significant differences at 24 h between control pups and pups that received the low inoculum (p<0.0001) (A), or between control pups and pups that received the high inoculum (p=0.0031) (B). (C) CFU/mL in the blood at 24 hpi were log transformed and presented as the mean ± SEM. Mann-Whitney test reveals a trend towards significance between the low and high dose inoculums (p=0.0882). Please click here to view a larger version of this figure.
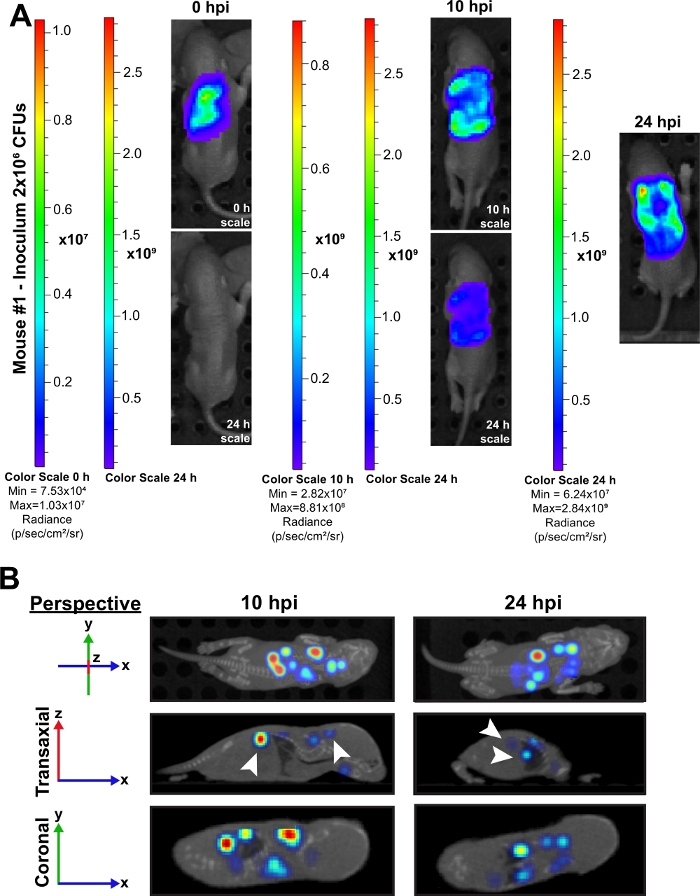
Figure 2: Intravital imaging demonstrates dissemination of bacteria in neonatal mice over time.
(A) A representative neonatal mouse (#1) infected with an inoculum of ~2 x 106 CFUs is shown at time 0, 10, and 24 hpi. A colorimetric scale with the minimum and maximum radiance values per time point are displayed for each time point. Mice at 0 and 10 h are displayed on both their time point scale and the 24 h scale to demonstrate changes in bacterial growth over time. (B) Representative 3D reconstructed microCT images of the same neonatal mouse at 10 and 24 hpi are shown. Each time point has images at overhead, transaxial, and coronal perspectives. In the transaxial image at 24 hpi, the plane has moved toward the periphery of the mouse to better display infection foci in the peripheral tissues. White arrows indicate the brain and kidney at 10 hpi and the kidney and lung at 24 hpi. Please click here to view a larger version of this figure.
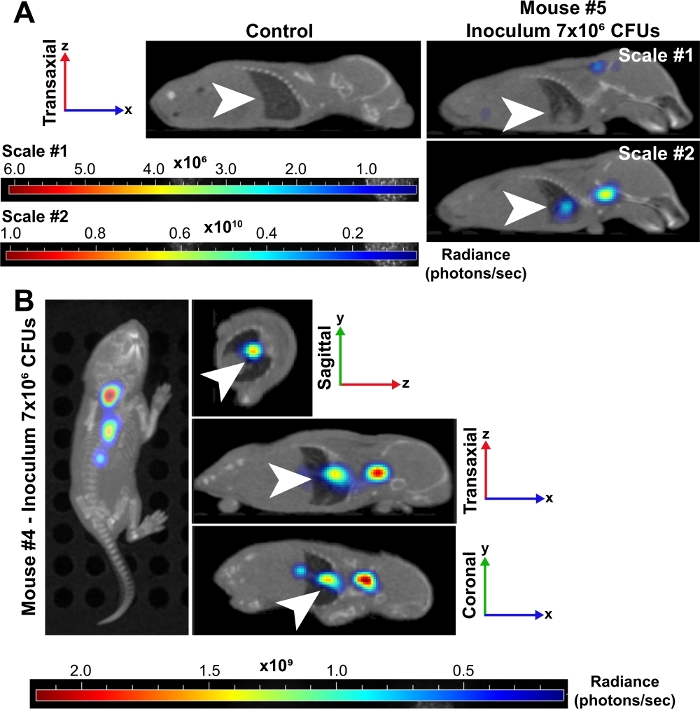
Figure 3: Lungs are a site of major infection during bacterial sepsis in neonates.
