The experiments outlined in this protocol were carried out using the attenuated H37Ra strain of Mtb, which can be handled in a Containment Level 2 laboratory. All manipulations of live mycobacteria were carried out in Class II biological safety cabinet (BSC). Experimental procedures were designed to minimize the generation of aerosols. Eukaryotic cell culture (THP-1 cells) was also carried out in a Class II BSC. The laboratory carried out a risk assessment and ensured that all procedures were carried out in line with institutional and national biological safety regulations. The human monocytic THP-1 cell line was used to perform the method as described (step 1). Cells are differentiated into macrophages following stimulation with phorbol 12-myristate 13-acetate (PMA) before infection with mycobacteria.
1. Cell culture
- Propagate H37Ra seed stock to log phase in Middlebrook 7H9 (MB) broth supplemented with albumin-dextrose-catalase (ADC) enrichment (10%) and 0.05% polysorbate 80. Store H37Ra stock in 1 mL aliquots in a -80 °C freezer for up to 1 year.
- Thaw a 1 mL vial of Mtb-H37Ra and transfer it to a T25 flask with a filter cap containing 9 mL of MB supplemented broth approximately 1 week before the planned experiment. Incubate at 37 °C for 5-7 days in a static incubator.
- Grow THP-1 cells in RPMI-1640 supplemented with non-heat killed 10% fetal calf serum (complete (c)RPMI) in a T75 flask in a CO2 humidified incubator at 5% CO2/37 °C and subculture twice per week to maintain a density of less than 1 x 106 cells/mL.
- Differentiate THP-1 cells into macrophages 3 days before infection by gently pipetting cells several times using a serological pipette in T75 flasks to disperse any clumps and place them in a 50 mL conical tube.
- Centrifuge cells at 300 x g for 10 min at room temperature, decant off the supernatant, and gently resuspend the pellet in 2 mL of RPMI. Perform cell count to estimate cells/mL.
- Seed 2 mL of THP-1 macrophages in 12-well tissue culture plates at a density of 100,000 cells/mL in cRPMI with 100 ng/mL PMA for 72 h. Remove PMA-containing medium from cells and replenish with fresh cRPMI before Mtb infection.
- Set up individual plates for each time point required.
- Seed cells at the same density (100,000 cells/mL) in 2-well glass chamber slides to determine the multiplicity of infection (MOI).
- Place in a 5% CO2 humidified incubator for 3 days at 37 °C.
2. Quantification of Mtb uptake
- Determination of Mtb uptake by macrophages (MOI)
- Set up the Class II biological safety cabinet (BSC) on the day of infection and work on two layers of tissue paper to catch any spills. Set up waste discard containers according to local regulations.
- Remove 6-8 mL of mycobacterial culture from the T25 flask and transfer it into a 15 mL polypropylene tube.
NOTE: Smaller volume tubes can be used for smaller experiments. - Centrifuge the tube in a benchtop centrifuge at room temperature for 10 min at 2890 x g.
- Carefully remove the tube from the centrifuge and transfer it to the biological safety cabinet. Wait 1 min to allow the bacteria to settle.
- Pour off the supernatant into the disinfectant discard container, recap tube, and resuspend the bacteria in the remaining medium by tapping the side of the tube. Wait 1 min to allow the bacteria to settle.
- Add 2 mL of pre-warmed cRPMI, mix gently, and transfer to a 50 mL conical tube.
- Resuspend the mycobacteria very carefully using a 25 G needle and 5 mL syringe. To resuspend, draw up the mycobacteria suspension into the syringe and eject very gently down the sidewall of the tube to minimize aerosol production. Repeat 6-8 times.
NOTE: Exercise utmost caution as this is a high-density culture of mycobacteria. To avoid the risk of needle stick injury, use blunt needles where possible, and Luer lock syringes. - Dispose of the needle and syringe in a sharps container in the BSC.
- Transfer the suspension to a 2 mL microfuge tube (with screw-on cap) and centrifuge at room temperature for 3 min at 100 x g to pellet any remaining clumps. Return the tube to the safety cabinet and wait 1 min to allow the bacteria to settle.
- Transfer the top 1-1.5 mL of the supernatant to a new tube. Discard the original tube in the waste bucket containing disinfectant. Mix well and add various amounts of the mycobacterial suspension (e.g., 5, 25, 50, 150 µL) to the 2-well glass chamber slides and incubate for 3 h in a CO2 incubator at 37 °C.
- Staining for acid fast bacteria (AFB)
NOTE: After 3 h incubation, the macrophages are washed and fixed with paraformaldehyde to inactivate mycobacteria. The slides are then stained using a Modified Auramine O kit (see Table of Materials) to estimate mycobacteria phagocytosed per cell. Due to their waxy cell wall, mycobacteria retain the Auramine dye after an acid-alcohol wash. The macrophage nuclei are then counter-stained with Hoechst. This method allows for the number of phagocytosed bacteria per cell to be counted and is used to determine the multiplicity of infection (MOI) of the macrophages.- Remove the medium from the glass chamber slide after pipetting up and down three times to dislodge bacteria that have not been phagocytosed.
- Wash once with 2 mL of room temperature PBS.
- Store stocks of 4% paraformaldehyde, dissolved in PBS in aliquots at -20 °C for up to 6 months. Thaw an aliquot of 4% paraformaldehyde immediately before use. Dilute to 2% paraformaldehyde with PBS and add 2 mL per well.
- Incubate for 10 min at room temperature. The glass chamber slide can be removed from the safety cabinet at this stage for staining.
- Wash the slide under a gentle stream of tap water.
- Dispense enough Auramine onto the slide to cover the cells using a plastic transfer pipette and incubate for 1 min at room temperature in the dark (cover with aluminum foil).
- Wash excess dye off the slide with tap water and add the decolorizer/quencher for 1 min in the dark.
- Wash off the excess with tap water and incubate for 15 min at room temperature with Hoechst 33342 (10 µg/mL in PBS) in the dark.
- Wash off the Hoechst stain with tap water, remove the chambers, drain excess water from the slide, add a drop of antifade and coverslip, and air dry.
- Examine the slide under the fluorescent microscope using the 100x oil objective. Mycobacteria will fluoresce green under the FITC filter. The nuclei fluoresce blue under the DAPI filter (Figure 1C).
- Determine the MOI by counting the number of mycobacteria phagocytosed per cell and the percentage of cells infected.
- Calculate the volume of mycobacterial suspension needed to achieve the required MOI based on the surface area of a well in the plate; for example, the surface area of the glass chamber slides used in this experiment is 4 cm2. Low MOI (approximately 1-2 bacilli/cell) is desirable for experiments conducted over several days (e.g., 5 days).
- Infection of macrophages
- Mix the mycobacteria suspension well and add the amount needed to the cells on 12-well plates once the volume required to achieve the desired MOI has been determined.
- Incubate at 37 °C for 3 h to allow mycobacteria to be phagocytosed.
- Remove extracellular bacteria by washing the wells with either warm RPMI or HBSS several times.
- Lyse the macrophages in one well (3 h sample) to determine the percentage time to positivity (TTP) of the initial inoculum (3 h sample) as outlined in step 3 below.
- Add fresh cRPMI and the required drug doses or vehicle control to the remaining wells, incubate the plates in the CO2 incubator at 37 °C for the time necessary (dependent on the experimental design but usually at several intervals between 1 to 8 days).
3. Harvesting samples for the liquid culture detection system
NOTE: On the day of infection, extracellular mycobacteria are removed by washing, and intracellular mycobacteria are harvested by lysis of one well of macrophages (3 h sample) to determine the initial amount phagocytosed as a baseline control for infection. At subsequent times both the medium, cell lysate, and washes are combined to measure total mycobacterial growth. Extracellular and intracellular growth can also be assessed separately if desired.
- Harvesting 3 h sample to determine TTP
- Wash off extracellular mycobacteria from all the wells after the initial 3 h of infection as outlined in step 2.3.3. Add 1 mL of fresh media to the 3 h control well to equalize the lysate volume with those of later time points.
NOTE: See step 3.2.7 if extracellular mycobacteria are to be excluded from the analysis.
- Wash off extracellular mycobacteria from all the wells after the initial 3 h of infection as outlined in step 2.3.3. Add 1 mL of fresh media to the 3 h control well to equalize the lysate volume with those of later time points.
- Sample collection
- Warm MB broth and instrument culture bottles to bring them to room temperature.
- Transfer the medium from the 12-well plate to the corresponding labeled conical tubes.
- Add 500 µL of sterile lysis buffer (0.1% Triton x-100 in PBS filtered through a sterile 0.2 µm filter) to each well for 10 min.
- Gently scrape the cells from the well with a sterile scraper and combine with the medium in the appropriate conical tube.
- Wash the well with 0.5 mL of sterile PBS and transfer to the appropriate tube.
- Gently pass each sample through a needle and syringe (25 G) 6-8 times to break up the clumps. Dilute samples 1:10 in MB broth; 100 µL sample + 900 µL MB medium.