(A) Representative 3D reconstructed microCT images of a neonatal mouse (#5) infected with an inoculum of ~7 x 106 CFUs are shown at 24 hpi compared to an uninfected control. Both mice are displayed in the transaxial perspective and lungs are indicated by white arrows. The infected mouse was placed on two radiance (photons/sec) scales. Scale #1 includes all 6 wavelengths (500, 520, 560, 580, 600, 620 nm) and scale #2 includes only 500, 520, and 560 nm wavelengths. This second scale allowed us to visualize an increased signal in bacteria in the lungs because lower wavelengths are more highly absorbed by tissue and produce stronger signal. (B) Representative 3D reconstructed microCT images of a neonatal mouse (#4) infected with an inoculum of ~7 x 106 CFUs are shown at 24 hpi. This time point has images at the overhead, sagittal, transaxial, and coronal perspectives. White arrows indicate infection foci in the lungs. Please click here to view a larger version of this figure.
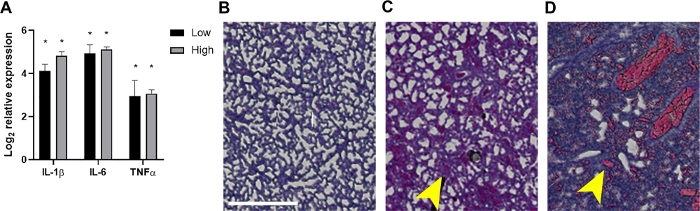
Figure 4: Inflammation and associated histopathological findings in the lungs of septic neonates.
At 24 hpi the lungs were harvested from pups that received ~2 x 106 or 7 x 106 CFUs or uninfected controls. (A) RNA was isolated and the expression of IL-1β, IL-6, or TNF-α as determined relative to uninfected controls by quantitative real-time PCR using the formula 2-ΔΔCt. The data is shown as the mean log2 transformed change in expression ± SEM for each inoculum as indicated. Statistical significance was determined using unpaired t-tests of ΔCt values between individual cytokine genes and the internal control in the 95% confidence interval. Asterisks indicate p<0.01. (B-D) Histopathologic sections of H&E stained lung tissues (20x, area of interest constructed into clipping mask and enlarged for clarity) are shown. Lung tissues from a representative uninfected control (B) or infected neonate at the low (C) or high (D) inoculum are shown. Yellow arrows indicate alveolar thickening (C) or hemorrhaging (D). Scale bar = 500 μm. Please click here to view a larger version of this figure.
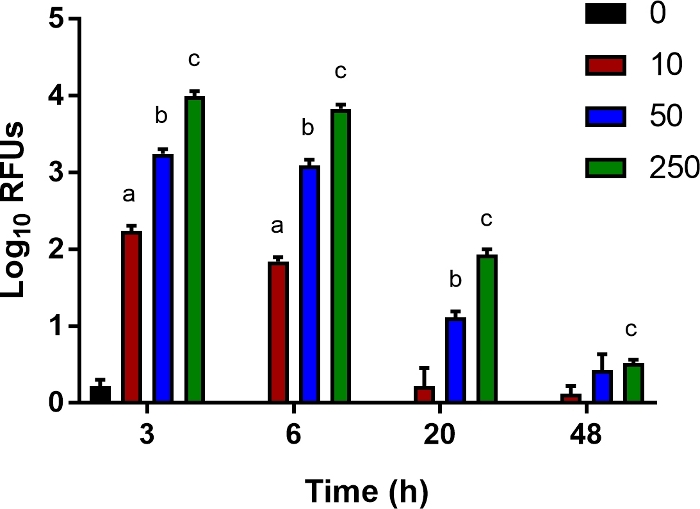
Figure 5: An in vitro assay for bacterial clearance.
Ly6B.2+ cells were isolated from the spleens of uninfected control neonates. Cells were seeded in 96-well plates and infected with luciferase-expressing E. coli O1:K1:H7 at a multiplicity of infection (MOI) of 10, 50, or 250 as indicated. After 1 h, the medium was replaced with fresh that contained gentamicin (100 µg/mL). Mean relative light units (RLU) ± SE for an individual experiment representative of multiple are shown. Statistical significance in the 95% confidence interval was determined using unpaired t tests with Welch’s correction; asterisks indicate p<0.05. Please click here to view a larger version of this figure.