- At the required times/days (usually between 1 to 8 days), harvest the remaining samples by following steps 3.2.1-3.2.6 above.
NOTE: Investigators may prefer to exclude extracellular mycobacteria from their analysis, in which case, in step 3.2.2 above, the medium from each well is discarded, and macrophages are washed several times before adding lysis buffer.
- Inoculating and loading instrument culture bottles
NOTE: Details of the liquid culture instrument and related consumables are provided in the Table of Materials.- Sterilize the rubber cap of the instrument culture bottle with tissue paper soaked in 70% alcohol and allow it to air dry.
NOTE: This step needs to be carried out in the BSC. - Prepare bottles by transferring enough Nutrient supplements for all the samples into a conical tube (0.5 mL/bottle). Use a needle and syringe to inject 0.5 mL of Nutrient supplement into the instrument culture bottle.
- Pipette 500 µL of the diluted sample (1:10) into a 1 mL V-bottomed tube.
- Use a needle and syringe to inject the 500 µL of sample into the assigned instrument culture bottle.
- Sterilize the rubber cap of the instrument culture bottle with tissue paper soaked in 70% alcohol and allow it to air dry. Wipe the bottles with tissue paper soaked in 70% alcohol before removal from the BSC.
- Carefully transport bottles from the biosafety cabinet to the instrument for loading.
- Press the loading button on the automated microbial detection system.
- Scan the barcodes on instrument culture bottles and place the bottles into the detection system incubator at 37 °C for up to 42 days. Read and record the time taken to reach positivity from the instrument screen.
NOTE: The barcode allows the instrument to identify the bottle and link reflectance readings with a particular bottle. - Calculate percentage time to positivity (TTP) by comparing the TTP of the initial intracellular inoculum (Day 0) to that of macrophages cultured for the indicated times. A positive change in percentage TTP means mycobacterial growth13.
For example, for day 3:
Percentage change in time to positivity =
- Sterilize the rubber cap of the instrument culture bottle with tissue paper soaked in 70% alcohol and allow it to air dry.
The automated liquid culture instrument used in this study monitors CO2 levels every 10 min. A color change in the sensor at the bottom of the instrument bottle is measured colorimetrically and expressed as reflectance units. The instrument software then applies detection algorithms to calculate time to positivity (TTP), i.e., the number of days from inoculation until cultures are flagged as positive (Figure 1A). An inverse relationship between TTP and log10CFU (determined by the agar plate method)12 in the initial inoculum is illustrated in Figure 1B. When Mtb growth within macrophages-infected at MOI ranging from 1-2 to 5-10 in the presence or absence of pharmacological inhibitors (Figure 1C) was compared by the automated culture method described or by enumeration of colonies on solid agar, there was a significant correlation between results obtained by both methods (Figure 1D). To display Mtb growth graphically, the percentage change in TTP was calculated according to the equation above by comparing the TTP values for up to 8 days after infection of macrophages to the initial TTP value12. Results demonstrated a similar trend between liquid culture and CFU, showing significant inhibition of Mtb growth in macrophages in the presence of AtRA in solution or the equivalent dose of AtRA encapsulated in PLGA microparticles (MP) (Figure 2A,B).
The efficacy of another HDT, IFNγ, which has been used to treat multi-drug resistant TB14, in combination with the second-line antibiotic linezolid, was also investigated. A dose-response experiment was first carried out in infected THP-1 cells to determine the efficacy of linezolid alone at concentrations ranging from 0.6-5.0 µg/mL (Figure 2C) before the combination of linezolid at a suboptimal dose (1.25 µg/mL) and IFNγ was tested: there was no significant interaction between the drugs (Figure 2D).
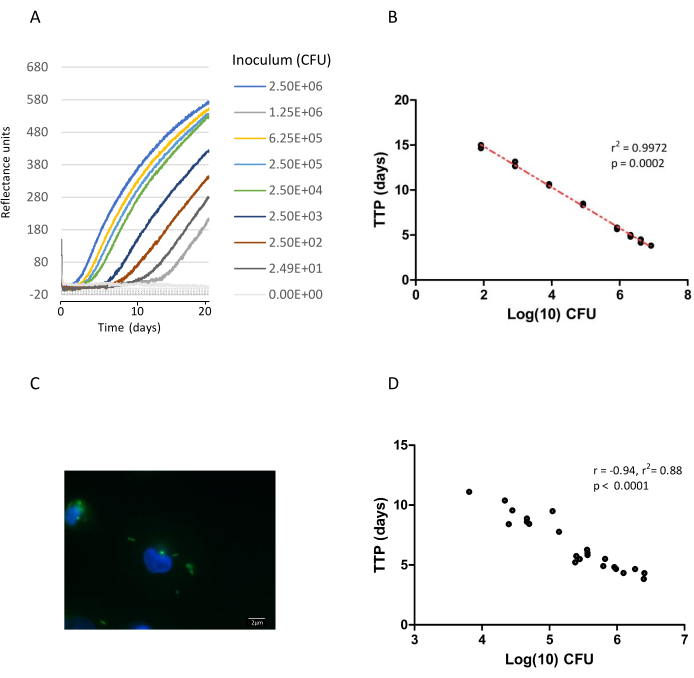
Figure 1: Quantification of Mtb growth by automated liquid culture and on solid medium. Mtb H37Ra was diluted in Middlebrook broth over a range of dilutions (1:2 to 1:100,000). A 300 µL aliquot of each dilution was injected into duplicate instrument culture bottles, incubated on the liquid culture instrument, and their growth was monitored. Simultaneously, an aliquot (10 µL) was spread on MB agar plates containing 0.5% glycerol and 10% OADC (Oleic acid, albumin, dextrose, catalase supplement) in triplicate, for CFU enumeration as previously published12. (A) Data points from the liquid culture system of each dilution are plotted as reflectance units versus time15. To allow for comparisons between samples, the background was normalized to the 9 h reflectance reading for each sample. Growth was monitored for 42 days in all (the first 21 days is shown on graph), time to positivity (TTP) ranged from 3.83 to 11.1 days. (B) TTP from diluted samples was plotted against log10 CFU estimation; each data point represents the values for two replicates from one experiment and describes two separate experiments. The line of best fit and regression coefficient (r2) are shown. (C) Example of AFB staining of intracellular Mtb H37Ra in THP-1 macrophages with auramine (green) which is used to calculate multiplicity of infection, nuclei are counterstained with Hoechst 333258 (blue). Images were generated using an Epifluorescent Microscope with a 100x (numerical aperture [NA], 1.3) oil objective. Scale bar represents 2 µm. (D) Correlation analysis (Pearson) of paired TTP (liquid culture) and CFU estimation of Mtb H37Ra growth in THP-1 macrophage lysates from multiple experiments (n = 23), treated with/without pharmacological reagents and infected at MOI ranging from 1-2 to 5-10 bacilli/infected macrophage. Please click here to view a larger version of this figure.
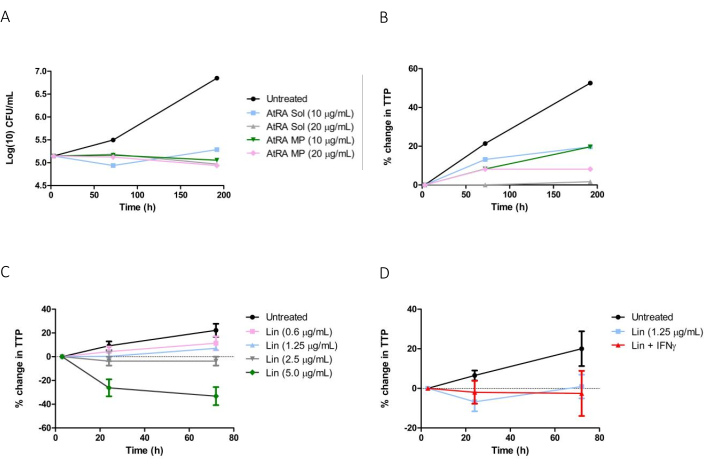
Figure 2: Evaluation of host-directed therapies for TB using an automated liquid culture system. THP-1 macrophages were infected with Mtb H37Ra for 3 h, extracellular bacteria were removed, and cells were treated with candidate host-directed therapies for up to 192 h. (A) CFU estimation of Mtb growth in macrophages treated with AtRA solution (Sol) or 2 µM AtRA microparticles (MP) (10-20 µg/mL). (B) % change in (time to positivity TTP) in macrophages treated with AtRA solution or AtRA PLGA MP. Infected THP1 cells cultured in 0.1% DMSO in cRPMI were designated as untreated controls. (C) Macrophages were treated with increasing concentrations of linezolid solution (0.6 µg/mL to 5 µg/mL), % change in TTP was determined 24 and 72 h post-infection using an automated liquid culture system. (D) Macrophages infected with Mtb H37Ra were treated with linezolid alone (1.25 µg/mL) or linezolid + IFNγ (5 ng/mL) up to 72 h, % change in TTP was calculated. Untreated controls consisted of infected THP1 cells cultured in cRPMI alone for the indicated times. Please click here to view a larger version of this figure.
